

Abstract
Chronic diseases have emerged as a paramount global health burden, accounting for 74% of global mortality and causing substantial economic losses. The oral cavity serves as a critical indicator of overall health and is inextricably linked to chronic disorders. Neglecting oral health can exacerbate localized pathologies and accelerate the progression of chronic conditions, whereas effective management has the potential to reduce their incidence and mortality. Nevertheless, limited resources and lack of awareness often impede timely dental intervention, delaying optimal therapeutic measures. This review provides a comprehensive analysis of the impact of prevalent chronic diseases—such as diabetes mellitus, rheumatoid arthritis, cardiovascular disorders, and chronic respiratory diseases—on oral health, along with an exploration of how changes in oral health affect these chronic conditions through both deterioration and intervention mechanisms. Additionally, novel insights into the underlying pathophysiological mechanisms governing these relationships are presented. By synthesizing these advancements, this review aims to illuminate the complex interrelationship between oral health and chronic diseases while emphasizing the urgent need for greater collaboration between dental practitioners and general healthcare providers to improve overall health outcomes.
Keywords: cardiovascular diseases, chronic diseases, chronic respiratory diseases, diabetes, oral health, rheumatoid arthritis
Mechanisms linking oral health to chronic diseases. The figure highlights oral health connections to diabetes, cardiovascular diseases, rheumatoid arthritis, and respiratory diseases. Key mechanisms include inflammation, microbial dysbiosis, oxidative stress, and immune dysregulation, emphasizing the systemic impacts of oral diseases like periodontitis.

1. INTRODUCTION
Noncommunicable diseases (NCDs), including cardiovascular diseases (CVDs), diabetes mellitus (DM), chronic respiratory diseases, cancers, and obesity, are characterized by their prolonged nature and often incurability. According to the World Health Organization (WHO), NCDs account for 74% of global mortality, with approximately 17 million individuals succumbing before the age of 70 each year. 1 These diseases impose a substantial economic burden, with healthcare expenditures surpassing 85% of total global healthcare costs. 2 In the US healthcare system alone, over one trillion dollars are allocated annually to the management of chronic diseases. 3 By 2030, the economic burden of major NCDs is projected to result in a loss of output amounting to $47 trillion, equivalent to 75% of the global gross domestic product (GDP) in 2010. 4 Moreover, aging populations and declining birth rates are anticipated to further exacerbate this burden.
The oral cavity, situated at the intersection of medicine and dentistry, serves as a critical indicator of overall health, with its pathological conditions frequently exerting a more profound impact on systemic health than is commonly acknowledged by many healthcare providers. 5 Ignoring oral health can not only exacerbate localized issues but also have significant repercussions on chronic diseases. 6 , 7 , 8 , 9 Proactively managing oral health through regular dental examinations and the maintenance of proper oral hygiene can significantly enhance quality of life while aiding in the prevention and management of chronic diseases, thereby reducing their incidence and mortality rates. 10 , 11 , 12 , 13 Regrettably, due to limited access to medical resources and dental care, 14 many patients only recognize the close association between oral and systemic health after experiencing more severe health events, which subsequently delays optimal treatment and prevention. It is imperative to further explore this domain to enhance awareness of the critical role that oral health plays in the development of chronic diseases and to underscore its significance in the prevention and management of systemic conditions.
This review seeks to elucidate the relationships between oral health and prevalent chronic diseases (Figure 1), including DM, rheumatoid arthritis (RA), CVDs, and chronic respiratory diseases. It highlights recent advancements in understanding the mechanisms that connect oral health to these ailments and discusses strategies for enhancing oral care while managing chronic diseases.
FIGURE 1.

Oral conditions and chronic diseases. The left portion of the chart presents the common oral conditions referred to in this article, while the right portion exhibits the chronic diseases closely associated with oral conditions. Created with BioRender.com.
2. DIABETES MELLITUS AND ORAL HEALTH
DM encompasses a spectrum of metabolic disorders characterized by insufficient insulin secretion, insulin resistance, or a combination of both, leading to impaired regulation of blood glucose levels. It exhibits a complex and interdependent relationship with oral health. Hyperglycemia increases the risk of oral diseases, including periodontal diseases, apical periodontitis (AP), head and neck cancer (HNC), salivary gland diseases, dental caries, and root fracture, while also impeding the healing process of extraction sites. Glycemic control is intricately associated with the success rates of dental implants and root canal treatment (RCT) in patients with diabetes. Moreover, declining oral health conditions, such as periodontal disease, can increase the prevalence of diabetes and negatively impact glycemic control. Furthermore, diabetic patients frequently experience salivary gland dysfunction and chronic inflammation, resulting in complications such as xerostomia, infections, and oral mucosal lesions.
Consequently, the maintenance of oral health should be considered a vital component of comprehensive diabetes management to mitigate the incidence of related complications and enhance patients' quality of life. To facilitate readers' access to pertinent literature, we have summarized recent reviews, systematic evaluations, and meta‐analyses regarding the relationship between diabetes and various oral diseases in the table (Table 1).
TABLE 1.
Recent reviews/systematic reviews/meta‐analyses on diabetes and oral diseases.
| Topic | Author, year | Study type | Main contents |
|---|---|---|---|
| Overall oral health | Alqadi, 2024 15 | R | The oral manifestations of DM are delineated, along with essential dental considerations for the management of diabetic patients during treatment. |
| Grisi, 2022 16 | R | The authors examine prevalent oral signs and symptoms of diabetes, highlighting the mechanisms that connect DM to oral diseases and the associated risks of inadequate oral health in patients with DM. | |
| Ahmad, 2021 17 | R | The relationship between DM and oral complications is reviewed. | |
| Borgnakke, 2021 18 | R | The relationship between oral diseases and DM, including the underlying mechanisms, is summarized. Additionally, prevalent risk factors are delineated. | |
| Negrini, 2021 19 | R | The principal oral manifestations of DM are summarized. The interactions among diabetes, its risk factors, the oral microbiome, and oral diseases are analyzed. | |
| Periodontitis | Enteghad, 2024 20 | R | Epidemiological and clinical evidence regarding the association between DM and periodontitis is summarized. The predictive value of periodontal parameters for identifying diabetes is emphasized, and the biological mechanisms through which diabetes induces periodontal disease are reviewed. |
| Mirnic, 2024 21 | R | The clinical and epidemiological studies examining the bidirectional relationship between DM and periodontal disease, along with the pathogenesis and the role of oxidative stress, have been succinctly summarized. | |
| Vlachou, 2024 22 | R | The bidirectional relationship between DM and periodontitis is investigated, with a focus on the cellular and molecular mechanisms underlying the interaction between the oral microbiome and the host immune response. | |
| Păunică, 2023 23 | R | The most recent findings regarding the etiological factors, treatment, and prevention of both diseases are presented, with an emphasis on the role of diabetic microvascular complications, the oral microbiome, and inflammatory mediators. | |
| Zhao, 2023 24 | R | The potential mechanisms underlying the interaction between periodontitis and diabetes are summarized into six points: (1) microbiome factors; (2) enhanced inflammatory responses through cytokines, adipokines, AGE/RAGE, and miRNAs; (3) host immune factors; (4) oxidative stress; (5) alveolar bone resorption damage; and (6) epigenetic changes. | |
| Nibali, 2022 25 | R | The comorbidities associated with DM and periodontitis are summarized, and the underlying mechanisms are examined. | |
| Salhi, 2022 26 | R | The data concerning the impact of periodontitis on diabetes and vice versa are summarized in a descriptive table. | |
| Genco, 2020 27 | R | The role of diabetes as a risk factor for periodontal and other oral diseases is reviewed. | |
| Genco, 2020 28 | R | Studies elucidating the adverse effects of periodontal disease and diabetes are discussed, with a summary of their implications for clinical practice and public health. | |
| Graves, 2020 29 | R | The impact of DM on periodontal tissues, including periodontal ligament cells, osteoblasts, and osteocytes, is summarized. Furthermore, the effects of diabetes on the oral microbiome and its role in exacerbating periodontal bone loss are discussed. | |
| Polak, 2020 30 | R | The progression from DM to periodontitis is delineated, with a focus on microbiome alterations and immune changes in poorly controlled diabetes. Both microbiological and immunological shifts contributing to this condition are summarized. | |
| Costa, 2023 31 | S | The prevalence and severity of periodontal disease are higher in individuals with T1DM compared to the healthy population. | |
| Maia, 2023 32 | S | Fewer than half of diabetic patients are aware of their elevated risk for periodontal disease, and dentists frequently do not serve as the primary source encouraging them to seek this information. | |
| Nguyen, 2020 33 | S | Patients with periodontal disease are at an increased risk of developing diabetes‐related complications. | |
| Stöhr, 2021 34 | SM | There exists a positive bidirectional association between periodontitis and DM, underscoring the necessity of screening diabetic patients for periodontitis and vice versa. | |
| Baeza, 2019 35 | SM | SRP significantly affects metabolic control and reduction of systemic inflammation in patients with T2DM. | |
| Dental implants | Zhang, 2023 36 | R | The structure of peri‐implant soft tissue sealing, associated diseases and their treatments, as well as the regulatory mechanisms of T2DM in relation to soft tissue sealing damage, are comprehensively reviewed. |
| Vijay, 2021 37 | R | Recent advancements in the application of carbon‐based nanomaterials for enhancing dental implants in diabetic patients are summarized. | |
| Bencze, 2024 38 | SM | Within the constraints of this study, patients with poorly controlled T2DM or prediabetes may exhibit worse peri‐implant conditions compared to individuals without diabetes and those with well‐controlled T2DM. Furthermore, well‐controlled T2DM does not serve as a risk indicator for peri‐implant diseases. | |
| Al Ansari, 2022 39 | SM | Implants in diabetic patients exhibit a higher risk of failure and increased marginal bone resorption compared to nondiabetic individuals, with T1DM demonstrating a greater failure rate than T2DM. | |
| Andrade, 2022 40 | SM | With adequate blood glucose control, optimal oral hygiene, and strict adherence to procedural protocols, T2DM does not present a risk for immediate loading of implants. | |
| Lv, 2022 41 | SM | Diabetes or hyperglycemia upregulates negative regulators of bone metabolism, harming peri‐implant health. HbA1c levels are dose related to advanced glycation end products, periodontal disease, and marginal bone loss. | |
| Shang, 2021 42 | SM | BOP and PIBL were significantly higher in T2DM patients. However, strict oral hygiene reduced the impact of blood sugar levels on these parameters. | |
| AP | Tibúrcio‐Machado, 2017 43 | R | Current literature suggests a positive correlation between diabetes and an increased prevalence of periapical lesions. |
| Pérez‐Losada, 2020 44 | SM | There may be common pathophysiological factors underlying both AP and DM; however, the relationship between these two conditions necessitates further prospective studies. | |
| Liu, 2023 45 | SM | DM may elevate the risk of AP in teeth that have undergone endodontic treatment. Furthermore, in cases where apical periodontitis is already established, DM may exacerbate the progression of this condition. | |
| Head and neck cancer | Wang, 2020 46 | R | Recent advancements in the research concerning the relationship between DM and the mechanisms underlying head and neck cancer development have been summarized. |
| Ramos‐Garcia, 2021 47 | SM | The prevalence and risk of oral cancer, as well as potentially malignant oral diseases, are elevated in individuals with DM, and their associated mortality rate from oral cancer is significantly higher than that of nondiabetic individuals. | |
| Yan, 2021 48 | SM | T2DM is associated with an increased risk of head and neck cancers in East Asia. | |
| Salivary | Pérez‐Ros, 2021 49 | R | Salivary amylase and glucose concentrations represent potential noninvasive biomarkers for evaluating blood glucose control and clinical management in patients with DM. |
| Dental caries | Zhou, 2024 50 | SM | T2DM may lead to an increased dental caries index in adults, along with reduced salivary flow rate, pH, and buffering capacity. |
| Weijdijk, 2023 51 | SM | Compared to nondiabetic patients, diabetic patients have a higher DMF index score with moderate certainty. | |
| Coelho, 2020 52 | SM | T1DM patients have a higher risk of dental caries. | |
| de Lima, 2020 53 | SM | DM may increase the incidence of coronal and root caries in adults. Poor glycemic control makes diabetic patients more susceptible to dental caries. |
Abbreviations: AGE, advanced glycation end product; AP, apical periodontitis; BOP, bleeding on probing; DM, diabetes mellitus; PIBL, peri‐implant bone loss; R, review; RAGE, receptor for advanced glycation end product; S, systematic review; SM, systematic and meta‐analysis; SRP, scaling and root planning; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
2.1. Diabetes and periodontal diseases
Robust epidemiological and clinical evidence substantiates the association between the two. 20 , 21 , 22 Diabetic patients exhibit a significantly higher prevalence of periodontitis and show worse periodontal parameters, including clinical attachment loss, periodontitis surface area, and the number of teeth lost. 20 , 54 , 55 , 56 , 57 , 58 Conversely, individuals with periodontitis are at an increased risk of developing diabetes. 6
A recent study delineated the pathophysiological mechanisms through which diabetes impacts periodontal disease, encompassing vascular alterations in the gingiva, immune responses, collagen metabolism disorders, and specific microbiological profiles within periodontal pockets. Similarly, the mechanisms by which periodontal disease may affect diabetes include increased serum oxidative stress markers, elevated inflammatory markers, and enhanced insulin resistance. 21 In 2023, Zhao et al. identified six potential mechanisms underlying the interaction between periodontitis and diabetes (Figure 2): (1) microbial factors; (2) enhanced inflammatory response through cytokines, adipokines, advanced glycation end product/receptor for advanced glycation end product (AGE/RAGE) pathways, and miRNAs; (3) host immune factors; (4) oxidative stress; (5) alveolar bone resorption damage; and (6) epigenetic changes. 24 Later, Enteghad et al. added that the uncoupling of resorptive and formative responses in connective tissue. 20 To provide a novel perspective on the interaction between diabetes and periodontitis, we reviewed the literature pertaining to the underlying mechanisms (Table 2) utilizing key molecules that may play significant roles in both diseases as indicators.
FIGURE 2.
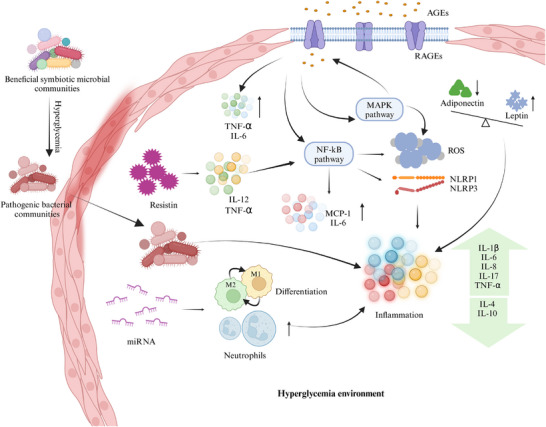
Mechanisms linking oral health and diabetes. Diabetes induces oral inflammation through multiple pathways, transforming beneficial microbial communities into pathogenic ones. Additionally, AGEs and resistin elevate inflammatory cytokines, thereby activating classical inflammatory pathways and generating ROS and inflammasomes. Dysregulation of adiponectin, leptin, and miRNA expression further drives immune cell differentiation and recruitment, exacerbating inflammation. AGEs, advanced glycation end products; IL‐4, interleukin‐4; IL‐6, interleukin‐6; IL‐8, interleukin‐8; IL‐10, interleukin‐10; IL‐17, interleukin‐17; MCP‐1, monocyte chemoattractant protein‐1; MMP, matrix metalloproteinase; M1, M1 macrophage; M2, M2 macrophage; NLRP1, NLR family pyrin domain containing 1; NLRP3, NLR family pyrin domain containing 3; RAGEs, receptor for advanced glycation end products; ROS, reactive oxygen species; TNF‐α, tumor necrosis factor‐alpha. Created with BioRender.com.
TABLE 2.
Key molecules in the interaction between diabetes and periodontitis.
| Core factors | Main findings | Clinical study | In vivo | In vitro |
|---|---|---|---|---|
| IL‐1 beta | Inflammatory cytokines play a role in the interplay between diabetes and periodontitis | 62 | ||
| IL‐6 | 63 | 64 | ||
| IL‐10 | 65 | |||
| IL‐12 | 66 | |||
| IL‐17 | 67 , 68 | |||
| IL‐21 | 69 | |||
| TNF‐E | 65 , 70 , 71 | 72 , 73 , 74 , 75 | 76 | |
| Adiponectin | Adiponectin has anti‐inflammatory effects and is linked to diabetes and glycemic control. After periodontal therapy, increased adiponectin can improve insulin resistance and lower HbA1c. The adiponectin receptor agonist, AdipoAI, may reduce tissue inflammation and damage, suggesting potential for treating diabetes‐related periodontitis. | 77 | 78 | |
| Visfatin | Periodontal inflammation can upregulate proinflammatory cytokines such as IL‐6 and IL‐1b, leading to elevated visfatin expression in periodontal tissues. Visfatin may play a role in the pathogenesis of periodontitis by promoting the upregulation of matrix metalloproteinase‐1 and chemokine CC‐motif ligand 2 in periodontal ligament cells. | 79 | ||
| ROS | ROS production induces MAPK and NLRP3‐related protein expression in high glucose conditions. ROS act as upstream signals for MAPKs, NF‐kappa B, and the NLRP3 inflammasome, leading to their activation. This process, along with increased oxidative damage and downregulation of Nrf2, contributes to the onset and progression of diabetic periodontitis. | 58 | 62 , 76 , 80 | |
| MAPK | 80 | |||
| NLRP3 | 80 | |||
| NF‐κB | 81 | 80 , 81 | ||
| Nrf2 | 82 | |||
| MMP | Elevated levels of MMP‐8 and MMP‐9 are associated with more severe periodontitis and an increased risk of diabetes mellitus. | 56 , 83 | ||
| CRP | CRP affects periodontitis and diabetes by inhibiting osteoblast formation and promoting osteoclast formation through the PI3K/AKT signaling pathway, disrupting alveolar bone homeostasis. | 84 | 85 | |
| hBDs | The concentrations of hBD‐2 and hBD‐3 are closely related to periodontal health and diabetic status. | 86 , 87 | ||
| GLUT1 | GLUT1, a key glucose transporter in macrophages, is upregulated in the gingiva of diabetic mice. It contributes to high glucose‐induced macrophage senescence and the SASP response, potentially worsening diabetic periodontitis. | 88 | ||
| AGEs | In chronic hyperglycemic conditions, AGEs significantly increase and affect periodontal tissue cell function by binding to RAGE, correlating with the severity of periodontitis. Additionally, AGEs negatively impact the skeletal system by inhibiting the expression of osteoblast‐related molecules, exacerbating periodontal disease in diabetic patients. | 70 , 89 | 73 | 76 , 90 , 91 , 92 , 93 |
| WBC | WBCs worsen the development and progression of periodontitis in diabetic patients by amplifying inflammatory responses and impairing immune function. | 84 , 94 | ||
| PMNs | The systemic effects of periodontal tissue inflammation may intensify the innate immune response of neutrophils, promoting the interaction between diabetes and periodontitis. | 95 | ||
| RANKL | Oral infections and diabetes can upregulate osteoclast RANKL expression, increasing the number and activity of osteoclasts, which leads to bone loss. In diabetic patients, RANK and RANKL expression are elevated, while OPG expression is reduced. | 96 | ||
| Microbial change | Diabetes can alter the diversity and composition of the oral microbiome, particularly the subgingival microbiota. | 97 , 98 , 99 | ||
| Gut microorganism | In PD patients, alterations in gut microbiota composition, particularly the reduction of butyrate‐producing bacteria, are associated with elevated blood glucose levels and impaired glucose tolerance. Using antibiotics or fecal microbiota transplantation to eliminate gut bacteria can improve blood glucose levels and inflammation markers. | 100 | ||
| miRNA | miR‐146a and miR‐155 may be novel biomarkers for periodontitis in both diabetic and nondiabetic patients. Additionally, miR‐126, by targeting TRAF6 and reducing inflammation in gingival fibroblasts under high glucose conditions, could serve as a potential therapeutic target for treating periodontitis in diabetic patients. | 101 | 102 , 103 | 103 , 104 , 105 , 106 |
| SNPs | SNPs influence disease susceptibility and severity. SNPs in the IL‐1, IL‐4, and IL‐6 genes are significantly associated with the risk of diabetes and periodontitis. | 107 | ||
| 25VD3 | Patients with diabetes and periodontitis have lower levels of vitamin D and calcium, which are negatively correlated with RBS and HbA1c levels. | 108 |
Abbreviations: AGEs, advanced glycation end products; CRP, C‐reactive protein; GLUT1, the glucose transporter 1; hBDs, human beta‐defensins; IL, interleukin; MAPK, mitogen‐activated protein kinase; MMP, metalloproteinase; NF‐κB, nuclear factor kappa‐B; NLRP3, NOD‐like receptor pyrin domain containing three; Nrf2, nuclear factor erythroid 2‐related factor 2; OPG, osteoprotegerin; PD, periodontal diseases; PMNs, polymorphonuclear neutrophils; RAGEs, receptor for advanced glycation end products; RANK, receptor activator of nuclear factor‐κ B; RANKL, receptor activator of nuclear factor‐κ B ligand; RBS, random blood sugar; ROS, reactive oxygen species; SASP, senescence‐associated secretory phenotype; SNP, single nucleotide polymorphisms; TNF‐α, tumor necrosis factor‐alpha; VD, vitamin D; WBC, white blood cell.
With the advancement of various saliva‐based methodologies, markers, and models for the clinical screening of diabetes and prediabetes, saliva has emerged as a promising medium for this purpose. Dentists may leverage noninvasive chairside techniques to screen or diagnose diabetes and collaborate effectively with internists to manage the oral health of diabetic patients. Studies have demonstrated that placental growth factor (PlGF) 59 in gingival crevicular fluid (GCF) and microbial components 60 in saliva are correlated with blood glucose levels. These findings offer a promising avenue for the noninvasive auxiliary diagnosis of DM. In addition, researchers have developed diagnostic models capable of screening for prediabetes and diabetes in patients with periodontitis, 61 demonstrating moderate to good discriminative ability. In the future, dental clinics may assume an increasingly vital role in diabetes screening.
2.2. Diabetes and dental implants
Dental implants represent an effective solution for the replacement of missing teeth; however, their success is contingent upon both the local periodontal conditions and the overall health of patients, particularly with respect to a history of diabetes. Ongoing discussions examine how diabetes influences dental implant outcomes, with some researchers suggesting that diabetes may lead to complications surrounding implants and impede bone healing, ultimately resulting in a lower surgical success rate. 109 , 110 , 111 Even if the initial success rates for implants in diabetic individuals can be quite high, the long‐term results often seem less promising. 112 Conversely, other studies report differing results, indicating that the implant success rate remains within an acceptable range. 113 , 114 , 115 , 116 , 117 , 118 This inconsistency may stem from variations in diagnostic criteria and other influencing factors, particularly differences in the glycemic control of the studied patients. 38 , 39 , 40 , 42 , 119 The evidence derived from two recently published meta‐analyses indicates that the management of blood glucose levels is a critical factor influencing the success of implants in diabetic patients. 41 , 120
The mechanisms through which diabetes influences dental implants are analogous to its effects on osteogenesis and osteoclastogenesis. 121 A review conducted by de Oliveira et al. delineated these mechanisms as follows: (1) disrupting the balance between bone resorption and synthesis; (2) inducing microvascular disease; and (3) diminishing markers of bone formation while affecting collagen structure. 122 Furthermore, AGEs‐related NOX (NADPH oxidases)‐mediated oxidative stress significantly impairs bone healing in diabetic patients. 123
Future improvements in the success rates of dental implants for diabetic patients are expected to focus on enhancing implant material properties, 37 refining implant coatings, 124 and advancing surgical techniques. 125
2.3. Diabetes and apical periodontitis
AP manifests at the apex of the tooth root, leading to inflammation in both dental and periodontal tissues. Root canal therapy (RCT) serves as the primary treatment modality. Although evidence remains limited, existing studies indicate a positive correlation between diabetes and the prevalence of AP lesions. 43 Poor blood glucose control can lead to higher rates of AP and increased failure rates of RCT. 126 , 127 , 128 , 129 The impact of RCT on blood glucose management in diabetic patients is still under debate. 130 , 131 , 132 The discrepancies in findings may be attributed to differences in criteria, limited sample sizes, or varying follow‐up periods. Further well‐structured, large‐scale clinical trials are needed.
Existing evidence suggests that diabetes may exacerbate both the incidence and progression of AP by modulating levels of inflammatory factors, oxidative stress, and the prevalence of Candida albicans (C. albicans) within periodontal tissues. Several animal studies have underscored the significant roles of interleukin‐6 (IL‐6), tumor necrosis factor‐alpha (TNF‐α), and interleukin‐17 (IL‐17) in the pathogenesis and progression of both diabetes and AP. 68 , 133 Furthermore, diabetes is known to disrupt the antioxidant balance by elevating malondialdehyde (MDA) and uric acid levels while concurrently decreasing albumin concentrations. The presence of AP exacerbates these diabetic effects, leading to further reductions in albumin and increases in uric acid levels. 134 Additionally, another investigation demonstrated that the presence of C. albicans in type 2 diabetes mellitus (T2DM) individuals correlates with a higher incidence of AP. 135
2.4. Diabetes and tooth extraction
Persistent hyperglycemia and chronic inflammation associated with DM can adversely affect the healing process of extraction sockets. 136 , 137 , 138 This underscores the importance of blood glucose control for diabetic patients undergoing tooth extraction. However, many oral surgeons remain uncertain about the critical thresholds for blood glucose and HbA1c levels, as well as the point at which the risk of adverse complications significantly escalates. 139 A systematic review has provided new insights, indicating that a fasting blood glucose level of 240 mg/dL serves as the critical threshold for any dental treatment, as warning signs of diabetes begin to manifest at this level. For diabetic patients, the maximum acceptable blood glucose levels prior to tooth extraction are 180 mg/dL before meals and 234 mg/dL 2 h postprandially. 140 Moreover, the use of prophylactic antibiotics is not sufficiently supported by evidence. T2DM does not necessitate prophylactic antibiotics prior to tooth extraction in the absence of acute odontogenic infections. 138 A systematic review indicates that there is currently no scientific evidence to substantiate the efficacy of prophylactic antibiotic use prior to dental surgery in patients with diabetes. 141
The characteristics of diabetic wounds encompass elevated levels of ROS, impaired M1/M2 macrophage polarization, and chronic inflammation driven by proinflammatory chemokines. 139 The challenges associated with healing postextraction wounds are linked to diminished osteogenic differentiation of mesenchymal stem cells (MSC), 142 activation of matrix metalloproteinase‐9 (MMP‐9), persistent imbalance in the receptor activator of nuclear factor‐κ B ligand (RANKL)/osteoprotegerin (OPG) ratio. 143 Furthermore, the hyperglycemic environment disrupts the secretion of cytokines such as TNF‐α, IL‐6, and IL‐1β from macrophages, 144 resulting in functional impairments in neutrophils during the inflammatory response stages of wound healing, including migration, chemotaxis, and adhesion. 138
2.5. Diabetes and head and neck cancer
HNCs encompass a range of malignancies originating in regions such as the oral cavity, pharynx, larynx, paranasal sinuses, nasal cavity, salivary glands, and lymph nodes within the head and neck area. 145 Among these, cancers directly impacting the oral cavity and adjacent areas, such as oral squamous cell carcinoma (OSCC) and oropharyngeal carcinoma, are of particular concern due to their profound implications for oral health and systemic well‐being. Besides, for advanced‐stage cancers, the application of high‐energy radiation can lead to various potentially severe oral complications, including reduced salivary secretion causing xerostomia, oral pain, bacterial and fungal infections, taste disturbances, swallowing difficulties, discomfort, bleeding of periodontal tissues, and speech impairments. 146 , 147 This section focuses on the relationship between the aforementioned cancers that directly affect oral health and chronic diseases, as well as the impact of cancer treatments and medications on chronic conditions.
DM has been associated with an increased risk of developing various cancers, including HNC. 46 , 47 , 148 T2DM promotes proliferation, metastasis, and inhibits apoptosis in OSCC. 149 Patients with oral and oropharyngeal cancers who have a history of diabetes may have lower survival rates. 150
Researches indicate that antidiabetic medications such as metformin, 46 pioglitazone, 151 and SGLT‐2 inhibitors 152 , 153 exhibit antitumor effects. A review has elucidated the mechanisms of action of SGLT‐2 inhibitors and their applications in the management of type 2 diabetes and its associated complications. Both SGLT1 and SGLT2 are expressed in various tumors, where they facilitate euglycemic glycolysis by supplying tumor cells with glucose. Furthermore, the proliferation of carcinomas expressing SGLT2 can be effectively inhibited through the administration of an SGLT2 inhibitor. 154 Besides, the effects ofGLP‐1 receptor agonists (GLP‐1RAs) on tumors remain ambiguous, with some studies suggesting a potential increase 155 , 156 in cancer risk and others indicating otherwise. 157 , 158 Additional experiments are warranted to investigate.
The association between diabetes and HNC may be attributed to shared risk factors inherent to both conditions. 159 A review published in 2020 delineated the potential mechanisms by which diabetes may influence the occurrence, metastasis, and prognosis occ. These mechanisms include hyperglycemia, hyperinsulinemia, insulin resistance, chronic inflammation, and immune dysfunction. 46
2.6. Diabetes and salivary gland diseases
In recent years, accumulating evidence has established a robust association between salivary gland diseases and diabetes. 160 Salivary gland dysfunction in diabetic patients is predominantly characterized by impaired salivary secretion, resulting in diminished saliva flow, a sensation of dry mouth, and an elevated risk of dental caries. 161 , 162 Considering that the management of xerostomia should prioritize addressing its underlying causes, 163 effective blood glucose control is essential for diabetic patients experiencing this condition. When indicated, local saliva substitutes and/or stimulants may be utilized as adjunctive therapies.
Nitric oxide synthase (NOS) and its cofactor tetrahydrobiopterin (BH4) have been identified as promising targets for mitigating the reduced salivary secretion associated with diabetes‐induced xerostomia. 164 Immunohistochemical analyses of diabetic rats further elucidate that inflammation and oxidative stress are critical contributors to the progression of this condition. 165 Additionally, acinar cell vacuolation, 166 intracellular structural damage, 167 and dysfunction of the cholinergic vasodilation pathway 168 have been implicated as potential mechanism.
Novel approaches have emerged to alleviate xerostomia and enhance salivary secretion in diabetic patients. Wu et al. reported that sialography‐guided injection of pancreatic lipase into the salivary glands can effectively mitigate diabetes‐related chronic obstructive parotitis. 169 Additionally, Muhamed et al. confirmed the efficacy of a topical saliva stimulant spray containing 1% malic acid for treating xerostomia in patients with T2DM. 170 Furthermore, animal studies have demonstrated that both atropine and metformin can ameliorate salivary gland damage in diabetic rats and alleviate symptoms of xerostomia, with effects being particularly pronounced when used in combination. 171 These findings may offer new insights and strategies for the clinical management of diabetic xerostomia.
2.7. Diabetes and dental caries
Diabetic patients exhibit a heightened risk of developing dental caries, 172 which is influenced by their glycemic control and the duration of diabetes. 173 Two meta‐analyses have explored the relationship between diabetes and dental caries. One analysis revealed that the overall prevalence of dental caries in children and adolescents with type 1 diabetes was 67%, with the highest prevalence observed in South America and the lowest among patients maintaining good metabolic control. 174 The other study indicated that type 2 diabetes may contribute to an increase in the incidence of caries among adults. 50
The mechanisms underlying the association between diabetes and dental caries remain inadequately explored; however, they may be related to the effects of diabetes on saliva flow rate and buffering capacity, as well as alterations in the oral microbiota of affected individuals. Research has demonstrated that individuals with diabetes exhibit elevated levels of Lactobacillus alongside diminished saliva flow and buffering capacity. These factors facilitate the proliferation of Streptococcus mutans, thereby increasing the risk of dental caries. 175 , 176
2.8. Diabetes and root fracture
Root fracture refers to a break or crack in the root of a tooth. The incidence of vertical root fracture (VRF) in diabetic patients is 2.67 times higher than that observed in nondiabetic individuals. 177 Furthermore, the resistance to root fracture in the premolars of diabetic patients is significantly lower compared to their nondiabetic counterparts. 178
The impact of diabetes on the physiological structure of teeth may be related to the increased incidence of root fracture in diabetic patients. Research has found that diabetes can disrupt enamel development, leading to alterations in its microstructure and mechanical properties. 179 Additionally, diabetes affects the nanostructure of dentin, with concentrations of elements such as magnesium, zinc, strontium, lithium, manganese, and selenium being significantly lower than those in nondiabetic patients, while copper concentrations are higher in diabetic patients. 180
3. RHEUMATOID ARTHRITIS
RA is a chronic systemic autoimmune disorder that primarily targets the joints, resulting in pain, stiffness, and a decline in joint function. 181 Patients with RA exhibit a heightened incidence of dental caries, pulpitis, gingivitis, periodontitis, and oral ulcers. 182 The oral health‐related quality of life (OHRQoL) in patients with RA is compromised, influenced by factors such as the type of RA and the severity of periodontitis. 183 , 184 Consequently, understanding the relationship between RA and oral health, along with the underlying mechanisms, is crucial for the prevention and management of oral diseases in RA patients and may contribute to enhanced overall health outcomes.
To provide readers with a concise overview of the connections between RA and oral diseases, we summarize recent findings from relevant clinical studies in the table, highlighting key factors involved (Table 3).
TABLE 3.
Clinical trials related to rheumatoid arthritis (RA) and oral health.
| Diseases | Type of study | Aim | Sample | Sample | Molecule | Conclusions |
|---|---|---|---|---|---|---|
| Periodontitis | Cross‐sectional study | Evaluate the relationship between periodontal parameters and the presence and levels of ACPAs. | 164 RA patients | Blood | ACPA | In RA, the severity of periodontal conditions is linearly correlated with the presence and levels of ACPAs. 185 |
| Retrospective cross‐sectional study | Assess the production of NETs in patients with periodontitis and RA and their relationship with clinical parameters. | Early RA (n = 24), established RA (n = 64) and individuals without RA (n = 76) | Saliva and plasma | NETs | NETs may link PD and RA, with periodontal treatment significantly altering circulating NET levels. 186 | |
| Cross‐sectional study | Investigate whether serum levels of TREM‐1 and PGLYRP1 are associated with periodontitis in patients with RA. | 154 participants with RA (n = 55), Behcet's disease (n = 41) and healthy controls (n = 58) | Serum and saliva | TREM‐1 and PGLYRP1 | Elevated serum TREM‐1 is associated with PD and disease activity in RA. 187 | |
| Cross‐sectional study | Examine the effects of periodontitis and RA on the serum and saliva concentrations of MCP‐1, MIF, and fractalkine. | Periodontitis (n = 21), or with RA (n = 23), or with both diseases (n = 23), systemically and periodontally healthy individuals (n = 22) | Saliva and serum | MCP‐1, MIF, fractalkine | In RA, saliva shows elevated levels of MCP‐1, MIF, and fractalkine. 188 | |
| Case–control study | Investigate the genetic variations of PTPN22, PADI4, and CTLA4 and their impacts on RA and periodontitis. | 111 RA patients and 256 systemically healthy controls | Blood, plaque | PTPN22, PADI4, CTLA4 | Genetic variations may suggest a potential link between periodontitis and RA. 189 | |
| Cross‐sectional study | Investigate salivary and serum IgA ACPA in a population‐based cohort of elderly RA patients. | Patients with RA ≥ 61 years of age (n = 132) | Serum and saliva | Serum IgG ACPA and serum and saliva IgA ACPA | Serum and salivary IgA ACPA are not commonly found in RA patients with PD. 190 | |
| Retrospective cohort study | Explore the relationship between periodontal and serological indicators and disease activity in RA. | 127 patients with RA | Serum |
Anti‐agalactosyl immunoglobulin G |
PF is positively correlated with anti‐agalactosyl IgG titers, and both show a positive association with disease activity in RA. 191 | |
| Cross‐sectional study | Investigate the relationship between antibody titers against fibrinogen‐derived CCP and anti‐CEP‐1 in RA patients. | 107 patients with RA | Plasma and plaque | Anti‐CCP and anti‐CEP‐1 antibodies | In RA, PD may be a secondary risk factor for anti‐CCP positivity. 192 | |
| Case–control study | Investigate whether the association between periodontitis and RA is influenced by SNPs in the genes encoding PAD2 and PAD4. | 137 RA patients and 161 controls with self‐reported periodontitis | Blood | rs2057094、rs2076616、rs2235912 | Carriers of the alleles for SNPs rs2057094, rs2076616, and rs2235912 in the PADI2 gene may have an increased risk of developing RA in patients with periodontitis. 193 | |
| Case–control study | Quantify the relationship between periodontal clinical indicators, ABL, concentrations of antibodies against Porphyromonas gingivalis (P. gingivalis), P. intermedia, and Fusobacterium nucleatum (F. nucleatum), and the concentration of anti‐MAA antibodies. | (n = 284 RA cases, n = 330 OA controls) | Plasma | anti‐MAA antibodies | MAA may play a role in the interaction between periodontal tissues and RA. 194 | |
| Case‐controlled clinical trial | Investigate the levels of PRL in GCF, synovial fluid, and serum of patients with moderate active RA, both with and without periodontitis. | 80 | GCF, synovial fluid, and plasma | PRL | Local PRL levels in GCF and synovial fluid seem to be associated with the disease processes of periodontitis and RA, compared to serum levels. 195 | |
| Sjögren's syndrome | Cross‐sectional research | Investigate the relationship between NLRP3 gene polymorphisms and patients with RA and primary SS. | A total of 239 patients with RA, 285 patients with primary SS, and 170 controls | Blood | NLRP3 gene polymorphism | The NLRP3 genotype may affect clinical outcomes and progression in RA and primary SS. The activity of the NLRP3 inflammasome may explain the severity of these diseases. 196 |
Abbreviations: ABL, alveolar bone loss; ACPA, anti‐citrullinated protein antibody; anti‐CCP, anti‐cyclic citrullinated peptides; anti‐CEP‐1, anti‐citrullinated α‐enolase peptides; ARE, arylesterase; CMV, cytomegalovirus; EBV, Epstein–Barr virus; GCF, gingival crevicular fluid; MAA, malondialdehyde‐acetaldehyde; MCP‐1, monocyte chemoattractant protein‐1; MIF, migration inhibitory factor; NETs, neutrophil extracellular traps; OSI, oxidative stress index; PD, periodontitis; PGLYRP1, peptidoglycan recognition protein 1; PRL, prolactin; SNP, single nucleotide polymorphism; SS, Sjögren's syndrome; TAS, total antioxidant status; TMD, temporomandibular disorders; TOS, total oxidative status; TREM‐1, triggering receptor expressed on myeloid cells 1.
3.1. RA and periodontitis
Over the past decade, numerous studies worldwide have confirmed the correlation between RA and periodontitis. 197 , 198 , 199 , 200 On one hand, certain RA medications appear to elevate the risk of periodontal inflammation and exacerbate periodontitis. 201 , 202 Conversely, periodontal treatment has been shown to reduce RA activity. 181 , 203 , 204 The mechanisms by which RA influences periodontitis primarily involve microbial factors, inflammatory mediators, and genetic associations (Figure 3).
FIGURE 3.
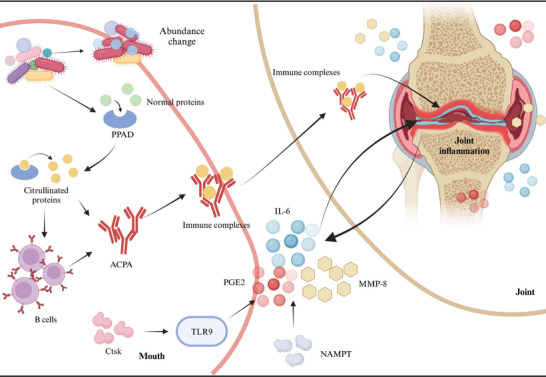
Mechanisms linking oral health and rheumatoid arthritis. Microorganisms such as Porphyromonas gingivalis (P. gingivalis) produce PPAD, which citrullinates proteins and stimulates B cells to generate ACPAs. These ACPAs form immune complexes that accumulate in the joints, contributing to the pathogenesis of rheumatoid arthritis. Additionally, NAMPT and Ctsk trigger inflammatory responses through distinct pathways, elevating levels of inflammatory cytokines and MMP‐8, ultimately leading to joint tissue damage. Furthermore, the composition of oral bacteria is altered in patients with rheumatoid arthritis. ACPA, anti‐citrullinated protein antibodies; Ctsk, cathepsin K; IL‐6, interleukin‐6; MMP‐8, matrix metalloproteinase 8; NAMPT, nicotinamide phosphoribosyl transferase; PGE2, prostaglandin E2; PPAD, P. gingivalis peptidyl arginine deiminase. Created with BioRender.com.
Patients with periodontitis and RA often exhibit an abnormal abundance of specific microorganisms, 205 , 206 along with limited variation in microbial taxa and gene functions between deep and shallow subgingival sites. 207 These findings suggest that RA may influence the development and progression of periodontitis through alterations in the microbiome. Furthermore, specific oral pathogens such as Porphyromonas gingivalis (P. gingivalis) produce peptidyl arginine deiminase (PPAD), 208 which can citrullinate proteins, resulting in the formation of citrullinated autogenic antigens (CPAs) and subsequently leading to the production of anti‐citrullinated protein antibodies (ACPAs). 209
Furthermore, RA and periodontitis share common molecular mediators, such as MMP‐8, IL‐6, and prostaglandin E2. 210 , 211 These same mediators may play a role in their interaction. RA can also influence periodontitis by regulating inflammatory factors through various upstream mediators. Studies have shown that nicotinamide phosphoribosyl transferase (NAMPT) expression is upregulated in the periodontal ligament tissues of RA mice, resulting in elevated levels of proinflammatory cytokines (IL‐6), chemokines (IL‐8, CCL5), and inflammatory mediators such as COX‐2, MMP‐1, and MMP‐3 in periodontal ligament cells. 212 Another study suggests that cathepsin K (Ctsk) influences the infiltration of dendritic cells and T cells, as well as the production of inflammatory factors through the TLR9 signaling pathway, serving as a key pathological regulator in both RA and periodontitis. This mechanism contributes to enhanced erosion of periodontal bone and knee cartilage. 213
In addition to the aforementioned microbial and inflammatory factors, other studies have explored genetic associations. It was found that IL‐1α‐889 C/IL‐1β‐511a is positively correlated with RA. 214 Furthermore, another study indicated that a high incidence and severity of periodontitis in first‐degree relatives (FDRs) of RA patients are associated with seropositivity for ACPAs, further supporting the hypothesis that periodontitis may serve as a risk factor for the development of RA. 215
3.2. RA and other oral diseases
3.2.1. Temporomandibular disorders
Many patients with RA exhibit clinical manifestations of temporomandibular joint (TMJ) inflammation, with the most common symptoms including pain in the TMJ area during movement or stress, joint clicking, and impaired mandibular function. 216 A large‐scale clinical study in Taiwan found that the risk of temporomandibular disorders (TMD) in patients with RA is 2.538 times higher than that in non‐RA patients. 217 Bone resorption occurs within the TMJ of RA patients, potentially mediated by TNF through synovial fluid. 218 In terms of treatment, animal studies have demonstrated that bone marrow mesenchymal stem cells (BMSCs) significantly enhance the healing of TMJs in rats with induced RA. 219
3.2.2. Sjögren syndrome and xerostomia
It has been reported that 51% of patients with RA experience dry mouth, and a statistically significant relationship exists between dry mouth and poor OHRQoL. The rates of whole‐mouth saliva at rest and stimulated parotid saliva flow in RA patients are significantly lower than those observed in non‐RA individuals. 220 The OHRQoL of RA patients is adversely affected by dry mouth syndrome, which subsequently impacts their overall quality of life. 184 Regarding the underlying mechanism, a case–control study was conducted to investigate the role of viruses in the association between RA and Sjögren's syndrome (SS), revealing that Epstein–Barr virus (EBV) is more prevalent among RA patients and correlates with Schirmer test results. 221
3.2.3. Dental caries and apical periodontitis
It has been observed that patients with RA exhibit a higher frequency and severity of dental plaque, with significantly elevated counts of S. mutans in the RA group. 222 There may also be an association between increased levels of systemic inflammatory cytokines induced by RA and AP. A cross‐sectional study demonstrated that RA is significantly associated with a higher prevalence of AP, indicating that RA patients are more likely to develop this condition. However, RA does not appear to influence the outcomes of RCT. 223
4. CARDIOVASCULAR DISEASES
CVDs, encompassing conditions such as ischemic heart disease, stroke, heart failure, peripheral artery disease, and various other cardiac and vascular disorders, represent a leading cause of mortality worldwide and significantly impair quality of life. 224 , 225 In 2019, CVDs accounted for 33% of all global deaths, with ischemic heart disease (9.1 million deaths) and stroke (6.6 million deaths) collectively representing 85% of fatalities related to CVDs. 226 There is a strong association between CVDs and oral health, particularly through the link between atherosclerosis and periodontitis. Additionally, an interplay exists between hypertension and periodontitis. Furthermore, patients with CVDs frequently exhibit higher rates of dental caries and tooth loss.
Consequently, it is imperative to underscore the critical role of clinical practitioners, dental professionals, and other healthcare providers in comprehending the relationship between periodontal disease and CVDs, identifying their risk factors, and recognizing the urgent need for timely referrals to specialized dental or periodontal care. Mitigating the prevalence and incidence of periodontal disease may contribute to a reduction in the associated risks of systemic diseases.
4.1. Atherosclerotic vascular disease and periodontal diseases
Atherosclerotic vascular disease (ASVD) is a chronic condition characterized by the accumulation of lipids, cholesterol, and other substances within the arterial walls, leading to the formation of atherosclerotic plaques. 227 There is a significant increase in risk associated with chronic periodontitis and ASVD, independent of other established cardiovascular risk factors. 228 Meta‐analyses encompassing prospective cohort studies, case–control studies, and cross‐sectional studies consistently demonstrate a markedly elevated risk of coronary heart disease (CHD) in patients with periodontal disease. 7 Furthermore, periodontal disease increases the incidence of myocardial infarction by two to four times, 229 while severe periodontal disease can elevate the risk of stroke by 3.5%. 230
The underlying mechanisms linking ASVD and periodontitis primarily involve infection, molecular mimicry, and systemic inflammation (Figure 4). 231 Furthermore, numerous lines of evidence suggest a potential association between P. gingivalis and atherosclerotic diseases related to periodontal disease. First, P. gingivalis can invade cardiovascular cells, 232 with its distant invasion correlating with an increased risk of acute myocardial infarction, 233 indicating that it may exacerbate the severity of coronary artery disease through the induction of systemic inflammation. Second, P. gingivalis degrades platelet endothelial cell adhesion molecules (PECAM‐1) and vascular endothelial cadherin (VE‐cadherin), compromising the integrity of the endothelial barrier and enhancing vascular permeability. 234 This disruption may promote platelet aggregation and the release of proinflammatory cytokines, potentially accelerating the progression of atherosclerosis. 235 Additionally, the presence of P. gingivalis is often associated with significantly elevated levels of antibodies against human heat shock protein 60 (HSP60). 236 Under conditions characterized by endothelial dysfunction, HSP60 expression is observed; its epitopes share similarities with GroEL protein from P. gingivalis, 237 which may lead to cross‐reactivity that further exacerbates endothelial damage and accelerates atherosclerosis.
FIGURE 4.
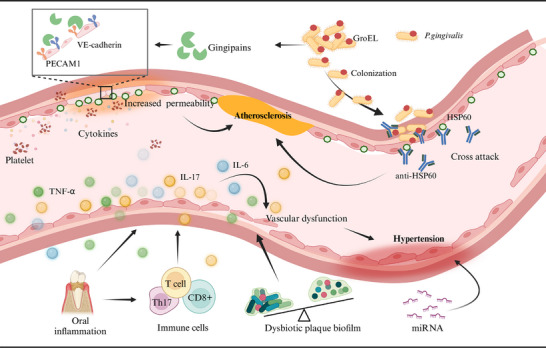
Mechanisms linking oral health and cardiovascular diseases. Atherosclerosis: Porphyromonas gingivalis (P. gingivalis) contains GroEL protein, which shares structural similarities with the HSP60 epitopes expressed by vascular endothelial cells. Consequently, antibodies against HSP60 may inadvertently target and damage these endothelial cells, thereby promoting the development of atherosclerosis. Additionally, P. gingivalis produces gingipains that degrade PECAM‐1 and VE‐cadherin, disrupting the integrity of the endothelial barrier, increasing permeability, promoting platelet aggregation, and triggering the release of proinflammatory cytokines—factors that may accelerate the progression of atherosclerosis. Created with BioRender.com. Hypertension: The inflammatory environment within the oral cavity releases cytokines such as TNF‐α, IL‐6, and IL‐17, which can impair endothelial function and contribute to hypertension. Furthermore, this inflammatory milieu activates various immune cells, exacerbating cytokine release and resulting in vascular dysfunction. Additionally, dysbiosis of the oral microbiota may also be associated with hypertension. HSP60, heat shock protein 60; IL‐6, interleukin‐6; IL‐17, interleukin‐17; PECAM1, platelet endothelial cell adhesion molecule; TNF‐α, tumor necrosis factor‐alpha; VE‐cadherin, vascular endothelial cadherin; WBC, white blood cell. Created with BioRender.com.
4.2. Hypertension and periodontal diseases
Hypertension is a prevalent risk factor for CVDs, affecting approximately 45% of the global population, with prevalence rates increasing with age. 238 Notably, about 50% of hypertensive patients fail to achieve effective blood pressure control. 239 , 240 This high prevalence can largely be attributed to a lack of public awareness regarding the classic triggers of hyperadherence to treatment recommendations among patients. 241 However, it is crucial to consider that nonclassical cardiovascular risk factors, such as periodontitis, may also contribute to the onset and poor management of hypertension. 242
Clinical data and systematic reviews indicate that patients with periodontal disease exhibit significantly higher systolic and diastolic blood pressure compared to those without the condition, 243 with a notable association between moderate to severe periodontal disease and an increased risk of hypertension. 244 Furthermore, there is a significant correlation among periodontal disease, the number of missing teeth, and the experience of basic periodontal treatment concerning future incidence of hypertension. 245 Despite considerable heterogeneity across studies, current evidence suggests that periodontal treatment is associated with a marked reduction in C‐reactive protein (CRP) levels and an improvement in endothelial function, along with varying degrees of blood pressure reduction. 11 , 246 , 247
The pathogenesis of hypertension in patients with periodontitis is complex and not yet fully elucidated, involving multiple interconnected mechanisms. For instance, inflammatory responses characterized by elevated levels of inflammatory molecules during periodontitis impair endothelial function and contribute to increased blood pressure (Figure 4). 241 , 248 , 249 Immune cell responses are also significant; activated T cells migrate to vascular tissues, releasing proinflammatory cytokines that lead to vascular dysfunction. 249 , 250 , 251 Additionally, microbial dysbiosis in the oral cavity, marked by pathogenic bacteria associated with periodontitis, correlates with elevated blood pressure. 252 , 253 , 254 Finally, noncoding RNAs, particularly microRNAs, may serve as epigenetic regulators linking periodontitis and hypertension. 255
4.3. Other oral diseases
In addition to periodontitis, patients with CVDs demonstrate a higher incidence of dental caries and tooth loss. 228 , 256 , 257 The loss of five or more teeth is significantly associated with an increased risk of CHD events and acute myocardial infarction. When the number of missing teeth reaches nine or more, there is a notable association with the risk of CVDs, diabetes, and all‐cause mortality. 258 A meta‐analysis revealed a linear relationship between tooth loss and CHD mortality. 259
5. CHRONIC RESPIRATORY DISEASES
The primary function of the respiratory system is to facilitate the exchange of oxygen and carbon dioxide, thereby supporting the metabolic activities of the body's cells. Common respiratory diseases include chronic obstructive pulmonary disease (COPD), asthma, and pneumonia. According to the 2019 Global Burden of Disease study, chronic respiratory diseases ranked as the third leading cause of death, accounting for 4 million fatalities worldwide and affecting approximately 454.6 million cases (ranging from 417.4 to 499.1 million). 260
The oral cavity is anatomically connected to the upper respiratory tract, and as air and food traverse the mouth into the pharynx, pathogens or inflammatory substances may enter the throat or lungs, potentially triggering or exacerbating respiratory diseases such as pneumonia, COPD, asthma, and lung cancer. 261 Studies have demonstrated a significant degree of similarity between the oral and lung microbiomes in healthy individuals. 262
Research shows that oral diseases are closely associated with various lung diseases, such as asthma, COPD, pulmonary fibrosis, and pneumonia. 263 , 264 Patients with chronic respiratory diseases show a declining trend in OHRQoL. 265
5.1. COPD
Patients with COPD often exhibit poorer oral health, as evidenced by worse periodontal status, higher plaque indices, and elevated DMFT (decayed, missing, filled teeth) scores. 266 Poor oral conditions or diseases, such as periodontitis, 267 , 268 dental caries, 264 and tooth loss 269 can exacerbate airflow limitation in COPD patients, worsening daily respiratory symptoms like coughing and wheezing and potentially contributing to acute exacerbations that lead to increased hospitalization rates and higher mortality. Direct evidence demonstrating that oral care interventions can improve outcomes in COPD is currently limited; however, two small‐scale trials have suggested that periodontal treatment may reduce the frequency of COPD exacerbations. 12 , 270
Research on the mechanisms linking COPD and various oral diseases is limited, with many studies conducted using animal models. These mechanisms may involve immune responses, microbial factors, and ferroptosis (Figure 5). Mutual exacerbation of periodontitis and COPD is associated with the activation of γδ T cells and M2 macrophages, ultimately leading to increased expression of IL‐17 and interferon gamma (IFN‐γ), as well as M2 macrophage polarization. 271 Furthermore, P. gingivalis or Fusobacterium nucleatum (F. nucleatum) promoted the development of COPD and impaired lung function in mice. 272 Studies have also shown that periodontitis accelerates the progression of COPD by upregulating ferroptosis in lung tissue. 273
FIGURE 5.

Mechanisms linking oral health and chronic respiratory diseases. Under specific conditions, oral bacteria can translocate to the respiratory tract and colonize the lungs. This may trigger immune and inflammatory responses, leading to the production of cytokines and MMPs that can damage lung tissue, potentially impacting oral tissues as well. Additionally, the expression of ferroptosis‐promoting genes such as Acsl4, Socs1, Ncoa4, and Ptgs2 are upregulated, inducing ferroptosis and contributing to chronic respiratory diseases. Furthermore, treatments for chronic respiratory diseases—such as inhaled corticosteroids—may increase plaque formation and reduce salivary flow rate, thereby elevating the risk of dental caries. Acsl4/Socs1/Ncoa4/Ptgs2, ferroptosis‐related genes; IFN‐γ, interferon‐gamma; IL‐6, interleukin‐6; IL‐17, interleukin‐17; MDA, malondialdehyde; MMP‐8, matrix metalloproteinase 8; TNF‐α, tumor necrosis factor‐alpha. Created with BioRender.com.
5.2. Bronchial asthma (asthma)
Patients with asthma exhibit altered salivary flow rates and composition, as well as poorer oral health, characterized by a higher prevalence of dental caries. 274 , 275 Medications, such as inhaled corticosteroid (ICS) therapy used to treat bronchial asthma are also associated with an increased incidence of dental caries. 276 The heightened risk of dental caries linked to ICS may be attributed to changes in salivary composition and flow rate. 277 Furthermore, clinical data and systematic reviews indicate that asthma patients may have an elevated risk of periodontitis 278 , 279 and tooth loss. 280
Currently, there is no conclusive evidence establishing a direct biological link between periodontitis and asthma. The prevailing theoretical framework posits that these two inflammatory diseases may influence one another through microbial interactions, inflammatory factors, and immune responses (Figure 5). Research has shown that the periodontal pathogen Prevotella can induce the production of matrix metalloproteinases (MMPs), which adversely affect both periodontitis and asthma. 281 Additionally, MMPs can be produced by various inflammatory cells in the respiratory tract, potentially exacerbating periodontal inflammation. 282 On the immunological front, periodontal pathogens activate host immune cells to produce cytokines such as prostaglandin E2 (PGE2), interferon‐γ, TNF‐α, and several interleukins (IL‐1, IL‐6, IL‐10, IL‐11). These cytokines stimulate macrophages and osteoclasts to release hydrolases and collagenases—enzymes that degrade collagen and elastic fibers in lung tissue—thereby contributing to bronchial remodeling processes in asthma. 283 Moreover, Th17 cells are implicated in various immune‐mediated inflammatory conditions such as psoriasis and RA; they serve as potent mediators of tissue inflammation. Interleukin 17A (IL‐17A) can activate a range of inflammatory cascades that mediate the development and progression of periodontitis along with related systemic chronic inflammatory diseases like asthma. 284
5.3. Pneumonia
Epidemiological studies have demonstrated a correlation between oral health issues and the risk of developing pneumonia. Data from the Korean national population indicate that oral health problems, such as dental caries and tooth loss, significantly increase the risk of pneumonia; frequent tooth brushing and regular professional dental cleanings are associated with a reduced incidence of this condition. 285 In specific populations, including intensive care unit (ICU) patients, 286 adults with severe and complex neurological disorders, 287 postoperative cancer patients, 288 and acute stroke patients, 289 professional oral care has been linked to a decrease in pneumonia incidence. When examining specific types of pneumonia, evidence supporting the link between oral health is more consistent for hospital‐acquired pneumonia (HAP), 290 , 291 whereas the association with community‐acquired pneumonia (CAP) remains controversial. 292 , 293 , 294 , 295
Regarding the potential mechanisms linking oral health to the development of various types of pneumonia, Kim et al. proposed that the oral environment can serve as a reservoir for pneumonia pathogens, which may be aspirated into the lower respiratory tract under certain conditions, thereby creating a favorable environment for pneumonia development. 293 Recent studies have reaffirmed that oral bacteria can act as a source of infection in aspiration pneumonia, with the quantity of oral bacteria identified as a significant risk factor for this condition. 296 , 297 Furthermore, inflammatory cytokines induced by oral inflammatory diseases such as periodontitis play a crucial role in pneumonia pathogenesis. 298 Recent animal experiments have demonstrated that P. gingivalis induces pneumonia in mice with periodontitis, significantly increasing levels of cytokines and neutrophils in peripheral blood and lung tissue. 299 A recent study innovatively transplanted human oral commensal microbiota into germ‐free mice to create human oral microbiota‐associated (HOMA) mice; this study analyzed the impact of oral microbiota on lung immunity and systemic conditions during acute lung injury and acute respiratory distress syndrome (ALI/ARDS). 300 The results indicated that HOMA mice exhibited systemic dysbiosis; compared to conventional (CNV) mice with sufficient microbial diversity, HOMA mice developed more severe ALI.
Mouthwash is a critical component of oral hygiene, and chlorhexidine mouthwash has been shown to reduce the incidence of respiratory infections; however, long‐term use may result in side effects including altered taste, dry mouth, and tooth discoloration. Over the past decade, research has increasingly focused on exploring new mouthwashes derived from natural products. A study comparing a 6.66% clove extract mouthwash with a 0.2% chlorhexidine mouthwash demonstrated that the control group had a 2.06‐fold higher risk of developing ventilator‐associated pneumonia (VAP) than the intervention group. 13 Additionally, a triple‐blind randomized controlled trial investigating the effects of propolis mouthwash revealed that the intervention group experienced significantly lower incidences of VAP on days 3, 5, and 7 compared to the control group. Propolis mouthwash may represent a viable alternative to chlorhexidine for patients in ICU. 301
6. CONCLUSION
Chronic diseases and oral health are intricately linked, as conditions such as periodontitis, dental caries, and AP can potentially increase the risk of chronic illnesses through pathways like systemic inflammation and pathogen transmission. Addressing oral hygiene is not only crucial for dental health but also plays a significant role in reducing the burden of chronic diseases. Improving oral health management, raising public awareness, and providing accessible and cost‐effective dental care can have a profound impact on public health outcomes. Medical institutions should consider integrating oral health into comprehensive patient care for individuals with CVDs, particularly during rehabilitation, by incorporating oral health education and preventive care. This holistic approach could mitigate long‐term risks while enhancing the overall quality of life for these patients.
The intricate and intimate connection between chronic diseases and oral health offers an extensive array of exploration prospects for future research and clinical practice. Future research, for the first, will focus on uncovering the underlying mechanisms of these interactions, with the goal of identifying new therapeutic targets. For example, mechanistic studies on diabetes and periodontitis suggest future drug targets may involve proresolving pathways, host response modulation, Th17/Treg imbalance, antioxidant therapy, immune training, and genetic modifications. 302 , 303 The integration of emerging technologies, such as multiomics approaches and artificial intelligence (AI), will be crucial for discovering new mechanism. 304 , 305 In the future, noninvasive diagnostic tools, such as saliva‐based rapid detection and continuous monitoring devices, will enable early detection and ongoing management of oral health issues linked to chronic diseases. 306 , 307
AUTHOR CONTRIBUTIONS
Di Fu: conception of the work; interpretation of data for the work; drafting the work. Xingyue Shu: conception and design of the work; Substantial contributions to acquisition and analysis of data for the work. Ge Zhou: revised the manuscript. Mengzhen Ji: revised the manuscript. Ga Liao: contributions to acquisition and analysis of data for the work; revised the manuscript critically for important intellectual content. Ling Zou: conception and design of the work; revising it critically for important intellectual content; acquisition of fundings. All the authors have read and approved the final manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS STATEMENT
Not applicable.
ACKNOWLEDGMENTS
Image created with Biorender.com, with permission. This work was supported by grants from the National Natural Science Foundation of China (Grant No. 82071111), Project of the Science and Technology Department of Sichuan Province (Grant No. 2024YFHZ0042), and the Clinical Research Program, West China Hospital of Stomatology Sichuan University (Grant no. LCYJ‐MS‐202310).
Fu D, Shu X, Zhou G, Ji M, Liao G, Zou L. Connection between oral health and chronic diseases. MedComm. 2025;6:e70052. 10.1002/mco2.70052
DATA AVAILABILITY STATEMENT
Data availability is not applicable to this review as no new data were created or analyzed in this review.
REFERENCES
- 1. Network GBoDC . Global Burden of Disease Study 2019 (GBD 2019) Results. Institute for Health Metrics and Evaluation – IHME; 2020. [Google Scholar]
- 2. Prevention CfDCa . Chronic Disease Prevention and Health Promotion. Chronic Disease Overview. Centers for Disease Control and Prevention; 2017. [Google Scholar]
- 3. Waters HGM, ed. The Costs of Chronic Disease in the U.S. 1st ed. Milken Institute; 2018. [Google Scholar]
- 4. Bloom DE, Cafiero E, Jané‐Llopis E, et al. The Global Economic Burden of Noncommunicable Diseases. Program on the Global Demography of Aging; 2012. [Google Scholar]
- 5. Kane SF. The effects of oral health on systemic health. Gen Dent. 2017;65(6):30‐34. [PubMed] [Google Scholar]
- 6. Wu CZ, Yuan YH, Liu HH, et al. Epidemiologic relationship between periodontitis and type 2 diabetes mellitus. BMC Oral Health. 2020;20(1):204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Bahekar AA, Singh S, Saha S, et al. The prevalence and incidence of coronary heart disease is significantly increased in periodontitis: a meta‐analysis. Am Heart J. 2007;154(5):830‐837. [DOI] [PubMed] [Google Scholar]
- 8. Sanz M, Marco Del Castillo A, Jepsen S, et al. Periodontitis and cardiovascular diseases: consensus report. J Clin Periodontol. 2020;47(3):268‐288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Ferreira MKM, Ferreira RO, Castro MML, et al. Is there an association between asthma and periodontal disease among adults? Systematic review and meta‐analysis. Life Sci. 2019;223:74‐87. [DOI] [PubMed] [Google Scholar]
- 10. Preshaw PM, Taylor JJ, Jaedicke KM, et al. Treatment of periodontitis reduces systemic inflammation in type 2 diabetes. J Clin Periodontol. 2020;47(6):737‐746. [DOI] [PubMed] [Google Scholar]
- 11. Sharma S, Sridhar S, McIntosh A, et al. Periodontal therapy and treatment of hypertension‐alternative to the pharmacological approach. A systematic review and meta‐analysis. Pharmacol Res. 2021;166:105511. [DOI] [PubMed] [Google Scholar]
- 12. Apessos I, Voulgaris A, Agrafiotis M, et al. Effect of periodontal therapy on COPD outcomes: a systematic review. BMC Pulmon Med. 2021;21(1):92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Jahanshir M, Nobahar M, Ghorbani R, et al. Effect of clove mouthwash on the incidence of ventilator‐associated pneumonia in intensive care unit patients: a comparative randomized triple‐blind clinical trial. Clin Oral Investig. 2023;27(7):3589‐3600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Sanchez P, Everett B, Salamonson Y, et al. Oral health and cardiovascular care: perceptions of people with cardiovascular disease. PLoS One. 2017;12(7):e0181189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Alqadi SF. Diabetes mellitus and its influence on oral health: review. Diabetes Metab Syndr Obes. 2024;17:107‐120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Grisi DC, Vieira IV, de Almeida Lima AK, et al. The complex interrelationship between diabetes mellitus, oral diseases and general health. Curr Diabetes Rev. 2022;18(3):e220321192408. [DOI] [PubMed] [Google Scholar]
- 17. Ahmad R, Haque M. Oral health messiers: diabetes mellitus relevance. Diabetes Metab Syndr Obes. 2021;14:3001‐3015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Borgnakke WS, Genco RJ, Eke PI, et al. Oral Health and Diabetes. National Institute of Diabetes and Digestive and Kidney Diseases (US); 2021. [PubMed] [Google Scholar]
- 19. Negrini TC, Carlos IZ, Duque C, et al. Interplay among the oral microbiome, oral cavity conditions, the host immune response, diabetes mellitus, and its associated‐risk factors‐An overview. Front Oral Health. 2021;2:697428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Enteghad S, Shirban F, Nikbakht MH, et al. Relationship between diabetes mellitus and periodontal/peri‐implant disease: a contemporaneous review. Int Dent J. 2024;74(3):426‐445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Mirnic J, Djuric M, Brkic S, et al. Pathogenic mechanisms that may link periodontal disease and type 2 diabetes mellitus—the role of oxidative stress. Int J Mol Sci. 2024;25(18):9806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Vlachou S, Loumé A, Giannopoulou C, et al. Investigating the interplay: periodontal disease and type 1 diabetes mellitus—a comprehensive review of clinical studies. Int J Mol Sci. 2024;25(13):7299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Păunică I, Giurgiu M, Dumitriu AS, et al. The bidirectional relationship between periodontal disease and diabetes mellitus—a review. Diagnostics. 2023;13(4):681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Zhao M, Xie Y, Gao W, et al. Diabetes mellitus promotes susceptibility to periodontitis‐novel insight into the molecular mechanisms. Front Endocrinol. 2023;14:1192625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Nibali L, Gkranias N, Mainas G, et al. Periodontitis and implant complications in diabetes. Periodontol 2000. 2022;90(1):88‐105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Salhi L, Reners M. Update on the bidirectional link between diabetes and periodontitis. Adv Exp Med Biol. 2022;1373:231‐240. [DOI] [PubMed] [Google Scholar]
- 27. Genco RJ, Borgnakke WS. Diabetes as a potential risk for periodontitis: association studies. Periodontol 2000. 2020;83(1):40‐45. [DOI] [PubMed] [Google Scholar]
- 28. Genco RJ, Graziani F, Hasturk H. Effects of periodontal disease on glycemic control, complications, and incidence of diabetes mellitus. Periodontol 2000. 2020;83(1):59‐65. [DOI] [PubMed] [Google Scholar]
- 29. Graves DT, Ding Z, Yang Y. The impact of diabetes on periodontal diseases. Periodontol 2000. 2020;82(1):214‐224. [DOI] [PubMed] [Google Scholar]
- 30. Polak D, Sanui T, Nishimura F, et al. Diabetes as a risk factor for periodontal disease‐plausible mechanisms. Periodontol 2000. 2020;83(1):46‐58. [DOI] [PubMed] [Google Scholar]
- 31. Costa R, Ríos‐Carrasco B, Monteiro L, et al. Association between type 1 diabetes mellitus and periodontal diseases. J Clin Med. 2023;12(3):1147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Maia MB, Souza JGS, Bertolini M, et al. Knowledge of bidirectional relationship between diabetes and periodontal disease among diabetes patients: a systematic review. Int J Dent Hyg. 2023;21(1):28‐40. [DOI] [PubMed] [Google Scholar]
- 33. Nguyen ATM, Akhter R, Garde S, et al. The association of periodontal disease with the complications of diabetes mellitus. A systematic review. Diabetes Res Clin Pract. 2020;165:108244. [DOI] [PubMed] [Google Scholar]
- 34. Stöhr J, Barbaresko J, Neuenschwander M, et al. Bidirectional association between periodontal disease and diabetes mellitus: a systematic review and meta‐analysis of cohort studies. Sci Rep. 2021;11(1):13686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Baeza M, Morales A, Cisterna C, et al. Effect of periodontal treatment in patients with periodontitis and diabetes: systematic review and meta‐analysis. J Appl Oral Sci. 2020;28:e20190248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Zhang Z, Ji C, Wang D, et al. The burden of diabetes on the soft tissue seal surrounding the dental implants. Front Physiol. 2023;14:1136973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Vijay R, Mendhi J, Prasad K, et al. Carbon nanomaterials modified biomimetic dental implants for diabetic patients. Nanomaterials. 2021;11(11):2977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Bencze B, Cavalcante BGN, Romandini M, et al. Prediabetes and poorly controlled type‐2 diabetes as risk indicators for peri‐implant diseases: a systematic review and meta‐analysis. J Dent. 2024;146:105094. [DOI] [PubMed] [Google Scholar]
- 39. Al Ansari Y, Shahwan H, Chrcanovic BR. Diabetes mellitus and dental implants: a systematic review and meta‐analysis. Materials. 2022;15(9):3227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Andrade CAS, Paz JLC, de Melo GS, et al. Survival rate and peri‐implant evaluation of immediately loaded dental implants in individuals with type 2 diabetes mellitus: a systematic review and meta‐analysis. Clin Oral Investig. 2022;26(2):1797‐1810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Lv X, Zou L, Zhang X, et al. Effects of diabetes/hyperglycemia on peri‐implant biomarkers and clinical and radiographic outcomes in patients with dental implant restorations: a systematic review and meta‐analysis. Clin Oral Implants Res. 2022;33(12):1183‐1198. [DOI] [PubMed] [Google Scholar]
- 42. Shang R, Gao L. Impact of hyperglycemia on the rate of implant failure and peri‐implant parameters in patients with type 2 diabetes mellitus: systematic review and meta‐analysis. J Am Dent Assoc. 2021;152(3):189‐201.e181. [DOI] [PubMed] [Google Scholar]
- 43. Tibúrcio‐Machado CD, Bello MC, Maier J, et al. Influence of diabetes in the development of apical periodontitis: a critical literature review of human studies. J Endod. 2017;43(3):370‐376. [DOI] [PubMed] [Google Scholar]
- 44. Pérez‐Losada FL, Estrugo‐Devesa A, Castellanos‐Cosano L, et al. Apical periodontitis and diabetes mellitus type 2: a systematic review and meta‐analysis. J Clin Med. 2020;9(2):540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Liu X, He G, Qiu Z, et al. Diabetes mellitus increases the risk of apical periodontitis in endodontically‐treated teeth: a meta‐analysis from 15 studies. J Endod. 2023;49(12):1605‐1616. [DOI] [PubMed] [Google Scholar]
- 46. Wang X, Wang H, Zhang T, et al. Diabetes and its potential impact on head and neck oncogenesis. J Cancer. 2020;11(3):583‐591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Ramos‐Garcia P, Roca‐Rodriguez MDM, Aguilar‐Diosdado M, et al. Diabetes mellitus and oral cancer/oral potentially malignant disorders: a systematic review and meta‐analysis. Oral Dis. 2021;27(3):404‐421. [DOI] [PubMed] [Google Scholar]
- 48. Yan P, Wang Y, Yu X, et al. Type 2 diabetes mellitus and risk of head and neck cancer subtypes: a systematic review and meta‐analysis of observational studies. Acta Diabetol. 2021;58(5):549‐565. [DOI] [PubMed] [Google Scholar]
- 49. Pérez‐Ros P, Navarro‐Flores E, Julián‐Rochina I, et al. Changes in salivary amylase and glucose in diabetes: a scoping review. Diagnostics. 2021;11(3):453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Zhou G, Shu X, Long Y, et al. Dental caries and salivary alterations in patients with type 2 diabetes: a systematic review and meta‐analysis. J Dent. 2024;150:105321. [DOI] [PubMed] [Google Scholar]
- 51. Weijdijk LPM, Van der Weijden GA, Slot DE. DMF scores in patients with diabetes mellitus: a systematic review and meta‐analysis of observational studies. J Dent. 2023;136:104628. [DOI] [PubMed] [Google Scholar]
- 52. Coelho AS, Amaro IF, Caramelo F, et al. Dental caries, diabetes mellitus, metabolic control and diabetes duration: a systematic review and meta‐analysis. J Esthet Restor Dent. 2020;32(3):291‐309. [DOI] [PubMed] [Google Scholar]
- 53. de Lima AKA, Amorim Dos Santos J, Stefani CM, et al. Diabetes mellitus and poor glycemic control increase the occurrence of coronal and root caries: a systematic review and meta‐analysis. Clin Oral Investig. 2020;24(11):3801‐3812. [DOI] [PubMed] [Google Scholar]
- 54. Roy M, Gastaldi G, Courvoisier DS, et al. Periodontal health in a cohort of subjects with type 1 diabetes mellitus. Clin Exp Dent Res. 2019;5(3):243‐249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Gogeneni H, Buduneli N, Ceyhan‐Öztürk B, et al. Increased infection with key periodontal pathogens during gestational diabetes mellitus. J Clin Periodontol. 2015;42(6):506‐512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Chaparro A, Realini O, Hernández M, et al. Early pregnancy levels of gingival crevicular fluid matrix metalloproteinases‐8 and ‐9 are associated with the severity of periodontitis and the development of gestational diabetes mellitus. J Periodontol. 2021;92(2):205‐215. [DOI] [PubMed] [Google Scholar]
- 57. Özçaka Ö, Ceyhan‐Öztürk B, Gümüş P, et al. Clinical periodontal status and inflammatory cytokines in gestational diabetes mellitus. Arch Oral Biol. 2016;72:87‐91. [DOI] [PubMed] [Google Scholar]
- 58. Bunpeng N, Boriboonhirunsarn D, Boriboonhirunsarn C, et al. Association between gestational diabetes mellitus and periodontitis via the effect of reactive oxygen species in peripheral blood cells. J Periodontol. 2022;93(5):758‐769. [DOI] [PubMed] [Google Scholar]
- 59. Chaparro A, Zúñiga E, Varas‐Godoy M, et al. Periodontitis and placental growth factor in oral fluids are early pregnancy predictors of gestational diabetes mellitus. J Periodontol. 2018;89(9):1052‐1060. [DOI] [PubMed] [Google Scholar]
- 60. Liu YK, Chen V, He JZ, et al. A salivary microbiome‐based auxiliary diagnostic model for type 2 diabetes mellitus. Arch Oral Biol. 2021;126:105118. [DOI] [PubMed] [Google Scholar]
- 61. Su N, Teeuw WJ, Loos BG, et al. Development and validation of a screening model for diabetes mellitus in patients with periodontitis in dental settings. Clin Oral Investig. 2020;24(11):4089‐4100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Vo TTT, Lee CW, Chiang YC, et al. Protective mechanisms of Taiwanese green propolis toward high glucose‐induced inflammation via NLRP3 inflammasome signaling pathway in human gingival fibroblasts. J Periodontal Res. 2021;56(4):804‐818. [DOI] [PubMed] [Google Scholar]
- 63. Passoja A, Knuuttila M, Hiltunen L, et al. Serum interleukin‐6 may modulate periodontal inflammation in type 1 diabetic subjects. J Clin Periodontol. 2011;38(8):687‐693. [DOI] [PubMed] [Google Scholar]
- 64. Matsuda Y, Kato T, Takahashi N, et al. Ligature‐induced periodontitis in mice induces elevated levels of circulating interleukin‐6 but shows only weak effects on adipose and liver tissues. J Periodontal Res. 2016;51(5):639‐646. [DOI] [PubMed] [Google Scholar]
- 65. Purnamasari D, Khumaedi AI, Soeroso Y, et al. The influence of diabetes and or periodontitis on inflammation and adiponectin level. Diabetes Metab Syndr. 2019;13(3):2176‐2182. [DOI] [PubMed] [Google Scholar]
- 66. Liu Y, Zhang Q. Periodontitis aggravated pancreatic β‐cell dysfunction in diabetic mice through interleukin‐12 regulation on Klotho. J Diabetes Investig. 2016;7(3):303‐311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Xiao E, Mattos M, Vieira GHA, et al. Diabetes enhances IL‐17 expression and alters the oral microbiome to increase its pathogenicity. Cell Host Microbe. 2017;22(1):120‐128.e124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Cintra LT, Samuel RO, Azuma MM, et al. Apical periodontitis and periodontal disease increase serum IL‐17 levels in normoglycemic and diabetic rats. Clin Oral Investig. 2014;18(9):2123‐2128. [DOI] [PubMed] [Google Scholar]
- 69. Ferreira RC, Simons HZ, Thompson WS, et al. IL‐21 production by CD4+ effector T cells and frequency of circulating follicular helper T cells are increased in type 1 diabetes patients. Diabetologia. 2015;58(4):781‐790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Singhal S, Pradeep AR, Kanoriya D, et al. Human soluble receptor for advanced glycation end products and tumor necrosis factor‐α as gingival crevicular fluid and serum markers of inflammation in chronic periodontitis and type 2 diabetes. J Oral Sci. 2016;58(4):547‐553. [DOI] [PubMed] [Google Scholar]
- 71. Türer ÇC, Durmuş D, Balli U, et al. Effect of non‐surgical periodontal treatment on gingival crevicular fluid and serum endocan, vascular endothelial growth factor‐A, and tumor necrosis factor‐alpha levels. J Periodontol. 2017;88(5):493‐501. [DOI] [PubMed] [Google Scholar]
- 72. Kim JH, Lee DE, Woo GH, et al. Osteocytic sclerostin expression in alveolar bone in rats with diabetes mellitus and ligature‐induced periodontitis. J Periodontol. 2015;86(8):1005‐1011. [DOI] [PubMed] [Google Scholar]
- 73. Huang Y, Guo W, Zeng J, et al. Prediabetes enhances periodontal inflammation consistent with activation of toll‐like receptor‐mediated nuclear factor‐κB pathway in rats. J Periodontol. 2016;87(5):e64‐e74. [DOI] [PubMed] [Google Scholar]
- 74. Santamaria‐Jr M, Bagne L, Zaniboni E, et al. Diabetes mellitus and periodontitis: inflammatory response in orthodontic tooth movement. Orthod Craniofac Res. 2020;23(1):27‐34. [DOI] [PubMed] [Google Scholar]
- 75. Grauballe MB, Østergaard JA, Schou S, et al. Effects of TNF‐α blocking on experimental periodontitis and type 2 diabetes in obese diabetic Zucker rats. J Clin Periodontol. 2015;42(9):807‐816. [DOI] [PubMed] [Google Scholar]
- 76. Fang H, Yang K, Tang P, et al. Glycosylation end products mediate damage and apoptosis of periodontal ligament stem cells induced by the JNK‐mitochondrial pathway. Aging. 2020;12(13):12850‐12868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Abdella NA, Mojiminiyi OA. Clinical applications of adiponectin measurements in type 2 diabetes mellitus: screening, diagnosis, and marker of diabetes control. Dis Markers. 2018;2018:5187940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Qiu W, Wang Z, Chen Z, et al. The adiponectin receptor agonist AdipoAI attenuates periodontitis in diabetic rats by inhibiting gingival fibroblast‐induced macrophage migration. Br J Pharmacol. 2023;180(18):2436‐2451. [DOI] [PubMed] [Google Scholar]
- 79. Wu Y, Chen L, Wei B, et al. Effect of non‐surgical periodontal treatment on visfatin concentrations in serum and gingival crevicular fluid of patients with chronic periodontitis and type 2 diabetes mellitus. J Periodontol. 2015;86(6):795‐800. [DOI] [PubMed] [Google Scholar]
- 80. An Y, Zhang H, Wang C, et al. Activation of ROS/MAPKs/NF‐κB/NLRP3 and inhibition of efferocytosis in osteoclast‐mediated diabetic osteoporosis. Faseb J. 2019;33(11):12515‐12527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Zheng J, Chen S, Albiero ML, et al. Diabetes activates periodontal ligament fibroblasts via NF‐κB in vivo. J Dent Res. 2018;97(5):580‐588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Li X, Sun X, Zhang X, et al. Enhanced oxidative damage and Nrf2 downregulation contribute to the aggravation of periodontitis by diabetes mellitus. Oxid Med Cell Longev. 2018;2018:9421019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Bastos MF, Tucci MA, de Siqueira A, et al. Diabetes may affect the expression of matrix metalloproteinases and their inhibitors more than smoking in chronic periodontitis. J Periodontal Res. 2017;52(2):292‐299. [DOI] [PubMed] [Google Scholar]
- 84. Torrungruang K, Ongphiphadhanakul B, Jitpakdeebordin S, et al. Mediation analysis of systemic inflammation on the association between periodontitis and glycaemic status. J Clin Periodontol. 2018;45(5):548‐556. [DOI] [PubMed] [Google Scholar]
- 85. Zhou M, Xu X, Li J, et al. C‐reactive protein perturbs alveolar bone homeostasis: an experimental study of periodontitis and diabetes in the rat. J Clin Periodontol. 2022;49(10):1052‐1066. [DOI] [PubMed] [Google Scholar]
- 86. Yilmaz D, Caglayan F, Buber E, et al. Gingival crevicular fluid levels of human beta‐defensin‐1 in type 2 diabetes mellitus and periodontitis. Clin Oral Investig. 2018;22(5):2135‐2140. [DOI] [PubMed] [Google Scholar]
- 87. Yilmaz D, Yilmaz N, Polat R, et al. Salivary levels of hBDs in children and adolescents with type 1 diabetes mellitus and gingivitis. Clin Oral Investig. 2022;26(7):4897‐4904. [DOI] [PubMed] [Google Scholar]
- 88. Wang Q, Nie L, Zhao P, et al. Diabetes fuels periodontal lesions via GLUT1‐driven macrophage inflammaging. Int J Oral Sci. 2021;13(1):11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Akram Z, Alqahtani F, Alqahtani M, et al. Levels of advanced glycation end products in gingival crevicular fluid of chronic periodontitis patients with and without type‐2 diabetes mellitus. J Periodontol. 2020;91(3):396‐402. [DOI] [PubMed] [Google Scholar]
- 90. Mei YM, Li L, Wang XQ, et al. AGEs induces apoptosis and autophagy via reactive oxygen species in human periodontal ligament cells. J Cell Biochem. 2020;121(8–9):3764‐3779. [DOI] [PubMed] [Google Scholar]
- 91. Chiu HC, Fu MM, Yang TS, et al. Effect of high glucose, Porphyromonas gingivalis lipopolysaccharide and advanced glycation end‐products on production of interleukin‐6/‐8 by gingival fibroblasts. J Periodontal Res. 2017;52(2):268‐276. [DOI] [PubMed] [Google Scholar]
- 92. Hiroshima Y, Sakamoto E, Yoshida K, et al. Advanced glycation end‐products and Porphyromonas gingivalis lipopolysaccharide increase calprotectin expression in human gingival epithelial cells. J Cell Biochem. 2018;119(2):1591‐1603. [DOI] [PubMed] [Google Scholar]
- 93. Yi X, Zhang L, Lu W, et al. The effect of NLRP inflammasome on the regulation of AGEs‐induced inflammatory response in human periodontal ligament cells. J Periodontal Res. 2019;54(6):681‐689. [DOI] [PubMed] [Google Scholar]
- 94. Pink C, Kocher T, Meisel P, et al. Longitudinal effects of systemic inflammation markers on periodontitis. J Clin Periodontol. 2015;42(11):988‐997. [DOI] [PubMed] [Google Scholar]
- 95. Fine N, Chadwick JW, Sun C, et al. Periodontal inflammation primes the systemic innate immune response. J Dent Res. 2021;100(3):318‐325. [DOI] [PubMed] [Google Scholar]
- 96. Graves DT, Alshabab A, Albiero ML, et al. Osteocytes play an important role in experimental periodontitis in healthy and diabetic mice through expression of RANKL. J Clin Periodontol. 2018;45(3):285‐292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97. Demmer RT, Breskin A, Rosenbaum M, et al. The subgingival microbiome, systemic inflammation and insulin resistance: the oral infections, glucose intolerance and insulin resistance study. J Clin Periodontol. 2017;44(3):255‐265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Matsha TE, Prince Y, Davids S, et al. Oral microbiome signatures in diabetes mellitus and periodontal disease. J Dent Res. 2020;99(6):658‐665. [DOI] [PubMed] [Google Scholar]
- 99. Shi B, Lux R, Klokkevold P, et al. The subgingival microbiome associated with periodontitis in type 2 diabetes mellitus. Isme J. 2020;14(2):519‐530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100. Li L, Bao J, Chang Y, et al. Gut microbiota may mediate the influence of periodontitis on prediabetes. J Dent Res. 2021;100(12):1387‐1396. [DOI] [PubMed] [Google Scholar]
- 101. Radović N, Nikolić Jakoba N, Petrović N, et al. MicroRNA‐146a and microRNA‐155 as novel crevicular fluid biomarkers for periodontitis in non‐diabetic and type 2 diabetic patients. J Clin Periodontol. 2018;45(6):663‐671. [DOI] [PubMed] [Google Scholar]
- 102. Byun JS, Lee HY, Tian J, et al. Effect of salivary exosomal miR‐25‐3p on periodontitis with insulin resistance. Front Immunol. 2021;12:775046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103. Li B, Xin Z, Gao S, et al. SIRT6‐regulated macrophage efferocytosis epigenetically controls inflammation resolution of diabetic periodontitis. Theranostics. 2023;13(1):231‐249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104. Wu Y, Song LT, Li JS, et al. MicroRNA‐126 regulates inflammatory cytokine secretion in human gingival fibroblasts under high glucose via targeting tumor necrosis factor receptor associated factor 6. J Periodontol. 2017;88(11):e179‐e187. [DOI] [PubMed] [Google Scholar]
- 105. Ou L, Sun T, Cheng Y, et al. MicroRNA‐214 contributes to regulation of necroptosis via targeting ATF4 in diabetes‐associated periodontitis. J Cell Biochem. 2019;120(9):14791‐14803. [DOI] [PubMed] [Google Scholar]
- 106. He L, Liu C, Liu Y, et al. Circular RNA hsa_circ_0084054 promotes the progression of periodontitis with diabetes via the miR‐508‐3p/PTEN axis. J Periodontal Res. 2023;58(4):827‐840. [DOI] [PubMed] [Google Scholar]
- 107. Cirelli T, Nepomuceno R, Rios ACS, et al. Genetic polymorphisms in the Interleukins IL1B, IL4, and IL6 are associated with concomitant periodontitis and type 2 diabetes mellitus in Brazilian patients. J Periodontal Res. 2020;55(6):918‐930. [DOI] [PubMed] [Google Scholar]
- 108. Zhang P, Zhang W, Zhang D, et al. 25‐Hydroxyvitamin D(3) ‐enhanced PTPN2 positively regulates periodontal inflammation through the JAK/STAT pathway in human oral keratinocytes and a mouse model of type 2 diabetes mellitus. J Periodontal Res. 2018;53(3):467‐477. [DOI] [PubMed] [Google Scholar]
- 109. von Wilmowsky C, Stockmann P, Harsch I, et al. Diabetes mellitus negatively affects peri‐implant bone formation in the diabetic domestic pig. J Clin Periodontol. 2011;38(8):771‐779. [DOI] [PubMed] [Google Scholar]
- 110. Tang D, Wang E, Xu Y, et al. Is hyperglycemia the only risk factor for implant in type 2 diabetics during the healing period? Oral Dis. 2021;27(6):1551‐1563. [DOI] [PubMed] [Google Scholar]
- 111. Liu J, Wu Z, He H, et al. Gallium and silicon synergistically promote osseointegration of dental implant in patients with osteoporosis. Med Hypotheses. 2017;103:35‐38. [DOI] [PubMed] [Google Scholar]
- 112. Daubert DM, Weinstein BF, Bordin S, et al. Prevalence and predictive factors for peri‐implant disease and implant failure: a cross‐sectional analysis. J Periodontol. 2015;86(3):337‐347. [DOI] [PubMed] [Google Scholar]
- 113. Aguilar‐Salvatierra A, Calvo‐Guirado JL, González‐Jaranay M, et al. Peri‐implant evaluation of immediately loaded implants placed in esthetic zone in patients with diabetes mellitus type 2: a two‐year study. Clin Oral Implants Res. 2016;27(2):156‐161. [DOI] [PubMed] [Google Scholar]
- 114. Al Amri MD, Abduljabbar TS. Comparison of clinical and radiographic status of platform‐switched implants placed in patients with and without type 2 diabetes mellitus: a 24‐month follow‐up longitudinal study. Clin Oral Implants Res. 2017;28(2):226‐230. [DOI] [PubMed] [Google Scholar]
- 115. Dŏgan ŞB, Kurtiş MB, Tüter G, et al. Evaluation of clinical parameters and levels of proinflammatory cytokines in the crevicular fluid around dental implants in patients with type 2 diabetes mellitus. Int J Oral Maxillofac Implants. 2015;30(5):1119‐1127. [DOI] [PubMed] [Google Scholar]
- 116. Eskow CC, Oates TW. Dental implant survival and complication rate over 2 years for individuals with poorly controlled type 2 diabetes mellitus. Clin Implant Dent Relat Res. 2017;19(3):423‐431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117. Abduljabbar T, Javed F, Malignaggi VR, et al. Influence of implant location in patients with and without type 2 diabetes mellitus: 2‐year follow‐up. Int J Oral Maxillofac Surg. 2017;46(9):1188‐1192. [DOI] [PubMed] [Google Scholar]
- 118. Al Amri MD, Abduljabbar TS, Al‐Johany SS, et al. Comparison of clinical and radiographic parameters around short (6 to 8 mm in length) and long (11 mm in length) dental implants placed in patients with and without type 2 diabetes mellitus: 3‐year follow‐up results. Clin Oral Implants Res. 2017;28(10):1182‐1187. [DOI] [PubMed] [Google Scholar]
- 119. Oliveira LM, Zanatta FB, Antoniazzi RP, et al. Does diabetes mellitus affect guided bone regeneration outcomes in individuals undergoing dental implants? A systematic review and meta‐analysis. Front Dent Med. 2024;5. [Google Scholar]
- 120. Jiang X, Zhu Y, Liu Z, et al. Association between diabetes and dental implant complications: a systematic review and meta‐analysis. Acta Odontol Scand. 2021;79(1):9‐18. [DOI] [PubMed] [Google Scholar]
- 121. Retzepi M, Donos N. The effect of diabetes mellitus on osseous healing. Clin Oral Implants Res. 2010;21(7):673‐681. [DOI] [PubMed] [Google Scholar]
- 122. de Oliveira P, Bonfante EA, Bergamo ETP, et al. Obesity/metabolic syndrome and diabetes mellitus on peri‐implantitis. Trends Endocrinol Metab. 2020;31(8):596‐610. [DOI] [PubMed] [Google Scholar]
- 123. Hu X‐F, Wang L, Xiang G, et al. Angiogenesis impairment by the NADPH oxidase‐triggered oxidative stress at the bone‐implant interface: critical mechanisms and therapeutic targets for implant failure under hyperglycemic conditions in diabetes. Acta Biomater. 2018;73:470‐487. [DOI] [PubMed] [Google Scholar]
- 124. Zafar MS, Fareed MA, Riaz S, et al. Customized therapeutic surface coatings for dental implants. Coatings. 2020;10(6):568. [Google Scholar]
- 125. Yadav R, Agrawal KK, Rao J, et al. Crestal bone loss under delayed loading of full thickness versus flapless surgically placed dental implants in controlled type 2 diabetic patients: a parallel group randomized clinical trial. J Prosthodont. 2018;27(7):611‐617. [DOI] [PubMed] [Google Scholar]
- 126. Sánchez‐Domínguez B, López‐López J, Jané‐Salas E, et al. Glycated hemoglobin levels and prevalence of apical periodontitis in type 2 diabetic patients. J Endod. 2015;41(5):601‐606. [DOI] [PubMed] [Google Scholar]
- 127. Smadi L. Apical periodontitis and endodontic treatment in patients with type II diabetes mellitus: comparative cross‐sectional survey. J Contemp Dent Pract. 2017;18(5):358‐362. [DOI] [PubMed] [Google Scholar]
- 128. Yip N, Liu C, Wu D, et al. The association of apical periodontitis and type 2 diabetes mellitus: a large hospital network cross‐sectional case‐controlled study. J Am Dent Assoc. 2021;152(6):434‐443. [DOI] [PubMed] [Google Scholar]
- 129. Limeira FIR, Arantes DC, de Souza Oliveira C, et al. Root canal treatment and apical periodontitis in a Brazilian population with type 1 diabetes mellitus: a cross‐sectional paired study. J Endod. 2020;46(6):756‐762. [DOI] [PubMed] [Google Scholar]
- 130. Davidović B, Krunić J, Mladenović I, et al. Effects of apical periodontitis treatment on hyperglycaemia in diabetes: a prospective cohort study. Int Endod J. 2024;57(8):1099‐1109. [DOI] [PubMed] [Google Scholar]
- 131. Wang S, Wang X, Bai F, et al. Effect of endodontic treatment on clinical outcome in type 2 diabetic patients with apical periodontitis. Heliyon. 2023;9(3):e13914. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 132. Arya S, Duhan J, Tewari S, et al. Healing of apical periodontitis after nonsurgical treatment in patients with type 2 diabetes. J Endod. 2017;43(10):1623‐1627. [DOI] [PubMed] [Google Scholar]
- 133. Prasetyo EP, Sampoerno G, Juniarti DE, et al. Effect of lipopolysaccharide‐induced apical periodontitis in diabetes mellitus rats on periapical inflammation. Eur J Dent. 2023;17(4):1146‐1152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134. Prieto AKC, Gomes‐Filho JE, Azuma MM, et al. Influence of apical periodontitis on stress oxidative parameters in diabetic rats. J Endod. 2017;43(10):1651‐1656. [DOI] [PubMed] [Google Scholar]
- 135. De la Torre‐Luna R, Domínguez‐Pérez RA, Guillén‐Nepita AL, et al. Prevalence of Candida albicans in primary endodontic infections associated with a higher frequency of apical periodontitis in type two diabetes mellitus patients. Eur J Clin Microbiol Infect Dis. 2020;39(1):131‐138. [DOI] [PubMed] [Google Scholar]
- 136. Gadicherla S, Smriti K, Roy S, et al. Comparison of extraction socket healing in non‐diabetic, prediabetic, and type 2 diabetic patients. Clin Cosmet Investig Dent. 2020;12:291‐296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137. Power DJ, Sambrook PJ, Goss AN. The healing of dental extraction sockets in insulin‐dependent diabetic patients: a prospective controlled observational study. Aust Dent J. 2019;64(1):111‐116. [DOI] [PubMed] [Google Scholar]
- 138. Fernandes KS, Glick M, de Souza MS, et al. Association between immunologic parameters, glycemic control, and postextraction complications in patients with type 2 diabetes. J Am Dent Assoc. 2015;146(8):592‐599. [DOI] [PubMed] [Google Scholar]
- 139. Yang S, Li Y, Liu C, et al. Pathogenesis and treatment of wound healing in patients with diabetes after tooth extraction. Front Endocrinol. 2022;13:949535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140. Gazal G. Management of an emergency tooth extraction in diabetic patients on the dental chair. Saudi Dent J. 2020;32(1):1‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141. Sykara M, Maniatakos P, Tentolouris A, et al. The necessity of administrating antibiotic prophylaxis to patients with diabetes mellitus prior to oral surgical procedures—a systematic review. Diabetes Metab Syndr. 2022;16(10):102621. [DOI] [PubMed] [Google Scholar]
- 142. Zhang S, Song S, Wang S, et al. Type 2 diabetes affects postextraction socket healing and influences first‐stage implant surgery: a study based on clinical and animal evidence. Clin Implant Dent Relat Res. 2019;21(3):436‐445. [DOI] [PubMed] [Google Scholar]
- 143. Maftei G‐A, Martu M‐A, Martu M‐C, et al. Correlations between salivary immuno‐biochemical markers and HbA1c in type 2 diabetes subjects before and after dental extraction. Antioxidants. 2021;10(11):1741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144. Al Shehhi YI, Elemam NM, Alsaegh MA. The response of salivary proinflammatory biomarkers to tooth extraction in individuals with type II diabetes mellitus. BMC Oral Health. 2024;24(1):250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145. Daraei P, Moore CE. Racial disparity among the head and neck cancer population. J Cancer Educ. 2015;30(3):546‐551. [DOI] [PubMed] [Google Scholar]
- 146. Liu S, Zhao Q, Zheng Z, et al. Status of treatment and prophylaxis for radiation‐induced oral mucositis in patients with head and neck cancer. Front Oncol. 2021;11:642575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147. Shavi GR, Thakur B, Bhambal A, et al. Oral health related quality of life in patients of head and neck cancer attending cancer hospital of Bhopal city, India. J Int Oral Health. 2015;7(8):21‐27. [PMC free article] [PubMed] [Google Scholar]
- 148. Ederaine SA, Dominguez JL, Harvey JA, et al. Survival and glycemic control in patients with co‐existing squamous cell carcinoma and diabetes mellitus. Future Sci OA. 2021;7(5):Fso683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149. Hu X, Wu J, Xiong H, et al. Type 2 diabetes mellitus promotes the proliferation, metastasis, and suppresses the apoptosis in oral squamous cell carcinoma. J Oral Pathol Med. 2022;51(5):483‐492. [DOI] [PubMed] [Google Scholar]
- 150. Xu W, Chen Z, Zhang L. Impact of diabetes on the prognosis of patients with oral and oropharyngeal cancer: a meta‐analysis. J Diabetes Investig. 2024;15(8):1140‐1150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151. Tseng CH. Pioglitazone and oral cancer risk in patients with type 2 diabetes. Oral Oncol. 2014;50(2):98‐103. [DOI] [PubMed] [Google Scholar]
- 152. Sung HL, Hung CY, Tung YC, et al. Comparison between sodium‐glucose cotransporter 2 inhibitors and dipeptidyl peptidase 4 inhibitors on the risk of incident cancer in patients with diabetes mellitus: a real‐world evidence study. Diabetes Metab Res Rev. 2024;40(3):e3784. [DOI] [PubMed] [Google Scholar]
- 153. Hu WS, Lin CL. Patients with diabetes with and without sodium‐glucose cotransporter‐2 inhibitors use with incident cancer risk. J Diabetes Complic. 2023;37(5):108468. [DOI] [PubMed] [Google Scholar]
- 154. Koepsell H. The Na(+)‐D‐glucose cotransporters SGLT1 and SGLT2 are targets for the treatment of diabetes and cancer. Pharmacol Ther. 2017;170:148‐165. [DOI] [PubMed] [Google Scholar]
- 155. Gier B, Matveyenko AV, Kirakossian D, et al. Chronic GLP‐1 receptor activation by exendin‐4 induces expansion of pancreatic duct glands in rats and accelerates formation of dysplastic lesions and chronic pancreatitis in the Kras(G12D) mouse model. Diabetes. 2012;61(5):1250‐1262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156. Bjerre Knudsen L, Madsen LW, Andersen S, et al. Glucagon‐like Peptide‐1 receptor agonists activate rodent thyroid C‐cells causing calcitonin release and C‐cell proliferation. Endocrinology. 2010;151(4):1473‐1486. [DOI] [PubMed] [Google Scholar]
- 157. Cao C, Yang S, Zhou Z. GLP‐1 receptor agonists and risk of cancer in type 2 diabetes: an updated meta‐analysis of randomized controlled trials. Endocrine. 2019;66(2):157‐165. [DOI] [PubMed] [Google Scholar]
- 158. Liu Y, Zhang X, Chai S, et al. Risk of malignant neoplasia with glucagon‐like peptide‐1 receptor agonist treatment in patients with type 2 diabetes: a meta‐analysis. J Diabetes Res. 2019;2019:1534365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159. Gallagher EJ, LeRoith D. Diabetes, cancer, and metformin: connections of metabolism and cell proliferation. Ann N Y Acad Sci. 2011;1243:54‐68. [DOI] [PubMed] [Google Scholar]
- 160. Rohani B. Oral manifestations in patients with diabetes mellitus. World J Diabetes. 2019;10(9):485‐489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161. Lima DLF, Carneiro S, Barbosa FTS, et al. Salivary flow and xerostomia in older patients with type 2 diabetes mellitus. PLoS One. 2017;12(8):e0180891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162. Hoseini A, Mirzapour A, Bijani A, et al. Salivary flow rate and xerostomia in patients with type I and II diabetes mellitus. Electron Phys. 2017;9(9):5244‐5249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163. Visvanathan V, Nix P. Managing the patient presenting with xerostomia: a review. Int J Clin Pract. 2010;64(3):404‐407. [DOI] [PubMed] [Google Scholar]
- 164. Stewart CR, Obi N, Epane EC, et al. Effects of diabetes on salivary gland protein expression of tetrahydrobiopterin and nitric oxide synthesis and function. J Periodontol. 2016;87(6):735‐741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165. Chen SY, Wang Y, Zhang CL, et al. Decreased basal and stimulated salivary parameters by histopathological lesions and secretory dysfunction of parotid and submandibular glands in rats with type 2 diabetes. Exp Ther Med. 2020;19(4):2707‐2719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166. Monteiro MM, D'Epiro TT, Bernardi L, et al. Long‐ and short‐term diabetes mellitus type 1 modify young and elder rat salivary glands morphology. Arch Oral Biol. 2017;73:40‐47. [DOI] [PubMed] [Google Scholar]
- 167. Huang Y, Mao QY, Shi XJ, et al. Disruption of tight junctions contributes to hyposalivation of salivary glands in a mouse model of type 2 diabetes. J Anat. 2020;237(3):556‐567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168. Sato T, Mito K, Ishii H. Relationship between impaired parasympathetic vasodilation and hyposalivation in parotid glands associated with type 2 diabetes mellitus. Am J Physiol Regul Integr Comp Physiol. 2020;318(5):R940‐R949. [DOI] [PubMed] [Google Scholar]
- 169. Wu CB, Xue L, Zhou Q. Treatment strategy for chronic obstructive parotitis related to diabetes: a retrospective analysis of 12 cases. Front Pharmacol. 2022;13:869872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170. Muhamed SA, Moussa EM, Aboasy NK, et al. Effect of 1% malic acid spray on diabetes mellitus‐induced xerostomia: a randomized clinical trial. Oral Dis. 2024;30(2):631‐638. [DOI] [PubMed] [Google Scholar]
- 171. Zhang S, Li J, Nong X, et al. Artesunate combined with metformin ameliorate on diabetes‐induced xerostomia by mitigating superior salivatory nucleus and salivary glands injury in type 2 diabetic rats via the PI3K/AKT pathway. Front Pharmacol. 2021;12:774674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172. Shiferaw A, Alem G, Tsehay M, et al. Dental caries and associated factors among diabetic and nondiabetic adult patients attending Bichena Primary Hospital's Outpatient Department. Front Oral Health. 2022;3:938405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 173. Schmolinsky J, Kocher T, Rathmann W, et al. Diabetes status affects long‐term changes in coronal caries—the SHIP study. Sci Rep. 2019;9(1):15685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 174. Wang Y, Xing L, Yu H, et al. Prevalence of dental caries in children and adolescents with type 1 diabetes: a systematic review and meta‐analysis. BMC Oral Health. 2019;19(1):213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 175. Ferizi L, Dragidella F, Spahiu L, et al. The influence of type 1 diabetes mellitus on dental caries and salivary composition. Int J Dent. 2018;2018:5780916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 176. Latti BR, Kalburge JV, Birajdar SB, et al. Evaluation of relationship between dental caries, diabetes mellitus and oral microbiota in diabetics. J Oral Maxillofac Pathol. 2018;22(2):282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177. PradeepKumar AR, JothiLatha S, Durvasulu A, et al. Impact of type 2 diabetes mellitus on the occurrence of vertical root fracture: a case control study. J Endod. 2024;50(4):450‐455.e451. [DOI] [PubMed] [Google Scholar]
- 178. Saghiri MA, Nath D, Rahmani B, et al. The effect of diabetes on fracture resistance of teeth: an in vitro study. Aust Endod J. 2021;47(3):499‐505. [DOI] [PubMed] [Google Scholar]
- 179. Abbassy MA, Watari I, Bakry AS, et al. Diabetes detrimental effects on enamel and dentine formation. J Dent. 2015;43(5):589‐596. [DOI] [PubMed] [Google Scholar]
- 180. Saghiri MA, Vakhnovetsky J, Samadi E, et al. Effects of diabetes on elemental levels and nanostructure of root canal dentin. J Endod. 2023;49(9):1169‐1175. [DOI] [PubMed] [Google Scholar]
- 181. Cosgarea R, Tristiu R, Dumitru RB, et al. Effects of non‐surgical periodontal therapy on periodontal laboratory and clinical data as well as on disease activity in patients with rheumatoid arthritis. Clin Oral Investig. 2019;23(1):141‐151. [DOI] [PubMed] [Google Scholar]
- 182. Juan CY, Hsu CW, Lu MC. Increased dental visits in patients with rheumatoid arthritis: a secondary cohort analysis of population based claims data. BMC Oral Health. 2022;22(1):609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 183. Mühlberg S, Jäger J, Krohn‐Grimberghe B, et al. Oral health‐related quality of life depending on oral health in patients with rheumatoid arthritis. Clin Oral Investig. 2017;21(9):2661‐2670. [DOI] [PubMed] [Google Scholar]
- 184. Manzano BR, da Silva Santos PS, Bariquelo MH, et al. A case‐control study of oral diseases and quality of life in individuals with rheumatoid arthritis and systemic lupus erythematosus. Clin Oral Investig. 2021;25(4):2081‐2092. [DOI] [PubMed] [Google Scholar]
- 185. González‐Febles J, Rodríguez‐Lozano B, Sánchez‐Piedra C, et al. Association between periodontitis and anti‐citrullinated protein antibodies in rheumatoid arthritis patients: a cross‐sectional study. Arthritis Res Ther. 2020;22(1):27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 186. Oliveira SR, de Arruda JAA, Schneider AH, et al. Are neutrophil extracellular traps the link for the cross‐talk between periodontitis and rheumatoid arthritis physiopathology? Rheumatology (Oxford). 2021;61(1):174‐184. [DOI] [PubMed] [Google Scholar]
- 187. Inanc N, Mumcu G, Can M, et al. Elevated serum TREM‐1 is associated with periodontitis and disease activity in rheumatoid arthritis. Sci Rep. 2021;11(1):2888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 188. Yilmaz D, Gönüllü E, Gürsoy M, et al. Salivary and serum concentrations of monocyte chemoattractant protein‐1, macrophage inhibitory factor, and fractalkine in relation to rheumatoid arthritis and periodontitis. J Periodontol. 2021;92(9):1295‐1305. [DOI] [PubMed] [Google Scholar]
- 189. Schulz S, Zimmer P, Pütz N, et al. rs2476601 in PTPN22 gene in rheumatoid arthritis and periodontitis‐a possible interface? J Transl Med. 2020;18(1):389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 190. Svärd A, Renvert S, Sanmartin Berglund J, et al. Antibodies to citrullinated peptides in serum and saliva in patients with rheumatoid arthritis and their association to periodontitis. Clin Exp Rheumatol. 2020;38(4):699‐704. [PubMed] [Google Scholar]
- 191. Kaneko C, Kobayashi T, Ito S, et al. Association among periodontitis severity, anti‐agalactosyl immunoglobulin G titer, and the disease activity of rheumatoid arthritis. J Periodontal Res. 2021;56(4):702‐709. [DOI] [PubMed] [Google Scholar]
- 192. Reichert S, Jurianz E, Natalie P, et al. Is periodontitis a prognostic factor in order to indicate antibodies against citrullinated peptides in patients with rheumatoid arthritis? Clin Exp Rheumatol. 2020;38(2):227‐238. [PubMed] [Google Scholar]
- 193. Massarenti L, Enevold C, Damgaard D, et al. Peptidylarginine deiminase 2 gene polymorphisms in subjects with periodontitis predispose to rheumatoid arthritis. Int J Mol Sci. 2022;23(17):9536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194. Lee JA, Mikuls TR, Sayles HR, et al. Associations between periodontitis and serum anti‐malondialdehyde‐acetaldehyde antibody concentrations in rheumatoid arthritis: a case‐control study. J Periodontol. 2024;95:929‐941. [DOI] [PubMed] [Google Scholar]
- 195. El‐Wakeel NM, Shalaby ZF, Abdulmaguid RF, et al. Local gingival crevicular fluid, synovial fluid, and circulating levels of prolactin hormone in patients with moderately active rheumatoid arthritis and stage III and IV periodontitis before and after non‐surgical periodontal treatment—a controlled trial. Clin Oral Investig. 2023;27(6):2813‐2821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 196. Li RN, Ou TT, Lin CH, et al. NLRP3 gene polymorphisms in rheumatoid arthritis and primary Sjogren's syndrome patients. Diagnostics. 2023;13(2):206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 197. Jung ES, Choi YY, Lee KH. Relationship between rheumatoid arthritis and periodontal disease in Korean adults: data from the Sixth Korea National Health and Nutrition Examination Survey, 2013 to 2015. J Periodontol. 2019;90(4):350‐357. [DOI] [PubMed] [Google Scholar]
- 198. Lee KH, Choi YY. Rheumatoid arthritis and periodontitis in adults: using the Korean National Health Insurance Service‐National Sample Cohort. J Periodontol. 2020;91(9):1186‐1193. [DOI] [PubMed] [Google Scholar]
- 199. Karapetsa D, Consensi A, Castagnoli G, et al. Periodontitis in Italian patients with established rheumatoid arthritis: a cross‐sectional study. Oral Dis. 2022;28(6):1715‐1722. [DOI] [PubMed] [Google Scholar]
- 200. Bolstad AI, Fevang BS, Lie SA. Increased risk of periodontitis in patients with rheumatoid arthritis: a nationwide register study in Norway. J Clin Periodontol. 2023;50(8):1022‐1032. [DOI] [PubMed] [Google Scholar]
- 201. Ziebolz D, Rupprecht A, Schmickler J, et al. Association of different immunosuppressive medications with periodontal condition in patients with rheumatoid arthritis: results from a cross‐sectional study. J Periodontol. 2018;89(11):1310‐1317. [DOI] [PubMed] [Google Scholar]
- 202. Coat J, Demoersman J, Beuzit S, et al. Anti‐B lymphocyte immunotherapy is associated with improvement of periodontal status in subjects with rheumatoid arthritis. J Clin Periodontol. 2015;42(9):817‐823. [DOI] [PubMed] [Google Scholar]
- 203. Moura MF, Cota LOM, Silva TA, et al. Clinical and microbiological effects of non‐surgical periodontal treatment in individuals with rheumatoid arthritis: a controlled clinical trial. Odontology. 2021;109(2):484‐493. [DOI] [PubMed] [Google Scholar]
- 204. Nguyen VB, Nguyen TT, Huynh NC, et al. Effects of non‐surgical periodontal treatment in rheumatoid arthritis patients: a randomized clinical trial. Dent Med Probl. 2021;58(1):97‐105. [DOI] [PubMed] [Google Scholar]
- 205. Schmickler J, Rupprecht A, Patschan S, et al. Cross‐sectional evaluation of periodontal status and microbiologic and rheumatoid parameters in a large cohort of patients with rheumatoid arthritis. J Periodontol. 2017;88(4):368‐379. [DOI] [PubMed] [Google Scholar]
- 206. Manoil D, Bostanci N, Mumcu G, et al. Novel and known periodontal pathogens residing in gingival crevicular fluid are associated with rheumatoid arthritis. J Periodontol. 2021;92(3):359‐370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 207. Lehenaff R, Tamashiro R, Nascimento MM, et al. Subgingival microbiome of deep and shallow periodontal sites in patients with rheumatoid arthritis: a pilot study. BMC Oral Health. 2021;21(1):248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 208. Laugisch O, Wong A, Sroka A, et al. Citrullination in the periodontium—a possible link between periodontitis and rheumatoid arthritis. Clin Oral Investig. 2016;20(4):675‐683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 209. Bello‐Gualtero JM, Lafaurie GI, Hoyos LX, et al. Periodontal disease in individuals with a genetic risk of developing arthritis and early rheumatoid arthritis: a cross‐sectional study. J Periodontol. 2016;87(4):346‐356. [DOI] [PubMed] [Google Scholar]
- 210. Kirchner A, Jäger J, Krohn‐Grimberghe B, et al. Active matrix metalloproteinase‐8 and periodontal bacteria depending on periodontal status in patients with rheumatoid arthritis. J Periodontal Res. 2017;52(4):745‐754. [DOI] [PubMed] [Google Scholar]
- 211. Kurgan Ş, Fentoğlu Ö, Önder C, et al. The effects of periodontal therapy on gingival crevicular fluid matrix metalloproteinase‐8, interleukin‐6 and prostaglandin E2 levels in patients with rheumatoid arthritis. J Periodontal Res. 2016;51(5):586‐595. [DOI] [PubMed] [Google Scholar]
- 212. Kim D, Lee G, Huh YH, et al. NAMPT is an essential regulator of RA‐mediated periodontal inflammation. J Dent Res. 2017;96(6):703‐711. [DOI] [PubMed] [Google Scholar]
- 213. Pan W, Yin W, Yang L, et al. Inhibition of Ctsk alleviates periodontitis and comorbid rheumatoid arthritis via downregulation of the TLR9 signalling pathway. J Clin Periodontol. 2019;46(3):286‐296. [DOI] [PubMed] [Google Scholar]
- 214. Domínguez‐Pérez RA, Loyola‐Rodriguez JP, Abud‐Mendoza C, et al. Association of cytokines polymorphisms with chronic peridontitis and rheumatoid arthritis in a Mexican population. Acta Odontol Scand. 2017;75(4):243‐248. [DOI] [PubMed] [Google Scholar]
- 215. Loutan L, Alpizar‐Rodriguez D, Courvoisier DS, et al. Periodontal status correlates with anti‐citrullinated protein antibodies in first‐degree relatives of individuals with rheumatoid arthritis. J Clin Periodontol. 2019;46(7):690‐698. [DOI] [PubMed] [Google Scholar]
- 216. Moccia S, Nucci L, Spagnuolo C, et al. Polyphenols as potential agents in the management of temporomandibular disorders. Appl Sci. 2020;10(15):5305. [Google Scholar]
- 217. Lin CY, Chung CH, Chu HY, et al. Prevalence of temporomandibular disorders in rheumatoid arthritis and associated risk factors: a nationwide study in Taiwan. J Oral Facial Pain Headache. 2017;31(4):e29‐e36. [DOI] [PubMed] [Google Scholar]
- 218. Ahmed N, Petersson A, Catrina AI, et al. Tumor necrosis factor mediates temporomandibular joint bone tissue resorption in rheumatoid arthritis. Acta Odontol Scand. 2015;73(3):232‐240. [DOI] [PubMed] [Google Scholar]
- 219. El Qashty RMN, Mohamed NN, Radwan LRS, et al. Effect of bone marrow mesenchymal stem cells on healing of temporomandibular joints in rats with induced rheumatoid arthritis. Eur J Oral Sci. 2018;126(4):272‐281. [DOI] [PubMed] [Google Scholar]
- 220. Silvestre‐Rangil J, Bagán L, Silvestre FJ, et al. Oral manifestations of rheumatoid arthritis. A cross‐sectional study of 73 patients. Clin Oral Investig. 2016;20(9):2575‐2580. [DOI] [PubMed] [Google Scholar]
- 221. Sorgato CC, Lins ESM, Leão JC, et al. EBV and CMV viral load in rheumatoid arthritis and their role in associated Sjögren's syndrome. J Oral Pathol Med. 2020;49(7):693‐700. [DOI] [PubMed] [Google Scholar]
- 222. Martinez‐Martinez RE, Domínguez‐Pérez RA, Sancho‐Mata J, et al. The frequency and severity of dental caries, and counts of cariogenic bacteria in rheumatoid arthritis patients. Dent Med Probl. 2019;56(2):137‐142. [DOI] [PubMed] [Google Scholar]
- 223. Karataş E, Kul A, Tepecik E. Association between rheumatoid arthritis and apical periodontitis: a cross‐sectional study. Eur Endod J. 2020;5(2):155‐158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 224. Global, regional, and national age‐sex‐specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736‐1788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 225. GBD 2017 DALYs and HALE Collaborators . Global, regional, and national disability‐adjusted life‐years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1859‐1922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 226. Di Cesare M, Perel P, Taylor S, et al. The heart of the world. Glob Heart. 2024;19(1):11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 227. Reynolds HR, Craig RG. Atherosclerotic vascular disease and periodontal disease. In: Craig R, Kamer A, eds. A Clinician's Guide to Systemic Effects of Periodontal Diseases. Springer; 2016:39‐51. [Google Scholar]
- 228. Dietrich T, Webb I, Stenhouse L, et al. Evidence summary: the relationship between oral and cardiovascular disease. Br Dent J. 2017;222(5):381‐385. [DOI] [PubMed] [Google Scholar]
- 229. Gomes‐Filho IS, Coelho JMF, Miranda SS, et al. Severe and moderate periodontitis are associated with acute myocardial infarction. J Periodontol. 2020;91(11):1444‐1452. [DOI] [PubMed] [Google Scholar]
- 230. Cho HJ, Shin MS, Song Y, et al. Severe periodontal disease increases acute myocardial infarction and stroke: a 10‐year retrospective follow‐up study. J Dent Res. 2021;100(7):706‐713. [DOI] [PubMed] [Google Scholar]
- 231. Behle JH, Papapanou PN. Periodontal infections and atherosclerotic vascular disease: an update. Int Dent J. 2006;56(suppl 41):256‐262. [DOI] [PubMed] [Google Scholar]
- 232. Curia MC, Pignatelli P, D'Antonio DL, et al. Oral Porphyromonas gingivalis and Fusobacterium nucleatum abundance in subjects in primary and secondary cardiovascular prevention, with or without heterozygous familial hypercholesterolemia. Biomedicines. 2022;10(9):2144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 233. Wu Y, Wang Y, Du L, et al. The link between different infection forms of Porphyromonas gingivalis and acute myocardial infarction: a cross‐sectional study. BMC Oral Health. 2023;23(1):63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 234. Farrugia C, Stafford GP, Potempa J, et al. Mechanisms of vascular damage by systemic dissemination of the oral pathogen Porphyromonas gingivalis . FEBS J. 2021;288(5):1479‐1495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 235. Gimbrone MA, Jr. , García‐Cardeña G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ Res. 2016;118(4):620‐636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 236. Leishman SJ, Ford PJ, Do HL, et al. Periodontal pathogen load and increased antibody response to heat shock protein 60 in patients with cardiovascular disease. J Clin Periodontol. 2012;39(10):923‐930. [DOI] [PubMed] [Google Scholar]
- 237. Craig RG, Kamer AR. A Clinician's Guide to Systemic Effects of Periodontal Diseases. Springer; 2016. [Google Scholar]
- 238. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens. 2018;36(10):1953‐2041. [DOI] [PubMed] [Google Scholar]
- 239. Wang YR, Alexander GC, Stafford RS. Outpatient hypertension treatment, treatment intensification, and control in Western Europe and the United States. Arch Intern Med. 2007;167(2):141‐147. [DOI] [PubMed] [Google Scholar]
- 240. Cutler JA, Sorlie PD, Wolz M, et al. Trends in hypertension prevalence, awareness, treatment, and control rates in United States adults between 1988–1994 and 1999–2004. Hypertension. 2008;52(5):818‐827. [DOI] [PubMed] [Google Scholar]
- 241. Surma S, Romańczyk M, Witalińska‐Łabuzek J, et al. Periodontitis, blood pressure, and the risk and control of arterial hypertension: epidemiological, clinical, and pathophysiological aspects—review of the literature and clinical trials. Curr Hypertens Rep. 2021;23(5):27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 242. Del Pinto R, Pietropaoli D, Munoz‐Aguilera E, et al. Periodontitis and hypertension: is the association causal? High Blood Press Cardiovasc Prev. 2020;27(4):281‐289. [DOI] [PubMed] [Google Scholar]
- 243. Franek E, Napora M, Blach A, et al. Blood pressure and left ventricular mass in subjects with type 2 diabetes and gingivitis or chronic periodontitis. J Clin Periodontol. 2010;37(10):875‐880. [DOI] [PubMed] [Google Scholar]
- 244. Muñoz Aguilera E, Suvan J, Buti J, et al. Periodontitis is associated with hypertension: a systematic review and meta‐analysis. Cardiovasc Res. 2020;116(1):28‐39. [DOI] [PubMed] [Google Scholar]
- 245. Hwang SY, Oh H, Rhee MY, et al. Association of periodontitis, missing teeth, and oral hygiene behaviors with the incidence of hypertension in middle‐aged and older adults in Korea: a 10‐year follow‐up study. J Periodontol. 2022;93(9):1283‐1293. [DOI] [PubMed] [Google Scholar]
- 246. Rodrigues JVS, Cláudio MM, Franciscon JPS, et al. The effect of non‐surgical periodontal treatment on patients with combined refractory arterial hypertension and stage III, grade B periodontitis: a preliminary prospective clinical study. J Clin Med. 2023;12(13):4277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 247. Lanau N, Mareque‐Bueno J, Zabalza MJ. Impact of nonsurgical periodontal treatment on blood pressure: a prospective cohort study. Eur J Dent. 2024;18(02):517‐525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 248. Ozmeric N, Elgun S, Kalfaoglu D, et al. Interaction between hypertension and periodontitis. Oral Dis. 2024;30(3):1622‐1631. [DOI] [PubMed] [Google Scholar]
- 249. Czesnikiewicz‐Guzik M, Osmenda G, Siedlinski M, et al. Causal association between periodontitis and hypertension: evidence from Mendelian randomization and a randomized controlled trial of non‐surgical periodontal therapy. Eur Heart J. 2019;40(42):3459‐3470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 250. Dutzan N, Kajikawa T, Abusleme L, et al. A dysbiotic microbiome triggers T(H)17 cells to mediate oral mucosal immunopathology in mice and humans. Sci Transl Med. 2018;10(463):eaat0797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 251. Dutzan N, Abusleme L. T helper 17 cells as pathogenic drivers of periodontitis. Adv Exp Med Biol. 2019;1197:107‐117. [DOI] [PubMed] [Google Scholar]
- 252. Gordon JH, LaMonte MJ, Genco RJ, et al. Is the oral microbiome associated with blood pressure in older women? High Blood Press Cardiovasc Prev. 2019;26(3):217‐225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 253. Pietropaoli D, Del Pinto R, Ferri C, et al. Definition of hypertension‐associated oral pathogens in NHANES. J Periodontol. 2019;90(8):866‐876. [DOI] [PubMed] [Google Scholar]
- 254. LaMonte MJ, Gordon JH, Diaz‐Moreno P, et al. Oral microbiome is associated with incident hypertension among postmenopausal women. J Am Heart Assoc. 2022;11(6):e021930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 255. Rodriguez NM, Loren P, Paez I, et al. MicroRNAs: the missing link between hypertension and periodontitis? Int J Mol Sci. 2024;25(4):1992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 256. Ghanbari Z, Moradi Y, Samiee N, et al. Dental caries prevalence in relation to the cardiovascular diseases: cross‐sectional findings from the Iranian Kurdish population. BMC Oral Health. 2024;24(1):509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 257. Wiener RC, Sambamoorthi U. Cross‐sectional association between the number of missing teeth and cardiovascular disease among adults aged 50 or older: BRFSS 2010. Int J Vasc Med. 2014;2014:421567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 258. Liljestrand JM, Havulinna AS, Paju S, et al. Missing teeth predict incident cardiovascular events, diabetes, and death. J Dent Res. 2015;94(8):1055‐1062. [DOI] [PubMed] [Google Scholar]
- 259. Peng J, Song J, Han J, et al. The relationship between tooth loss and mortality from all causes, cardiovascular diseases, and coronary heart disease in the general population: systematic review and dose‐response meta‐analysis of prospective cohort studies. Biosci Rep. 2019;39(1):BSR20181773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 260. Momtazmanesh S, Moghaddam SS, Ghamari S‐H, et al. Global burden of chronic respiratory diseases and risk factors, 1990–2019: an update from the Global Burden of Disease Study 2019. eClinicalMedicine. 2023;59:101936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 261. Dong J, Li W, Wang Q, et al. Relationships between oral microecosystem and respiratory diseases. Front Mol Biosci. 2022;8:718222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 262. Charlson ES, Bittinger K, Haas AR, et al. Topographical continuity of bacterial populations in the healthy human respiratory tract. Am J Respir Crit Care Med. 2011;184(8):957‐963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 263. Gupta A, Saleena LM, Kannan P, et al. The impact of oral diseases on respiratory health and the influence of respiratory infections on the oral microbiome. J Dent. 2024;148:105213. [DOI] [PubMed] [Google Scholar]
- 264. Kim S‐H, Gu S, Kim J‐A, et al. Association between oral health and airflow limitation: analysis using a nationwide survey in Korea. J Korean Med Sci. 2023;38(31):e241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 265. Li S, Ning W, Wang W, et al. Oral health‐related quality of life in patients with chronic respiratory diseases—results of a systematic review. Front Med. 2021;8:757739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 266. Ciardo A, Simon MM, Eberhardt R, et al. Severe chronic obstructive pulmonary disease is associated with reduced oral health conditions. Oral Dis. 2024;30(5):3400‐3412. [DOI] [PubMed] [Google Scholar]
- 267. Hayes C, Sparrow D, Cohen M, et al. The association between alveolar bone loss and pulmonary function: the VA Dental Longitudinal Study. Ann Periodontol. 1998;3(1):257‐261. [DOI] [PubMed] [Google Scholar]
- 268. Scannapieco FA, Ho AW. Potential associations between chronic respiratory disease and periodontal disease: analysis of National Health and Nutrition Examination Survey III. J Periodontol. 2001;72(1):50‐56. [DOI] [PubMed] [Google Scholar]
- 269. Gaeckle NT, Heyman B, Criner AJ, et al. Markers of dental health correlate with daily respiratory symptoms in COPD. Chronic Obstr Pulm Dis. 2018;5(2):97‐105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 270. Zhou X, Han J, Liu Z, et al. Effects of periodontal treatment on lung function and exacerbation frequency in patients with chronic obstructive pulmonary disease and chronic periodontitis: a 2‐year pilot randomized controlled trial. J Clin Periodontol. 2014;41(6):564‐572. [DOI] [PubMed] [Google Scholar]
- 271. Xiong K, Ao K, Wei W, et al. Periodontitis aggravates COPD through the activation of γδ T cell and M2 macrophage. mSystems. 2024;9(2):e00572‐e00523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 272. Li W, Liu W, Yang H, et al. Oral infection with periodontal pathogens induced chronic obstructive pulmonary disease‐like lung changes in mice. BMC Oral Health. 2024;24(1):850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 273. Xiong K, Yang P, Wei W, et al. Periodontitis contributes to COPD progression via affecting ferroptosis. BMC Oral Health. 2023;23(1):664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 274. Bairappan S, Puranik MP, Sowmya KR. Impact of asthma and its medication on salivary characteristics and oral health in adolescents: a cross‐sectional comparative study. Spec Care Dentist. 2020;40(3):227‐237. [DOI] [PubMed] [Google Scholar]
- 275. Moreira LV, Galvão EL, Mourão PS, et al. Association between asthma and oral conditions in children and adolescents: a systematic review with meta‐analysis. Clin Oral Investig. 2023;27(1):45‐67. [DOI] [PubMed] [Google Scholar]
- 276. Jan BM, Khayat MA, Bushnag AI, et al. The association between long‐term corticosteroids use and dental caries: a systematic review. Cureus. 2023;15(9):e44600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 277. Sag C, Ozden FO, Acikgoz G, et al. The effects of combination treatment with a long‐acting beta2‐agonist and a corticosteroid on salivary flow rate, secretory immunoglobulin A, and oral health in children and adolescents with moderate asthma: a 1‐month, single‐blind clinical study. Clin Ther. 2007;29(10):2236‐2242. [DOI] [PubMed] [Google Scholar]
- 278. Lee SW, Lim HJ, Lee E. Association between asthma and periodontitis: results from the Korean National Health and Nutrition Examination Survey. J Periodontol. 2017;88(6):575‐581. [DOI] [PubMed] [Google Scholar]
- 279. Moraschini V, Calasans‐Maia JA, Calasans‐Maia MD. Association between asthma and periodontal disease: a systematic review and meta‐analysis. J Periodontol. 2018;89(4):440‐455. [DOI] [PubMed] [Google Scholar]
- 280. Brasil‐Oliveira R, Cruz ÁA, Souza‐Machado A, et al. Oral health‐related quality of life in individuals with severe asthma. J Bras Pneumol. 2020;47(1):e20200117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 281. Lopes MP, Cruz ÁA, Xavier MT, et al. Prevotella intermedia and periodontitis are associated with severe asthma. J Periodontol. 2020;91(1):46‐54. [DOI] [PubMed] [Google Scholar]
- 282. Hendrix AY, Kheradmand F. The role of matrix metalloproteinases in development, repair, and destruction of the lungs. Prog Mol Biol Transl Sci. 2017;148:1‐29. [DOI] [PubMed] [Google Scholar]
- 283. Gueders MM, Foidart JM, Noel A, et al. Matrix metalloproteinases (MMPs) and tissue inhibitors of MMPs in the respiratory tract: potential implications in asthma and other lung diseases. Eur J Pharmacol. 2006;533(1–3):133‐144. [DOI] [PubMed] [Google Scholar]
- 284. Irie K, Azuma T, Tomofuji T, et al. Exploring the role of IL‐17A in oral dysbiosis‐associated periodontitis and its correlation with systemic inflammatory disease. Dent J. 2023;11(8):194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 285. Son M, Jo S, Lee JS, et al. Association between oral health and incidence of pneumonia: a population‐based cohort study from Korea. Sci Rep. 2020;10(1):9576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 286. Ory J, Mourgues C, Raybaud E, et al. Cost assessment of a new oral care program in the intensive care unit to prevent ventilator‐associated pneumonia. Clin Oral Investig. 2018;22(5):1945‐1951. [DOI] [PubMed] [Google Scholar]
- 287. Prasad R, Daly B, Manley G. The impact of 0.2% chlorhexidine gel on oral health and the incidence of pneumonia amongst adults with profound complex neurodisability. Spec Care Dentist. 2019;39(5):524‐532. [DOI] [PubMed] [Google Scholar]
- 288. Kurasawa Y, Maruoka Y, Sekiya H, et al. Pneumonia prevention effects of perioperative oral management in approximately 25,000 patients following cancer surgery. Clin Exp Dent Res. 2020;6(2):165‐173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 289. Ozaki K, Teranaka S, Tohara H, et al. Oral management by a full‐time resident dentist in the hospital ward reduces the incidence of pneumonia in patients with acute stroke. Int J Dent. 2022;2022:6193818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 290. Iinuma T, Arai Y, Abe Y, et al. Denture wearing during sleep doubles the risk of pneumonia in the very elderly. J Dent Res. 2015;94( suppl3):28s‐36s. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 291. Cao Y, Liu C, Lin J, et al. Oral care measures for preventing nursing home‐acquired pneumonia. Cochrane Database Syst Rev. 2022;11(11):Cd012416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 292. de Melo Neto JP, Melo M, dos Santos‐Pereira SA, et al. Periodontal infections and community‐acquired pneumonia: a case‐control study. Eur J Clin Microbiol Infect Dis. 2013;32(1):27‐32. [DOI] [PubMed] [Google Scholar]
- 293. Kim S‐J, Kim K, Choi S, et al. Chronic periodontitis and community‐acquired pneumonia: a population‐based cohort study. BMC Pulmon Med. 2019;19(1):268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 294. Sumi Y, Miura H, Michiwaki Y, et al. Colonization of dental plaque by respiratory pathogens in dependent elderly. Arch Gerontol Geriatr. 2007;44(2):119‐124. [DOI] [PubMed] [Google Scholar]
- 295. Yamasaki K, Kawanami T, Yatera K, et al. Significance of anaerobes and oral bacteria in community‐acquired pneumonia. PLoS One. 2013;8(5):e63103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 296. Kikutani T, Tamura F, Tashiro H, et al. Relationship between oral bacteria count and pneumonia onset in elderly nursing home residents. Geriatr Gerontol Int. 2015;15(4):417‐421. [DOI] [PubMed] [Google Scholar]
- 297. Nishizawa T, Niikura Y, Akasaka K, et al. Pilot study for risk assessment of aspiration pneumonia based on oral bacteria levels and serum biomarkers. BMC Infect Dis. 2019;19(1):761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 298. Okuda K, Kimizuka R, Abe S, et al. Involvement of periodontopathic anaerobes in aspiration pneumonia. J Periodontol. 2005;76( suppl11):2154‐2160. [DOI] [PubMed] [Google Scholar]
- 299. Tian H, Zhang Z, Wang X, et al. Role of experimental periodontitis in inducing pulmonary inflammation in mice. Oral Dis. 2022;28(8):2294‐2303. [DOI] [PubMed] [Google Scholar]
- 300. Hayashi M, Mori M, Itsumi M, et al. Severity of acute lung injury in aspiration pneumonia model mice transplanted with human oral microflora. Oral Sci Int. 2024;21(1):121‐130. [Google Scholar]
- 301. Darbanian N, Nobahar M, Ghorbani R. Effect of propolis mouthwash on the incidence of ventilator‐associated pneumonia in intensive care unit patients: a comparative randomized triple‐blind clinical trial. BMC Oral Health. 2024;24(1):636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 302. Zhao M, Xie Y, Gao W, et al. Diabetes mellitus promotes susceptibility to periodontitis—novel insight into the molecular mechanisms. Front Endocrinol. 2023;14:1192625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 303. Luong A, Tawfik AN, Islamoglu H, et al. Periodontitis and diabetes mellitus co‐morbidity: a molecular dialogue. J Oral Biosci. 2021;63(4):360‐369. [DOI] [PubMed] [Google Scholar]
- 304. Kunath B, Hickl O, Queirós P, et al. Alterations of oral microbiota and impact on the gut microbiome in type 1 diabetes mellitus revealed by integrated multi‐omic analyses. Microbiome. 2022;10(1):243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 305. Li J, Yuan P, Hu X, et al. A tongue features fusion approach to predicting prediabetes and diabetes with machine learning. J Biomed Inform. 2021;115:103693. [DOI] [PubMed] [Google Scholar]
- 306. Taba M, Grant MM. Editorial: Salivary biomarkers for oral and systemic diseases. Front Dent Med. 2024;5:1429305. [Google Scholar]
- 307. Antony A. Flexible and wearable biosensors: revolutionizing health monitoring. In: Mathew R, Ajayan J, eds. Biosensors: Developments, Challenges and Perspectives. Springer Nature Singapore; 2024:237‐258. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data availability is not applicable to this review as no new data were created or analyzed in this review.