

Abstract
The built and natural environment can facilitate (un)healthy behaviors in adolescence. However, most previous studies have focused on examining associations between singular aspects of the environment. This study examined the association between the mixture of health‐promoting and health‐constraining environmental features in a Healthy Location Index (HLI) and physical activity and screen time among adolescents. This cross‐sectional study used data from the Built Environment and Active Transport to School (BEATS) Research Program based in Dunedin, New Zealand. Data from 1,162 adolescents with complete demographic, health behavior and spatial records were included in the analysis. The environment was defined using the HLI based on access to health‐promoting (e.g., greenspace, blue space, physical activity facility) and health‐constraining (e.g., fast‐food outlets) features and their mixture. Quantile g‐computation and multilevel mixed effects models, with adolescents nested within schools, examined associations between the environment and the two health behaviors. A positive association existed between meeting physical activity guidelines and access to health‐promoting environments (OR = 1.23 [95% CI 1.03; 1.47]), particularly blue space. In addition, the mixture of health‐promoting and health‐constraining environments was also important (ψ = 1.18 [1.01; 1.37]). However, there was limited evidence of an association between the environment and screen time. We provide evidence of a relationship between health‐promoting environments, the mix of health‐promoting and health‐constraining environments, and physical activity among adolescents. The findings support the hypothesis that the environment has the potential to positively influence healthy behaviors of youth, particularly when it comes to physical activity.
Keywords: adolescents, environmental mixture, geospatial, multilevel modeling, physical activity, built environment
Key Points
Combined evaluation of health‐promoting and health‐constraining features of the environment in the study of 1,162 high‐school students
Access to health‐promoting features of the environment impacts physical activity but not sedentary behavior
A mixture of health‐promoting and health‐constraining environments affects adolescents' physical activity
1. Introduction
Though engagement in physical activity and reduced sedentary behavior is associated with positive physical and mental health in youth (Bull et al., 2020), a majority of youth do not meet physical activity and sedentary behavior guidelines globally (Aubert et al., 2022; Guthold et al., 2020). Patterns of physical activity and sedentary behavior vary internationally by the level of social and economic development of a country, geo‐cultural region, and additional contextual factors such as negative impacts of war and climate change (Aubert et al., 2022). In this context, Aotearoa New Zealand (NZ) has a relatively supportive environment for physical activity—with a very high social and economic development, political stability, and a generally temperate climate. Yet only 58% of children and youth meet overall physical activity guidelines in NZ, and 43% meet screen time recommendations (Wilson et al., 2023). Specifically, rates of meeting physical activity guidelines are significantly lower for older adolescents (aged ∼15–17 years; 19%) compared with children (46%) and younger adolescents (36%) (Wilson et al., 2023). Only 12% of older adolescents meet screen time recommendations, compared with 36% of younger adolescents, and 61% of children (Wilson et al., 2023). More recently, a regional study in Otago (NZ) revealed less than a quarter (23%) of adolescents aged 13–18 years met physical activity guidelines and 18% met screen time recommendations in 2021/22 (Mandic et al., 2024).
To address low levels of physical activity and high screen time among adolescents, it is important to identify the antecedents and correlates most related to these behaviors. According to a review of reviews (Sterdt et al., 2014), the physical activity of children and youth is influenced by a range of factors categorized as demographic (e.g., sex, age, socioeconomic status), psychological (e.g., perceived competence, self‐efficacy), behavioral (e.g., participation in community sports), social/cultural (e.g., parental support, support from significant others), and the physical environment (e.g., access to sport/recreational facilities, time spent outdoors). Likewise, research has identified several modifiable factors at the individual (e.g., self‐efficacy toward limiting computer/electronic game use), interpersonal (e.g., parental modeling of TV and movie streaming) and neighborhood environmental (e.g., perceived opportunities for physical activity in the neighborhood) levels as potential targets for interventions aimed at reducing screen time among adolescents (Gebremariam et al., 2020; Stiglic & Viner, 2019). Ecological models of physical activity suggest that it is an interplay of these multiple factors at various levels over time that supports or limits physical activity, with an emphasis on the role of external factors such as the built environment and policies (Spence & Lee, 2002). In the case of the former, evidence of consistent associations has been noted for active transportation of children and youth, supportive infrastructure (e.g., dedicated bike lanes) and streetscapes, and total physical activity (Prince et al., 2022). Less consistent associations were found for other aspects of the environment (e.g., greenspace, street lighting, traffic safety) and various domains of physical activity. Similarly, ecological models recognize that sedentary behavior (e.g., consuming screen time while sitting, sitting during transportation) is context‐specific and heavily influenced by proximal environments (Hadgraft et al., 2023).
Objective assessment of environmental features is of value when producing evidence for policymakers and practitioners, enabling the alignment of measures with those used in practice (e.g., using geographic information systems [GIS] to derive measures of land use). However, the heterogeneity in objective environmental measures used (and their reporting) in relation to physical activity has hindered a comprehensive understanding of the array of features of importance (Smith et al., 2021). Examples include focusing on a singular measure of interest (e.g., park availability), indices addressing one environmental aspect only (e.g., walkability), and a limited focus on environmental features that may play distinct roles in hindering health behaviors (i.e., health constraining factors). Emergent research has revealed the co‐occurrence of both health‐promoting and health‐constraining environmental factors in NZ (Marek et al., 2021), further highlighting the complexity of understanding the links between environments and physical activity. However, studies that attempt to account holistically for the effects of combinations of relevant environmental exposures, instead of using the traditional approach that focuses on examining the effects of singular aspects of the environment, are lacking in the literature.
The primary purpose of this study was to examine the association between the mixture of health‐promoting and health‐constraining environmental features and physical activity of adolescents residing in Dunedin (NZ). A second purpose was to examine the association between the mixture of health‐promoting and health‐constraining environmental features and screen time among these same adolescents.
2. Materials and Methods
2.1. Data
This study involves a cross‐sectional secondary analysis of data from the Built Environment and Active Transport to School (BEATS) Study conducted in Dunedin, NZ in 2014–2015 (Mandic et al., 2015). The BEATS Research Program examined individual, social, environmental and policy influences on adolescents’ active transport (e.g., walking, cycling) to school. Details on the development of the research and community collaborations, planning and study implementation are described elsewhere (Mandic et al., 2015, 2016). Briefly, the BEATS Study was an observational cross‐sectional study that used a multimethod approach incorporating both quantitative methods (i.e., surveys, anthropometry, accelerometers, GIS analysis, and mapping) along with qualitative methods such as focus groups and interviews. The study gathered a range of data from students, parents, teachers, and school principals. Measures specific to this study are outlined below. The University of Otago Ethics Committee approved this study (Ref: 13/203).
2.2. Setting
The BEATS Study was conducted in Dunedin, a coastal city located on the lower South Island of NZ, with a population of approximately 128,000 people.
2.3. Participants, Procedures, and Measures
Participants included 1,780 adolescents aged 13–18 years from all 12 secondary schools in the city. Data collection was carried out during 2014–2015 (4,232 adolescents invited; 42% participation rate).
The adolescents completed an anonymized 30–40‐min online questionnaire during school time, under the supervision of research staff. The questionnaire included sociodemographic characteristics, school characteristics, as well as health behaviors (e.g., self‐reported physical activity and screen time). All participating adolescents provided written consent and for those aged <16 years, parents signed either a parent opt‐out or parental opt‐in consent based on each school's preference. Those with invalid surveys (n = 38), incomplete student consents (n = 20), no required parental consent (n = 59), missing data (n = 363) or missing addresses (n = 142) were excluded. Participants with missing data were similar in socioeconomic status and weight status but were slightly younger and with a greater proportion of girls (Mandic et al., 2017).
2.4. Sociodemographic Characteristics and Health Behaviors
Socioeconomic, demographic, spatial data (environmental exposures excluded), and health behaviors included in the analyses were the date of birth, sex, ethnicity, school, home address area‐level deprivation, and home address.
Age was calculated from the date of birth at the time of the survey. Sex was self‐reported as “male” or “female.” Ethnicity was categorized into five groups: Māori (indigenous population of NZ), Pacific Peoples, Asian, NZ European, and Other. Respondents could select more than one ethnicity—in these instances, prioritized ethnic grouping was used, in the following order: Māori, Pacific Peoples, Asian, Other, NZ European (Ministry of Health, 2004). The New Zealand Index of Deprivation (NZDep2018), an area‐based measure of socioeconomic deprivation, was used as a proxy for participants' socioeconomic position (Atkinson et al., 2020). The index is based on nine Census variables and the final score was categorized into quintiles (Q1—least deprived to Q5—most deprived). The deprivation quintiles were assigned to participants based on their home address. The school the adolescent attended was also recorded.
Physical activity was assessed using the question “Over the past 7 days, on how many days were you physically active for a total of at least 60 min per day?” (Currie et al., 2009). Those who self‐reported participating in ≥60 min of moderate‐to‐vigorous physical activity every day were categorized as meeting physical activity guidelines. Screen time outside of school was assessed using the questions “About how many hours a day do you usually watch television/play games on a computer or games console/use a computer for chatting online, Internet, emailing, homework etc. in your free time?” for weekdays and weekend days separately. Total weekly screen time was calculated by combining the estimates on weekdays and weekends and ≤2 hr of screen time per day was a threshold to identify meeting screen time guidelines.
2.5. Defining Environmental Exposure
Exposure to environments was estimated using the components of the existing Healthy Location Index (HLI) that is available at a meshblock level (the smallest statistical geographic unit of about 30–60 dwellings (around 60–120 residents) (Statistics New Zealand, 2019) for each area in NZ (Marek et al., 2021)). The HLI is a composite measure based on the accessibility of five health‐promoting features (i.e., supermarkets, fruit and vegetable stores, physical activity facilities, greenspace, and blue space) and five health‐constraining features (i.e., fast food outlets, takeaways, dairies, alcohol outlets, gaming venues) of the built environment (Marek et al., 2021). However, in this study, we do not use gaming venues and alcohol outlets as individual domains because most participants were not of the age to legally use these premises in NZ. The HLI can be used as one index accounting for the co‐occurrence of these environments, further broken down into either health‐promoting and health‐constraining environments, or the individual domains can be deployed. While HLI is a nationwide measure, available data contain distances, ranks and deciles that can be used for the creation of local‐specific indices. In this study, we combined deciles of health‐promoting, health‐constraining, and individual domains into quintiles and assigned them to every participant using their home address.
2.6. Statistical Analyses
Descriptive statistics of the cohort are presented as frequencies/counts and percentages for all variables except age, which is presented as the median and interquartile range (IQR). Five adolescents with missing complete ethnicity information were excluded from the further modeling. Multilevel mixed effects logistic regression models with adolescents nested within schools were constructed to investigate associations between environments where adolescents lived and whether they met weekly physical activity and screen time guidelines. The focus of the analysis was on the effect of the health‐promoting and health‐constraining environments represented by quintiles derived from HLI. Models were adjusted for additional variables (age, sex, ethnicity, and area‐level socioeconomic deprivation). The associations resulting from the final models are presented as odds ratios (OR) with 95% confidence intervals and associated p‐values. Quintiles of health‐promoting and health‐constraining environmental features were treated as continuous variables in alignment with the requirements of quantile g‐computing modeling. In this way, we assume that differences between individual environmental quintiles are constant. An alpha level of 0.05 was employed for the determination of statistical significance.
The same approach as in multilevel mixed effects logistic regression models was used to identify important individual domains of HLI associated with meeting physical activity and screen time guidelines. However, instead of combined health‐promoting and health‐constraining environments, we explored quintiles of access to each of health‐promoting and health‐constraining environments (Q1—least accessible/Q5—the most accessible). Again, analyses were adjusted for age, sex, prioritized ethnicity, and socioeconomic deprivation.
As health‐promoting and health‐constraining environmental features are often co‐located in space, quantile g‐computation was employed to analyze the combined effect of a mixture of both exposures. Unlike inferential approaches that examine the effects of individual exposures while holding other exposures constant, methods like quantile g‐computation that can estimate the effect of a mixture are essential for understanding the effects of potential public health actions that act on exposure sources (Keil et al., 2020). Quantile g‐computation yields estimates of the effect of increasing all exposures by one quantile simultaneously and by that it estimates a mixture effect ψ (Letellier et al., 2022) useful in the studies where combined exposures are considered. The approach estimates a regression line corresponding to the expected change in the outcome (on the link basis) given a simultaneous increase in the quantile‐based category for all exposures conditional on confounders (Keil, 2023). Details of the method can be found elsewhere (Keil et al., 2020; Robins, 1986).
Quantile g‐computation can be used with automatic or user‐generated quantiles. We employed user‐generated quintiles created by combining health‐promoting and health‐constraining deciles available in the HLI (Q1—least accessible/Q5—the most accessible). For both outcomes (physical activity and screen time), we applied quantile g‐computation with bootstrapping based on the logistic regression model with clustering of adolescents in their schools. The health‐promoting and health‐constraining features are considered exposures while additional confounders are identical to the multilevel mixed‐effect model. The results of the underlying clustered logistic model are comparable to the multilevel mixed effects logistic regression model. A mixture analysis of individual domains was not conducted as their mixture is captured by health‐promoting and health‐constraining environments.
3. Results
3.1. Descriptive Statistics
Among 1,162 adolescents in this analysis, 601 (52%) were female, 124 (11%) were Māori, 40 (3.5%) Pacific Peoples, and 77 (6.7%) Asian. Their median age was 15.1 (IQR: 14.0, 16.5) years. A higher proportion of participants lived in less deprived areas (Q1 + Q2: 648 (55%)) than in more deprived areas (Q4 + Q5: 335 (29%)). Participants lived mostly in areas with access to both health‐promoting and health‐constraining environmental features. Only 81 (7%) lived in the areas with the worst access to health‐promoting environments and 131 (11%) lived in the areas with the worst access to health‐constraining environments. More details on the cohort and their health behaviors are presented in Table 1.
Table 1.
Participants' Characteristics
| Overall N = 1,162 a | Physical activity guideline | Screen time guideline | |||
|---|---|---|---|---|---|
| Met N = 200 a | Not met N = 962 a | Met N = 150 a | Not met N = 1,012 a | ||
| Age | 15.06 (14.00, 16.47) | 15.00 (14.22, 16.22) | 15.08 (13.97, 16.50) | 14.38 (13.55, 15.31) | 15.15 (14.11, 16.55) |
| Sex | |||||
| Male | 561 (48.3%) | 130 (23.2%) | 431 (76.8%) | 63 (11.2%) | 498 (88.8%) |
| Female | 601 (51.7%) | 70 (11.6%) | 531 (88.4%) | 87 (14.5%) | 514 (85.5%) |
| Ethnicity | |||||
| NZ European | 858 (73.8%) | 147 (17.1%) | 711 (82.9%) | 118 (13.8%) | 740 (86.2%) |
| Māori | 124 (10.6%) | 32 (25.8%) | 92 (74.2%) | 11 (8.9%) | 113 (91.1%) |
| Pacific Peoples | 40 (3.4%) | 4 (10.0%) | 36 (90.0%) | 6 (15.0%) | 34 (85.0%) |
| Asian | 77 (6.6%) | 8 (10.4%) | 69 (89.6%) | 10 (13.0%) | 67 (87.0%) |
| Other | 58 (5.0%) | 7 (12.1%) | 51 (87.9%) | 5 (8.6%) | 53 (91.4%) |
| Unknown | 5 (0.04%) | 2 (40.0%) | 3 (60.0%) | 0 (0.0%) | 5 (100.0%) |
| Deprivation (quintile) | |||||
| 1 (least deprived) | 316 (27.2%) | 54 (17.1%) | 262 (82.9%) | 34 (10.8%) | 282 (89.2%) |
| 2 | 324 (27.9%) | 64 (19.8%) | 260 (80.2%) | 47 (14.5%) | 277 (85.5%) |
| 3 | 187 (16.1%) | 32 (17.1%) | 155 (82.9%) | 23 (12.3%) | 164 (87.7%) |
| 4 | 219 (18.8%) | 36 (16.4%) | 183 (83.6%) | 32 (14.6%) | 187 (85.4%) |
| 5 (most deprived) | 116 (10.0%) | 14 (12.1%) | 102 (87.9%) | 14 (12.1%) | 102 (87.9%) |
| Health‐promoting environment (quintile) | |||||
| 1 (worst access) | 81 (7.0%) | 14 (17.3%) | 67 (82.7%) | 11 (13.6%) | 70 (86.4%) |
| 2 | 246 (21.2%) | 33 (13.4%) | 213 (86.6%) | 36 (14.6%) | 210 (85.4%) |
| 3 | 297 (25.6%) | 48 (16.2%) | 249 (83.8%) | 31 (10.4%) | 266 (89.6%) |
| 4 | 294 (25.3%) | 52 (17.7%) | 242 (82.3%) | 37 (12.6%) | 257 (87.4%) |
| 5 (best access) | 244 (21.0%) | 53 (21.7%) | 191 (78.3%) | 35 (14.3%) | 209 (85.7%) |
| Health‐constraining environment (quintile) | |||||
| 1 (worst access) | 131 (11.3%) | 20 (15.3%) | 111 (84.7%) | 31 (23.7%) | 100 (76.3%) |
| 2 | 206 (17.7%) | 34 (16.5%) | 172 (83.5%) | 17 (8.3%) | 189 (91.7%) |
| 3 | 291 (25.0%) | 52 (17.9%) | 239 (82.1%) | 29 (10.0%) | 262 (90.0%) |
| 4 | 272 (23.4%) | 48 (17.6%) | 224 (82.4%) | 38 (14.0%) | 234 (86.0%) |
| 5 (best access) | 262 (22.5%) | 46 (17.6%) | 216 (82.4%) | 35 (13.4%) | 227 (86.6%) |
Median (IQR); N (%); Percentages (%) for Overall calculated by individual groups, percentages (%) for guidelines calculated by rows.
3.2. Associations Between the Health‐Promoting and Health‐Constraining Environmental Features and Physical Activity and Screen Time
As shown in Figure 1 most participants did not meet physical activity and screen time guidelines. However, those who met physical activity guidelines resided in areas with slightly better access to health‐promoting environments.
Figure 1.
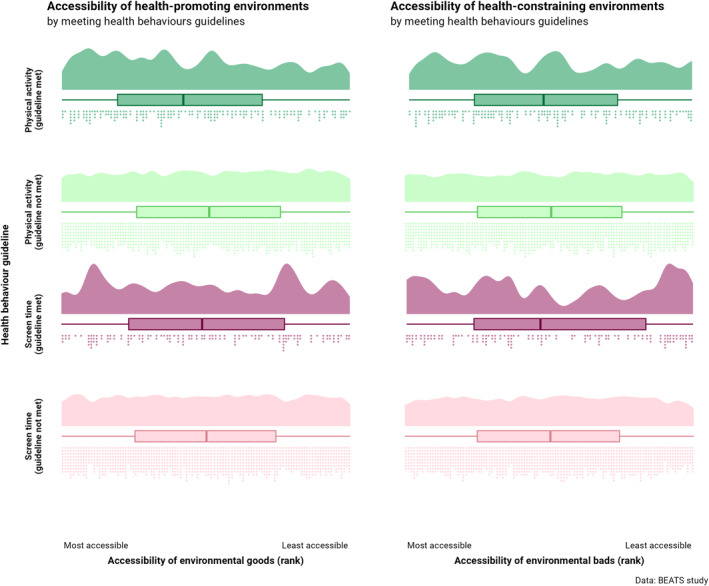
Distribution of adolescents and their health behaviors within health‐promoting and health‐constraining environments. Dots represent individuals and HLI accessibility rank.
The likelihood of meeting physical activity guidelines was associated with accessibility to health‐promoting environments with a one‐quintile increase in accessibility to such environments resulting in a 1.23 [95% CI 1.03, 1.47] increase in the likelihood that adolescents met the physical activity guidelines (Table 2). Even though no association existed between health‐constraining features of the environment and the likelihood of meeting the physical activity guidelines, the mixture of health‐promoting and health‐constraining environments was statistically significant (ψ = 1.18 [1.01; 1.37]). Additionally, females (OR = 0.45 [0.30, 0.67]) and Asian (OR = 0.45 [0.21, 0.98]) adolescents were less likely to meet the physical activity guidelines when compared to males and NZ European adolescents, respectively. Adolescents of Māori ethnicity were more likely (OR = 1.77 [1.12, 2.82]) to meet the physical activity guidelines than NZ European adolescents.
Table 2.
Findings From Multilevel Mixed Effects Models (Adolescents Nested in Schools) and Quantile g‐Computation Models Examining Associations Between the Environment and Meeting the Guidelines for Physical Activity and Screen Time
| Physical activity guideline | Screen time guideline | |||||
|---|---|---|---|---|---|---|
| OR a | 95% CI a | p‐value | OR a | 95% CI a | p‐value | |
| Health‐promoting environment (quintile) | 1.23 | 1.03, 1.47 | 0.02 | 1.13 | 0.93, 1.38 | 0.23 |
| Health‐constraining environment (quintile) | 0.95 | 0.80, 1.13 | 0.56 | 0.84 | 0.69, 1.02 | 0.08 |
| Age | 0.96 | 0.86, 1.07 | 0.46 | 0.71 | 0.62, 0.82 | <0.001 |
| Sex | ||||||
| Male | Reference group | Reference group | ||||
| Female | 0.45 | 0.30, 0.67 | <0.001 | 1.18 | 0.76, 1.83 | 0.47 |
| Ethnicity | ||||||
| NZ European | Reference group | Reference group | ||||
| Māori | 1.77 | 1.12, 2.82 | 0.02 | 0.56 | 0.28, 1.08 | 0.08 |
| Pasifika | 0.52 | 0.18, 1.52 | 0.23 | 0.92 | 0.36, 2.34 | 0.86 |
| Asian | 0.45 | 0.21, 0.98 | 0.04 | 0.98 | 0.47, 2.02 | 0.95 |
| Other | 0.63 | 0.28, 1.45 | 0.28 | 0.64 | 0.25, 1.68 | 0.36 |
| Deprivation (quintile) | ||||||
| 1 (least deprived) | Reference group | Reference group | ||||
| 2 | 1.25 | 0.82, 1.91 | 0.30 | 1.48 | 0.91, 2.43 | 0.12 |
| 3 | 0.95 | 0.56, 1.60 | 0.84 | 1.25 | 0.69, 2.27 | 0.46 |
| 4 | 0.98 | 0.58, 1.67 | 0.95 | 1.68 | 0.93, 3.06 | 0.09 |
| 5 (most deprived) | 0.74 | 0.37, 1.48 | 0.39 | 1.38 | 0.66, 2.92 | 0.39 |
| Random effect | ||||||
| School (SD) | 0.30 | 0.36 | ||||
| No. Obs. | 1,157 | 1,157 | ||||
| Sigma | 1.00 | 1.00 | ||||
| Log‐likelihood | −503 | −423 | ||||
| AIC | 1,033 | 874 | ||||
| BIC | 1,104 | 945 | ||||
| Deviance | 990 | 830 | ||||
| Residual df | 1,142 | 1,143 | ||||
| Mixture of goods and bads b | ||||||
| Ψ (psi) | 1.18 | 1.01, 1.37 | 0.04 | 0.95 | 0.80, 1.13 | 0.58 |
Note. Variables with p‐value < 0.05 in bold italics.
OR = Odds Ratio, CI = Confidence Interval.
Effect of mixture of goods and bads estimated using quantile g‐computation.
No statistically significant associations were apparent between access to health‐promoting and health‐constraining features of the environment and meeting screen time guidelines. As indicated in Table 2, age (OR = 0.71 [0.62; 0.82]) was identified as the most important factor with older adolescents having lower odds of meeting screen time guidelines compared with younger adolescents. The mixture of health‐promoting and health‐constraining environments was not identified as statistically significant. Even though not statistically significant, increased access to the mix of health‐constraining environments lowers the odds of meeting the screen time guideline (OR = 0.84 [0.69; 1.02]), while the opposite applied to access to health‐promoting environments (OR = 1.13 [0.93; 1.38]). Furthermore, the odds of meeting the guideline were decreased for Māori participants (OR = 0.56 [0.28; 1.08]).
When examining the individual domains of the HLI in Table 3, access to blue space (such as beaches, rivers, and lakes) was the only variable positively associated with the likelihood of meeting both physical activity guidelines (OR = 1.15 [1.00, 1.31]) and screen time guidelines (OR = 1.18 [1.02, 1.37]).
Table 3.
Results of Multilevel Mixed Effects Models (Adolescents Nested in Schools) by Quintiles of Environmental Domains
| Physical activity | Screen time | |||||
|---|---|---|---|---|---|---|
| OR a | 95% CI a | p‐value | OR a | 95% CI a | p‐value | |
| Health‐promoting domains (quintile) | ||||||
| Supermarkets | 1.03 | 0.85, 1.25 | 0.76 | 0.98 | 0.79, 1.21 | 0.85 |
| Fruit & vegetable stores | 1.21 | 0.93, 1.57 | 0.16 | 1.18 | 0.87, 1.60 | 0.28 |
| Physical activity facilities | 0.86 | 0.68, 1.09 | 0.22 | 0.98 | 0.75, 1.27 | 0.88 |
| Blue space | 1.15 | 1.00, 1.31 | 0.04 | 1.18 | 1.02, 1.37 | 0.02 |
| Greenspace | 1.09 | 0.96, 1.24 | 0.18 | 0.95 | 0.83, 1.09 | 0.47 |
| Health‐constraining domains (quintile) | ||||||
| Fast foods | 1.23 | 0.93, 1.62 | 0.14 | 1.18 | 0.87, 1.61 | 0.28 |
| Takeaways | 1.06 | 0.85, 1.33 | 0.59 | 0.79 | 0.61, 1.02 | 0.07 |
| Dairy and convenience stores | 0.91 | 0.75, 1.11 | 0.35 | 0.98 | 0.80, 1.22 | 0.89 |
| Age | 0.96 | 0.85, 1.07 | 0.43 | 0.71 | 0.61, 0.81 | <0.001 |
| Sex | ||||||
| Male | Reference group | Reference group | ||||
| Female | 0.44 | 0.30, 0.66 | <0.001 | 1.16 | 0.75, 1.80 | 0.51 |
| Ethnicity | ||||||
| NZ European | Reference group | Reference group | ||||
| Māori | 1.78 | 1.11, 2.84 | 0.02 | 0.55 | 0.28, 1.08 | 0.08 |
| Pasifika | 0.48 | 0.16, 1.43 | 0.19 | 0.83 | 0.32, 2.14 | 0.70 |
| Asian | 0.45 | 0.21, 0.99 | 0.04 | 1.04 | 0.50, 2.17 | 0.92 |
| Other | 0.64 | 0.28, 1.46 | 0.28 | 0.65 | 0.25, 1.71 | 0.39 |
| Deprivation (quintile) | ||||||
| 1 (least deprived) | Reference group | Reference group | ||||
| 2 | 1.38 | 0.89, 2.12 | 0.15 | 1.54 | 0.93, 2.54 | 0.09 |
| 3 | 1.07 | 0.63, 1.81 | 0.81 | 1.30 | 0.71, 2.37 | 0.39 |
| 4 | 1.01 | 0.59, 1.72 | 0.98 | 1.64 | 0.90, 2.99 | 0.10 |
| 5 (most deprived) | 0.72 | 0.35, 1.47 | 0.36 | 1.31 | 0.61, 2.83 | 0.49 |
| Random effect | ||||||
| School (SD) | 0.30 | 0.34 | ||||
| No. Obs. | 1,157 | 1,157 | ||||
| Sigma | 1.00 | 1.00 | ||||
| Log‐likelihood | −500 | −419 | ||||
| AIC | 1,039 | 878 | ||||
| BIC | 1,140 | 979 | ||||
| Deviance | 984 | 823 | ||||
| Residual df | 1,137 | 1,137 | ||||
Note. Variables with p‐value <0.05 in bold italics.
OR = Odds Ratio, CI = Confidence Interval.
4. Discussion
This study aimed to examine the association between access to the mixture of health‐promoting and health‐constraining environmental features and physical activity and screen time of adolescents residing in Dunedin (NZ). Access to the built and natural environment was defined using a range of health‐promoting and health‐constraining environmental features existing in the HLI (Marek et al., 2021). Our study revealed three key findings. First, an association existed between better access to health‐promoting features of the environment and a greater likelihood of meeting the recommended physical activity guidelines. Second, g‐computation modeling showed the importance of the mixture of health‐promoting and health‐constraining features of the environment, likely due to their co‐occurrence in neighborhoods and space especially in this sample. Third, no association was apparent between health‐promoting and health‐constraining environmental features, or their mixture, and adolescents' screen time.
With regard to our first finding, access to health‐promoting environments (e.g., greenspaces, physical activity facilities, blue spaces) supports meeting physical activity guidelines in adolescents in Dunedin. This is important as engaging in sufficient levels of physical activity is related to a plethora of mental and physical health benefits for adolescents (Bull et al., 2020). Furthermore, this finding is consistent with a growing body of evidence that suggests environmental factors influence adolescents' physical activity levels (Prince et al., 2022). For instance, positive associations have been found between physical activity and publicly provided recreational infrastructure and transport infrastructure (Davison & Lawson, 2006) as well as perceived access to parks and playgrounds (Carroll‐Scott et al., 2013). In addition, outdoor and freely available neighborhood facilities including beaches, trails and neighborhood streets are frequently used for physical activity (Lee & Moudon, 2004).
Our study also showed that the combination of health‐promoting and health‐constraining environments is important, despite the health‐constraining environments not being significant on their own. This is consistent with previous NZ‐based evidence showing that the co‐occurrence of both health‐constraining and health‐promoting features was related to movement behaviors in adolescents when measured by GPS in the urban areas of Auckland and Wellington (Hobbs et al., 2022). Other research has also noted that the combination of both health‐promoting and health‐constraining features is important to consider when investigating the impact of the environment on health and health behaviors. For instance, corner stores (e.g., dairies, milk bars) and fast‐food restaurants may serve as attractive locations for adolescents, which may foster accumulation of more physical activity (Hume et al., 2005). Similar behavior of adolescents who spent a considerable time around fast‐food outlets and dairies was also identified by GPS based study in NZ (Hobbs et al., 2022). Though these types of locations often offer destinations that facilitate social interactions for adolescents, they are predominantly considered health‐constraining due to their associations with obesity and risk for other non‐communicable diseases such as type 2 diabetes (Libuy et al., 2024). Thus, the relevance or role of the physical environment for the physical activity of youth may vary depending on life stage (Holt et al., 2008). There is certainly a need for more nuanced research focusing on the context of individual domains of the environment as well as their mixture taking into account more specific enablers of and barriers to physical activity.
No association was observed between environment and adolescents' screen time. This mirrors previous evidence where, for most environmental factors (e.g., living in a cul‐de‐sac, playground area at school), there is no evidence or inconsistent evidence for an association with sedentary behavior of youth (Stierlin et al., 2015). Similarly, ecological models suggest that it is the most proximal environments (i.e., within the home, school, or workplace) that will most likely impact the sedentary behavior of people (Hadgraft et al., 2023). Thus, the neighborhood environment or that experienced while commuting to school may be less influential in the screen time consumption of adolescents. Despite this, NZ research has previously demonstrated that poorer access to health‐promoting environments was related to more vehicle travel and good access to health‐promoting environments was related to less sedentary time in adolescents (Hobbs et al., 2022). This previous study used a combination of accelerometery and global positioning systems data to provide detailed measures of actual environmental exposures, albeit with a smaller sample (n = 191 adolescents), spread across seven schools over two cities (Auckland and Wellington). In contrast, our study used home addresses as a proxy of exposure to the environment, but we had a much larger sample including adolescents from all 12 secondary schools in Dunedin city, which may explain these differential findings. Furthermore, it is known that the availability and accessibility of resources do not necessarily correspond to their utilization, which may also be influenced by other factors such as the quality, acceptability, and affordability of the environmental features (Gocer et al., 2023; Volf et al., 2022). Interestingly, when investigating individual domains of the built environment, access to blue spaces (beaches, rivers, and lakes) was associated with meeting screen time guidelines. While this illustrates the strength of the methodological approach we used, which allows for simultaneous examination of effects of the mixture of environmental exposures and its individual components, additional research is needed to examine the environmental correlates and determinants of sedentary behavior and screen time in adolescents.
While considering the “gestalt” or mixture of health‐promoting and constraining dimensions of the environment may be necessary to fully understand physical activity behavior, considering individual domains (e.g., access to blue spaces), may be more relevant to understanding screen time. One possible explanation is that the latter is, arguably, a less complex behavior than the former in terms, for example, of its determinants and purpose. Therefore, we advocate for using a method that allows for simultaneous examination of effects of the mixture of environmental exposures and of its individual components as presented in our study.
Consistent with ecological models (e.g., Spence & Lee, 2002), our findings suggest an upstream approach and the provision of physical activity‐conducive environments may be effective strategies for providing equitable opportunities to physical activity for children and youth (Bangsbo et al., 2016). In terms of individual health‐promoting features of the environment, our study showed the importance of blue space for adolescents to accumulate health‐promoting levels of physical activity. This finding adds to the growing evidence indicating that proximity and access to coastal and inland water bodies are associated with higher levels of physical activity (Georgiou et al., 2021) while contributing specifically to the scant evidence about this phenomenon in adolescents. It is of relevance to note that Dunedin is a coastal city with many beaches scattered along the coastline and around the harbor, most being easily accessible and only a few minutes drive from the central city. The salience of this feature of the environment is further highlighted in the circumstance that access to blue space was also the only individual environmental domain in this study that was significantly associated, in the expected directions, with both physical activity and screen time in adolescents. From a health promotion perspective, however, it is important to note that previous research underscores that individuals with less education and/or lower income are more likely to face issues of blue space access or availability (Schüle et al., 2019). Therefore, if we are to take advantage of the potential of blue spaces for physical activity promotion, appropriate measures need to be taken to ensure adolescents have access to these spaces, regardless of their background.
It is likely the consideration of additional features specific to supporting physical activity (e.g., bike lanes (Pan et al., 2021) and public transport (Rissel et al., 2012)) would further explain adolescents' physical activity. A combination of environmental and programming interventions may also be necessary; among the recognized investments for physical activity, initiatives such as whole‐of‐school programs, active transport, active urban design, sport and recreation, and community‐wide programs would be most relevant to this population (Milton et al., 2021). Internationally, a visible shift has occurred in the way policymakers and stakeholders deal with the public health challenges presented (not only) by climate change (Allen et al., 2018), including the promotion of sustainable behavior (e.g., active transport) and modification of the built environment to encourage such behavior (Salvo et al., 2021).
Similarly, international evidence shows that the general public can be open to policy initiatives that may facilitate physical activity for all while challenging conventional norms around the use of personal automobiles for local travel and transport, however the existing socioeconomic and demographic differences affecting need to be considered (Fagan et al., 2023; McCurdy et al., 2023). In relation to this, upstream and environmental approaches to interventions can enable reaching wider populations while having more sustainable longer‐term effects (Lakerveld et al., 2020). This is also important when considering other fields like spatial planning and urban design which often tackle the liveability of the places but can also impact population‐level health and health behaviors such as physical activity (Crane et al., 2021). To create more accessible and inclusive cities incorporating and emphasizing health‐promoting features of the environment, planners can improve on physical activity of not only adolescents but perhaps other population groups as well within the wider system (Mandic et al., 2020).
Strengths of the study include a large representative sample of adolescents from all high schools in the study city and the use of quantile g‐computation to assess the synergistic contribution of environmental characteristics to health behavior. However, some limitations should be acknowledged. First, due to the cross‐sectional design, causality cannot be inferred. Second, though we included covariates representing individual (age, sex, ethnicity) and area‐level (deprivation) characteristics, and clustered students within their schools, we were not able to control for other individual‐ and socioeconomic or environmental variables that create a whole landscape affecting adolescents' behaviors.
Third, while the area‐level data and residential location data are spatial, we have used non‐spatial models due to the intention to explore the importance of the mixture of the environments using quantile g‐computation, usage of (spatially) sparse individual‐level data preventing clear definition (and conceptualization) of the neighborhood, and lastly, the spatial context in both model types used (quantile g‐computing and multilevel models) is to some extent captured indirectly by the school due to the zoning of schools in New Zealand. The fourth limitation is then related to the complete case analysis that may have potentially biased the results and changed the inference (Donders et al., 2006), however, the imputation of missing data was not possible due to the details of the data access agreement.
We used only a selection of possible explanatory environmental variables that are available within the HLI (Marek et al., 2021). Even though HLI is the most complex and detailed measure of health‐promoting and constraining features of the built environment in NZ, it poses its own limitations. For instance, given that this research is focused on physical activity, other domains including the availability of walking and cycling infrastructure in home neighborhoods and distance to various destinations may provide further insight into the features of the environment that contribute to adolescents' physical activity and should be an area for future research. HLI also does not consider physical activity‐specific health constraining features such as the presence of major highways and arterial roads, and it does not measure additional quality or other temporal factors that might impact physical activity (e.g., safety and weather). In addition, this study does not account for the actual mobility and daily patterns of the participants (Campbell et al., 2021).
The data from the BEATS Study cover a large sample of adolescents from all 12 high schools across Dunedin, which has a unique geography including the proximity to blue spaces for many residents regardless of their socioeconomic status. The results of this study may not be directly applicable in other regions with different cultural and environmental conditions. Further, the sociodemographic characteristics of Dunedin differ from other cities and towns in NZ with lower proportions residing in the most deprived areas and a smaller proportion of Pacific Peoples. Finally, the survey uses prioritized ethnicity which may be problematic due to the common presence of individuals identifying as multiple ethnic groups.
5. Conclusions
We provide evidence of a relationship between health‐promoting environments, the mix of health‐promoting and health‐constraining environments, and physical activity in adolescence but not screen time. The findings support the hypothesis that the environment has the potential to induce positive health behaviors in adolescents, particularly when it comes to adolescents' physical activity. Consequently, leverage points for improving physical activity and thus, health of adolescents, can be sought in upstream environmental‐based interventions providing equitable access to health‐promoting features of the environment as well as opportunities to access them.
Conflict of Interest
Sandra Mandic is the founder and the director of the research consultancy AGILE Research Ltd. (www.agileresearch.nz) and the Team Leader Transport Strategy at Wellington City Council (Wellington, New Zealand). Other authors have no conflict of interest.
Acknowledgments
The BEATS Research Programme (2013–2023) was a collaboration between the Dunedin Secondary Schools’ Partnership, Dunedin City Council, University of Otago and Auckland University of Technology. The authors would like to acknowledge BEATS investigators, Advisory Board members, collaborators, research personnel (research assistants, students, and volunteers), and all participating schools and adolescents. The BEATS Study was supported by the Health Research Council of New Zealand Emerging Researcher First Grant (14/565), National Heart Foundation of New Zealand (1602 and 1615), Lottery Health Research Grant (Applic 341129), University of Otago Research Grant (UORG 2014), Dunedin City Council and the University of Otago internal grants. Open access publishing facilitated by University of Canterbury, as part of the Wiley ‐ University of Canterbury agreement via the Council of Australian University Librarians.
Marek, L. , Wiki, J. , Mandic, S. , Spence, J. C. , Smith, M. , García Bengoechea, E. , et al. (2025). Access to healthy built and natural environments and physical activity and screen time in New Zealand adolescents: A geospatial cross‐sectional study. GeoHealth, 9, e2024GH001101. 10.1029/2024GH001101
Data Availability Statement
Individual‐level data supporting this research are not accessible to the public or research community due to the sensitivity of the collected data as well as the confidentiality agreement where participants have been assured that the collected data will not be shared. For any queries about BEATS data used in this analysis, please contact Adjunct Professor Sandra Mandic at sandy.mandic@aut.ac.nz. The environmental data (Healthy Location Index) are available at GeoHealth Lab repository via https://www.canterbury.ac.nz/content/dam/uoc‐main‐site/documents/zip‐files/geohealth‐laboratory/Environmental_goods_bads_MB2018.zip under Creative Commons (CC BY 3.0 NZ) license.
References
- Allen, C. , Metternicht, G. , & Wiedmann, T. (2018). Initial progress in implementing the Sustainable Development Goals (SDGs): A review of evidence from countries. Sustainability Science, 13(5), 1453–1467. 10.1007/s11625-018-0572-3 [DOI] [Google Scholar]
- Atkinson, J. , Salmond, C. , & Crampton, P. (2020). NZDep2018 index of deprivation, final research report, December 2020. University of Otago. Retrieved from http://www.wnmeds.ac.nz/NZDep‐info.html [Google Scholar]
- Aubert, S. , Barnes, J. , Demchenko, I. , Hawthorne, M. , Abdeta, C. , Abi Nader, P. , et al. (2022). Global matrix 4.0 physical activity report card grades for children and adolescents: Results and analyses from 57 countries. Journal of Physical Activity and Health, 19(11), 700–728. 10.1123/jpah.2022-0456 [DOI] [PubMed] [Google Scholar]
- Bangsbo, J. , Krustrup, P. , Duda, J. , Hillman, C. , Andersen, L. B. , Weiss, M. , et al. (2016). The Copenhagen Consensus Conference 2016: Children, youth, and physical activity in schools and during leisure time. British Journal of Sports Medicine, 50(19), 1177–1178. 10.1136/bjsports-2016-096325 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bull, F. C. , Al‐Ansari, S. S. , Biddle, S. , Borodulin, K. , Buman, M. P. , Cardon, G. , et al. (2020). World Health Organization 2020 guidelines on physical activity and sedentary behaviour. British Journal of Sports Medicine, 54(24), 1451–1462. 10.1136/bjsports-2020-102955 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell, M. , Marek, L. , & Hobbs, M. (2021). Reconsidering movement and exposure: Towards a more dynamic health geography. Geography Compass, 15(6). Article e12566. 10.1111/gec3.12566 [DOI] [Google Scholar]
- Carroll‐Scott, A. , Gilstad‐Hayden, K. , Rosenthal, L. , Peters, S. M. , McCaslin, C. , Joyce, R. , & Ickovics, J. R. (2013). Disentangling neighborhood contextual associations with child body mass index, diet, and physical activity: The role of built, socioeconomic, and social environments. Social Science & Medicine, 95, 106–114. 10.1016/j.socscimed.2013.04.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crane, M. , Lloyd, S. , Haines, A. , Ding, D. , Hutchinson, E. , Belesova, K. , et al. (2021). Transforming cities for sustainability: A health perspective. Environment International, 147, 106366. 10.1016/j.envint.2020.106366 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Currie, C. , Nic Gabhainn, S. , Godeau, E. , & the International HBSC Network Coordinating Committee. (2009). The Health Behaviour in School‐aged Children: WHO Collaborative Cross‐National (HBSC) study: Origins, concept, history and development 1982‐2008. International Journal of Public Health, 54(Suppl 2), 131–139. 10.1007/s00038-009-5404-x [DOI] [PubMed] [Google Scholar]
- Davison, K. K. , & Lawson, C. T. (2006). Do attributes in the physical environment influence children's physical activity? A review of the literature. International Journal of Behavioral Nutrition and Physical Activity, 3(1), 19. Article 19. 10.1186/1479-5868-3-19 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donders, A. R. T. , Van Der Heijden, G. J. , Stijnen, T. , & Moons, K. G. (2006). A gentle introduction to imputation of missing values. Journal of Clinical Epidemiology, 59(10), 1087–1091. 10.1016/j.jclinepi.2006.01.014 [DOI] [PubMed] [Google Scholar]
- Fagan, M. J. , Vanderloo, L. M. , Banerjee, A. , Ferguson, L. J. , Lee, E. Y. , O’Reilly, N. , et al. (2023). Assessing support for policy actions with co‐benefits for climate change and physical activity in Canada. Journal of Physical Activity and Health, 21(3), 256–265. 10.1123/jpah.2023-0617 [DOI] [PubMed] [Google Scholar]
- Gebremariam, M. K. , Henjum, S. , Terragni, L. , & Torheim, L. E. (2020). Correlates of screen time and mediators of differences by parental education among adolescents. BMC Pediatrics, 20(1), 279. Article 279. 10.1186/s12887-020-02181-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Georgiou, M. , Morison, G. , Smith, N. , Tieges, Z. , & Chastin, S. (2021). Mechanisms of impact of blue spaces on human health: A systematic literature review and meta‐analysis. International Journal of Environmental Research and Public Health, 18(5), 2486. 10.3390/ijerph18052486 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gocer, O. , Wei, Y. , Torun, A. O. , Alvanides, S. , & Candido, C. (2023). Multidimensional attributes of neighbourhood quality: A systematic review. Heliyon, 9(11), e22636. 10.1016/j.heliyon.2023.e22636 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guthold, R. , Stevens, G. A. , Riley, L. M. , & Bull, F. C. (2020). Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population‐based surveys with 1·6 million participants. The Lancet Child & Adolescent Health, 4(1), 23–35. 10.1016/S2352-4642(19)30323-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hadgraft, N. , Dunstan, D. , & Owen, N. (2023). An ecological model for understanding and influencing sedentary behaviour. In Leitzmann M. F., Jochem C., & Schmid D. (Eds.), Sedentary behaviour epidemiology. Springer series on epidemiology and public health. Springer. 10.1007/978-3-031-41881-5_15 [DOI] [Google Scholar]
- Hobbs, M. , Stewart, T. , Marek, L. , Duncan, S. , Campbell, M. , & Kingham, S. (2022). Health‐promoting and health‐constraining environmental features and physical activity and sedentary behaviour in adolescence: A geospatial cross‐sectional study. Health & Place, 77, 102887. Article 102887. 10.1016/j.healthplace.2022.102887 [DOI] [PubMed] [Google Scholar]
- Holt, N. L. , Spence, J. C. , Sehn, Z. L. , & Cutumisu, N. (2008). Neighborhood and developmental differences in children's perceptions of opportunities to play and be physically active. Health & Place, 14(1), 2–14. 10.1016/j.healthplace.2007.03.002 [DOI] [PubMed] [Google Scholar]
- Hume, C. , Salmon, J. , & Ball, K. (2005). Children's perceptions of their home and neighborhood environments, and their association with objectively measured physical activity: A qualitative and quantitative study. Health Education Research, 20(1), 1–13. 10.1093/her/cyg095 [DOI] [PubMed] [Google Scholar]
- Keil, A. (2023). qgcomp: Quantile G‐computation. R Package Version 2.15.2. https://CRAN.R‐project.org/package=qgcomp [Google Scholar]
- Keil, A. P. , Buckley, J. P. , O’Brien, K. M. , Ferguson, K. K. , Zhao, S. , & White, A. J. (2020). A quantile‐based g‐computation approach to addressing the effects of exposure mixtures. Environmental Health Perspectives, 128(4). Article 047004. 10.1289/EHP5838 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lakerveld, J. , Woods, C. , Hebestreit, A. , Brenner, H. , Flechtner‐Mors, M. , Harrington, J. M. , et al. (2020). Advancing the evidence base for public policies impacting on dietary behaviour, physical activity and sedentary behaviour in Europe: The policy evaluation network promoting a multidisciplinary approach. Food Policy, 96, 101873. 10.1016/j.foodpol.2020.101873 [DOI] [Google Scholar]
- Lee, C. , & Moudon, A. V. (2004). Physical activity and environment research in the health field: Implications for urban and transportation planning practice and research. Journal of Planning Literature, 19(2), 147–181. 10.1177/0885412204267680 [DOI] [Google Scholar]
- Letellier, N. , Zamora, S. , Yang, J. A. , Sears, D. D. , Jankowska, M. M. , & Benmarhnia, T. (2022). How do environmental characteristics jointly contribute to cardiometabolic health? A quantile g‐computation mixture analysis. Preventive Medicine Reports, 30, 102005. 10.1016/j.pmedr.2022.102005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Libuy, N. , Church, D. , Ploubidis, G. , & Fitzsimons, E. (2024). Fast food proximity and weight gain in childhood and adolescence: Evidence from Great Britain. Health Economics, 33(3), 449–465. 10.1002/hec.4770 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mandic, S. , Bengoechea, E. G. , Coppell, K. J. , & Spence, J. C. (2017). Clustering of (un) healthy behaviors in adolescents from Dunedin, New Zealand. American Journal of Health Behavior, 41(3), 266–275. 10.5993/AJHB.41.3.6 [DOI] [PubMed] [Google Scholar]
- Mandic, S. , Jackson, A. , Lieswyn, J. , Mindell, J. S. , García Bengoechea, E. , Spence, J. C. , et al. (2020). Development of key policy recommendations for active transport in New Zealand: Multi‐sector and multidisciplinary endeavour. Journal of Transport & Health, 18, 100859. Article 100859. 10.1016/j.jth.2020.100859 [DOI] [Google Scholar]
- Mandic, S. , Khan, A. , Bengoechea, E. G. , Coppell, K. J. , Spence, J. C. , & Smith, M. (2024). Physical activity, screen time and dietary behaviours in New Zealand adolescents prior to and following the onset of the COVID‐19 pandemic. BMC Public Health, 24(1), 188. Article 188. 10.1186/s12889-024-17688-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mandic, S. , Mountfort, A. , Hopkins, D. , Flaherty, C. , Williams, J. , Brook, E. , et al. (2015). Built Environment and Active Transport to School (BEATS) study: Multidisciplinary and multi‐sector collaboration for physical activity promotion. RETOS, 28, 197–202. 10.47197/retos.v0i28.34955 [DOI] [Google Scholar]
- Mandic, S. , Williams, J. , Moore, A. , Hopkins, D. , Flaherty, C. , Wilson, G. , et al. (2016). Built Environment and Active Transport to School (BEATS) study: Protocol for a cross‐sectional study. BMJ Open, 6(5), e011196. Article e011196. 10.1136/bmjopen-2016-011196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marek, L. , Hobbs, M. , Wiki, J. , Kingham, S. , & Campbell, M. (2021). The good, the bad, and the environment: Developing an area‐based measure of access to health‐promoting and health‐constraining environments in New Zealand. International Journal of Health Geographics, 20(1), 16. Article 16. 10.1186/s12942-021-00269-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCurdy, A. , Faulkner, G. , Cameron, C. , Costas‐Bradstreet, C. , & Spence, J. C. (2023). Support for active transport policy initiatives among Canadian adults: The Canadian national active transportation survey. Active Travel Studies, 3(2). 10.16997/ats.1450 [DOI] [Google Scholar]
- Milton, K. , Cavill, N. , Chalkley, A. , Foster, C. , Gomersall, S. , Hagstromer, M. , et al. (2021). Eight Investments that work for physical activity. Journal of Physical Activity and Health, 18(6), 625–630. 10.1123/jpah.2021-0112 [DOI] [PubMed] [Google Scholar]
- Ministry of Health . (2004). A portrait of health: Key results of the 2002/03 New Zealand health survey. Ministry of Health. Retrieved from https://www.health.govt.nz/nz‐health‐statistics/surveys/new‐zealand‐health‐survey#02‐03 [Google Scholar]
- Pan, X. , Zhao, L. , Luo, J. , Li, Y. , Zhang, L. , Wu, T. , et al. (2021). Access to bike lanes and childhood obesity: A systematic review and meta‐analysis. Obesity Reviews, 22(S1), e13042. 10.1111/obr.13042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prince, S. A. , Lancione, S. , Lang, J. J. , Amankwah, N. , de Groh, M. , Jaramillo Garcia, A. , et al. (2022). Examining the state, quality and strength of the evidence in the research on built environments and physical activity among children and youth: An overview of reviews from high income countries. Health & Place, 76, 102828. Article 102828. 10.1016/j.healthplace.2022.102828 [DOI] [PubMed] [Google Scholar]
- Rissel, C. , Curac, N. , Greenaway, M. , & Bauman, A. (2012). Physical activity associated with public transport use‐‐a review and modelling of potential benefits. International Journal of Environmental Research and Public Health, 9(7), 2454–2478. 10.3390/ijerph9072454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robins, J. (1986). A new approach to causal inference in mortality studies with a sustained exposure period—Application to control of the healthy worker survivor effect. Mathematical Modelling, 7(9–12), 1393–1512. 10.1016/0270-0255(86)90088-6 [DOI] [Google Scholar]
- Salvo, D. , Garcia, L. , Reis, R. S. , Stankov, I. , Goel, R. , Schipperijn, J. , et al. (2021). Physical activity promotion and the United Nations sustainable development goals: Building synergies to maximize impact. Journal of Physical Activity and Health, 18(10), 1163–1180. 10.1123/jpah.2021-0413 [DOI] [PubMed] [Google Scholar]
- Schüle, S. A. , Hilz, L. K. , Dreger, S. , & Bolte, G. (2019). Social inequalities in environmental resources of green and blue spaces: A review of evidence in the WHO European region. International Journal of Environmental Research and Public Health, 16(7), 1216. 10.3390/ijerph16071216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith, M. , Cui, J. , Ikeda, E. , Mavoa, S. , Hasanzadeh, K. , Zhao, J. , et al. (2021). Objective measurement of children's physical activity geographies: A systematic search and scoping review. Health & Place, 67, 102489. Article 102489. 10.1016/j.healthplace.2020.102489 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spence, J. C. , & Lee, R. E. (2002). Toward a comprehensive model of physical activity. Psychology of Sport and Exercise, 4(1), 7–24. 10.1016/S1469-0292(02)00014-6 [DOI] [Google Scholar]
- Statistics New Zealand . (2019). Statistical standard for geographic areas 2018: New standard released Wellington: Statistics New Zealand. Retrieved from http://archive.stats.govt.nz/methods/classifications‐and‐standards/current‐classifications‐and‐standards‐review/review‐geographic.aspx
- Sterdt, E. , Liersch, S. , & Walter, U. (2014). Correlates of physical activity of children and adolescents: A systematic review of reviews. Health Education Journal, 73(1), 72–89. 10.1177/0017896912469578 [DOI] [Google Scholar]
- Stierlin, A. S. , De Lepeleere, S. , Cardon, G. , Dargent‐Molina, P. , Hoffmann, B. , Murphy, M. H. , et al. (2015). A systematic review of determinants of sedentary behaviour in youth: A DEDIPAC‐study. International Journal of Behavioral Nutrition and Physical Activity, 12(1), 133. Article 133. 10.1186/s12966-015-0291-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stiglic, N. , & Viner, R. M. (2019). Effects of screentime on the health and well‐being of children and adolescents: A systematic review of reviews. BMJ Open, 9(1), e023191. Article e023191. 10.1136/bmjopen-2018-023191 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Volf, K. , Kelly, L. , Bengoechea, E. G. , Casey, B. , Gelius, P. , Messing, S. , et al. (2022). Evidence of the impact of sport policies on physical activity and sport participation: A systematic mixed studies review. International Journal of Sport Policy and Politics, 14(4), 697–712. 10.1080/19406940.2022.2127835 [DOI] [Google Scholar]
- Wilson, O. W. A. , Ikeda, E. , Hinckson, E. , Mandic, S. , Richards, J. , Duncan, S. , et al. (2023). Results from Aotearoa New Zealand's 2022 report card on physical activity for children and youth: A call to address inequities in health‐promoting activities. Journal of Exercise Science and Fitness, 21(1), 58–66. 10.1016/j.jesf.2022.10.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Individual‐level data supporting this research are not accessible to the public or research community due to the sensitivity of the collected data as well as the confidentiality agreement where participants have been assured that the collected data will not be shared. For any queries about BEATS data used in this analysis, please contact Adjunct Professor Sandra Mandic at sandy.mandic@aut.ac.nz. The environmental data (Healthy Location Index) are available at GeoHealth Lab repository via https://www.canterbury.ac.nz/content/dam/uoc‐main‐site/documents/zip‐files/geohealth‐laboratory/Environmental_goods_bads_MB2018.zip under Creative Commons (CC BY 3.0 NZ) license.