

ABSTRACT
Introduction:
Breast cancer (BC) is considered one of the most commonly diagnosed cancers. Early detection is critical for effective management. This study aims to assess the utility of ultrasonography (US) and mammography (MG) in detecting BC features.
Methods:
This retrospective cross-sectional study involved the electronic records of 263 female patients diagnosed with BC. The mean age was 45.71 ± 12.25 years (17–90 years). A cross-tabulation test was performed to correlate the presence of each malignant feature (Yes/No) on both US and MG and the final ultrasonography diagnosis (benign/malignant). The compatibility between the presence of each feature on both imaging techniques was measured by the percentage of agreement in reporting the feature that was reported as Kappa. The sensitivity and specificity for each feature were calculated, and the receiver operating characteristic curve was used to measure the area under the curve for each feature on both modalities.
Results:
The strong compatibility between the two techniques was 87.1%, 94.29%, 66.92%, 79.85%, 77.56%, 77.18, and 79.84% for irregular shape, uncircumscribed, spiculated margins, tissue distortion, nipple retraction, skin thickening, and the presence of lymphadenopathy, respectively (P < 0.001). Boxplots show that the sensitivity of the US ranged from 37% to 95%, and the specificity ranged from 27% to 91%. However, MG’s sensitivity ranged from 44% to 93%, and the specificity ranged from 36% to 73%.
Conclusion:
US and MG images show similar morphological changes, enhancing diagnostic accuracy in breast lesions. US characterizes echogenicity, provides real-time imaging, and uses color and pulsed Doppler techniques for vascularity and lymphadenopathy detection, while MG is better for identifying different calcification types.
Keywords: Breast cancer, irregular shape of breast lesion, mammography, spiculated margins of breast lesion, ultrasonography
Introduction
Breast cancer (BC) is considered one of the most commonly diagnosed cancers and represents a global health challenge.[1] The World Health Organization (WHO) reports show that 2.3 million women were diagnosed with BC, causing nearly 685,000 female deaths worldwide in 2020.[2] Early detection is critical for BC as it plays a crucial role in its management. WHO defined two strategies for the early detection of BC: 1) early diagnosis, which is the recognition of symptomatic BC at an early stage, and 2) screening, which is the identification of asymptomatic BC in a target population of apparently healthy individuals.[3]
Mammography (MG) is infeasible in certain settings. Given the increasing burden of BC and lack of access to early detection with medical imaging, ultrasonography (US) is an effective primary tool for early detection of BC with high sensitivity and specificity.[4] In addition to the clinical diagnosis, combined imaging using both modalities is more effective in improving the diagnosis of BC.[5] Regarding BC smaller than 2 cm, the sensitivity of MG is greater in patients with a low breast density than in those with a high breast density. US has higher sensitivity than MG, and the combination of US and MG has better sensitivity than US alone.[6]
Medical imaging features usually used to describe breast lesions include the following: 1) shape (round/oval, lobular, or irregular), 2) orientation (parallel or antiparallel), 3) echogenic pattern (hyperechoic, hypoechoic, isoechoic, or mixed echogenicity), 4) margins (circumscribed or uncircumscribed, microlobulated, angular, and speculated), 5) boundary (abrupt or halo), and 6) posterior acoustic features (enhancement, shadowing, mixed, or none).[7] Medical imaging features of malignancy include irregular shape, speculated or angular margins, taller than wider orientation, microcalcification, and posterior acoustic shadowing.[8]
In the literature, many studies confirm the efficacy of combining both US and MG in providing better BC screening and diagnostic outcomes. However, optimized achievement and utility of such outcomes require a deeper understanding of the correlation between the common and modality-specific image features that we and MG typically use as lesion descriptors related to the presence or absence of the disease. Uniquely, this study elucidates the compatibility of both imaging modalities to detect the features of malignancy of BC, which are the cornerstones of getting the correct diagnosis of BC. Early diagnosis of BC dramatically improves prognosis, which is of interest of family doctors. US and MG have a critical role in early diagnosis of BC, which are widely used methods in family centers. Table 1 describes the most common descriptors used by each modality in BC prediction.
Table 1.
Radiographic features of breast lesions are shown in both ultrasound and MG
| Feature | Variables | Categories | Ultrasonography n (%) | Mammography n (%) |
|---|---|---|---|---|
| Mass | Presence of mass | Yes | 263 (100) | 216 (82.1) |
| No | 0 (0.0) | 47 (17.9) | ||
| Shape | Oval or round | Yes | 9 (3.4) | 8 (3.0) |
| No | 254 (96.6) | 255 (97) | ||
| Irregular | Yes | 239 (90.9) | 219 (83.3) | |
| No | 24 (9.1) | 44 (16.7) | ||
| Lobular | Yes | 15 (5.7) | 13 (4.9) | |
| No | 248 (94.3) | 250 (95.1) | ||
| Margins | Circumscribed | Yes | 16 (6.1) | 19 (7.2) |
| No | 247 (93.9) | 244 (92.8) | ||
| Uncircumscribed | Yes | 247 (93.9) | 244 (92.8) | |
| No | 16 (6.1) | 19 (7.2) | ||
| Spiculated | Yes | 93 (35.4) | 134 (51) | |
| No | 170 (64.6) | 129 (49) | ||
| Echogenicity | Hypoechoic | Yes | 250 (95.1) | NA |
| No | 13 (4.9) | NA | ||
| Heterogeneous | Yes | 8 (3.0) | NA | |
| No | 255 (97) | NA | ||
| Density | High density | Yes | NA | 227 (86.3) |
| No | NA | 36 (13.7) | ||
| Heterogeneous | Yes | NA | 25 (9.5) | |
| No | NA | 238 (90.5) | ||
| Calcification | Presence of Microcalcification | Yes | NA | 86 (32.7) |
| No | NA | 177 (67.3) | ||
| Presence of Calcification | Yes | NA | 23 (8.7) | |
| No | NA | 240 (91.3) | ||
| Tissue changes | Tissue distortion | Yes | 200 (76) | 197 (74.9) |
| No | 63 (24) | 66 (25.1) | ||
| Nipple retraction | Yes | 104 (39.5) | 113 (43) | |
| No | 159 (60.5) | 150 (57) | ||
| Skin thickening | Yes | 98 (37.3) | 120 (45.6) | |
| No | 165 (62.7) | 143 (54.4) | ||
| Others | Lymph nodes | Yes | 229 (87.1) | 190 (72.2) |
| No | 34 (12.9) | 73 (27.8) |
Patients and Methods
Study design
In this retrospective study, a total of 263 patients who had been diagnosed with BC were involved. The study was conducted at the Life Center for Cancer Early Detection of the National Cancer Control Foundation (NCCF) in Sana’a, Republic of Yemen, from January 2021 to June 2022. The data were collected from the patient’s electronic records. Three radiologists with more than 10 years of experience in the general US investigated the patients involved in this study. A 7.5 or 10 MHz linear transducer (Samsung Medison, Seoul, Korea) machine was utilized to assess the breast lesions in gray-scale and Doppler modes. Each patient underwent MG using a (Siemens Healthcare, Erlangen, Germany) machine. Following the appropriate positioning and compression of the breast with two transparent plastic paddles, each patient underwent imaging in both craniocaudal (CC) and mediolateral oblique (MLO) views. The images were interpreted by the radiologists who performed the US examinations. Each patient with a breast lesion underwent a breast US followed by MG and was classified 2, 3, 4 (a, b, or c), 5, or 6 according to the fifth edition of the American College of Radiology (ACR) Breast Imaging Reporting and Database System (BI-RADS) US.[9] Then patients who were doubted, suspicious, or highly suspicious underwent a true-cut biopsy (TCB) for histopathology. All biopsy examinations were performed by the same histopathology physician with more than 10 years of experience. Each biopsy was interpreted and categorized as not diagnostic (B1), benign (B2), lesions with uncertain potential (B3), suspicious of malignancy (B4), and malignant (B5) according to the Histopathological B Classification.[10]
Inclusion criteria: The study involved all patients who underwent imaging using both US and MG and were categorized into categories 4 (a, b, or c), 5, and 6 and confirmed to have breast malignancy by TCB and histopathology results. Exclusion criteria include 1) patients who have only US, 2) patients who have only MG, 3) patients with no clear diagnosis by both US and MG, 4) patients who are classified as category 1 or 2, and 5) patients who are classified as B1, B2, B3, or B4 according to the biopsy assessment categories. In addition, the US added other features such as the following: 1. echogenicity (hypoechoic, isoechoic, hyperechoic, and heterogeneous) and 2. calcification (Yes/no). MG added other features as the following: 1. density (hyperdense, hypodense, isodense, or mixed density), 2. microcalcification (Yes/no), and 3. another calcification (Yes/no). Due to the asymmetry of these features on US and MG, they were not included in this study [Figures 1 and 2].
Figure 1.
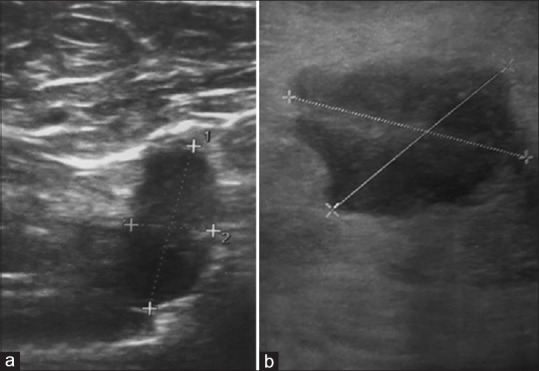
Selected US images of two different patients, shows (a) an irregular shape, spiculated margin, longer than wider, hypoechoic mass perpendicular to the skin line. (b) An irregular shape, circumscribed margin, lobulated, hypoechoic mass, and histologically proven intraductal carcinoma
Figure 2.
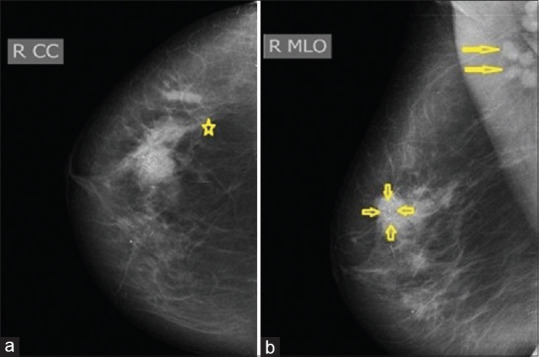
Selected MG images of the right breast of the same patient: (a) craniocaudal (CC) and (b) mediolateral oblique (MLO) shows irregular spiculated dense mass in the upper outer quadrant associated with architecture distortion (star), clustered microcalcification (short arrows), and rounded dense axillary lymph nodes (long arrows)
Statistical analysis
The collected data analysis was analyzed using SPSS, version 25 for Windows (IBM Corp. USA). Descriptive statistics were expressed as frequencies and percentages, and the continuous statistics were expressed as the mean ± standard deviation. A cross-tabulation test was performed to correlate each feature of breast lesion (Yes/No) on both US and MG. The compatibility between the presence of each feature on both imaging techniques was measured by the percentage of agreement in reporting the feature. The average agreement between the two techniques was reported as Kohen’s Kappa (Kappa <0 no agreement, Kappa 0.01–0.2 slight agreement, Kappa 0.21–0.4 fair agreement, Kappa 0.41–0.6 moderate agreement, Kappa 0.61–0.8 substantial agreement, Kappa >0.81 perfect agreement).[11] The strength of association of each feature was measured using the odds ratio (OR), which was assumed to be significant when more than 1, and a 95% confidence interval (CI) of the OR was reported. The P value was assumed to be statistically significant when less than 0.05. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were measured using Microsoft Excel (Microsoft Co., WA, USA). Finally, the receiver operating characteristic (ROC) curve and the area under the curve (AUC) for each feature on both US and MG were used.
Results
In total, 263 female patients with breast malignancy were included in this study. The mean age was 45.71 ± 12.26 years (17–90 years). Among these cases of breast cancer, 48.7% (128 cases) occurred in the right breast, and 51.3% (135 cases) occurred in the left breast.
Table 1 shows the occurrence of radiographic features on both US and MG. A cross-tabulation test of the occurrence of malignancy features on both US and MG shows significant compatibility between the two imaging modalities in the detection of signs of breast lesions, either benign or malignant [Table 2].
Table 2.
Cross-tabulation test between the occurrence of malignancy features on both US and MG
| Feature | Variable | Categories | Mammography* Ultrasonography n (%) | Total agreement n (%) | Kappa (K) | P | Odds Ratio | 95% confidence interval | |
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| Lower | Upper | ||||||||
| Shape | Oval or Round | Yes | 5 (62.5) | 256 (97.33) | 0.575 | <0.001 | 104.58 | 18.37 | 595.31 |
| No | 251 (98.4) | ||||||||
| Irregular | Yes | 212 (96.8) | 229 (87.1) | 0.433 | <0.001 | 19.07 | 7.25 | 50.15 | |
| No | 17 (38.6) | ||||||||
| Lobulated | Yes | 6 (42.2) | 247 (93.62) | 0.397 | <0.001 | 22.952 | 6.398 | 82.34 | |
| No | 241 (96.4) | ||||||||
| Margins | Uncircumscribed | Yes | 238 (97.5) | 248 (94.29) | 0.541 | <0.001 | 44.074 | 13.125 | 148.00 |
| No | 10 (52.6) | ||||||||
| Spiculated | Yes | 70 (52.2) | 176 (66.92) | 0.342 | <0.001 | 5.041 | 2.868 | 8.861 | |
| No | 106 (82.2) | ||||||||
| Tissue changes | Tissue distortion | Yes | 172 (87.3) | 210 (79.85) | 0.456 | <0.001 | 9.337 | 4.905 | 17.772 |
| No | 38 (57.6) | ||||||||
| Nipple retraction | Yes | 79 (69.9) | 204 (77.56) | 0.538 | <0.001 | 11.618 | 6.451 | 20.921 | |
| No | 125 (83.3) | ||||||||
| Skin thickening | Yes | 79 (65.8) | 203 (77.18) | 0.533 | <0.001 | 12.575 | 6.814 | 23.208 | |
| No | 124 (86.7) | ||||||||
| Others | Enlarged lymph nodes | Yes | 183 (96.3) | 210 (79.84) | 0.399 | <0.001 | 15.345 | 6.289 | 37.439 |
| No | 27 (37) | ||||||||
When comparing the sensitivity and specificity of radiographic features that appear in both imaging modalities, it was found that US is more sensitive in detecting irregular shapes, noncircumscribed borders, and enlarged lymph nodes. Moreover, US exhibits higher specificity in detecting noncircumscribed, spiculated margins, nipple retraction, and skin thickening [Table 3, Figure 3].
Table 3.
Sensitivity and specificity of each radiographic feature of malignancy on US and MG
| Feature | Variables | Sensitivity | Specificity | PPV | NPV | ||||
|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
||||||
| US | MG | US | MG | US | MG | US | MG | ||
| Shape | Irregular | 92% | 84% | 27% | 36% | 97% | 97% | 13% | 9% |
| Margin | No circumscribed | 95% | 93% | 27% | 9% | 97% | 96% | 19% | 5% |
| Spiculated | 37% | 52% | 91% | 64% | 99% | 97% | 6% | 5% | |
| Tissue changes | Tissue distortion | 78% | 77% | 64% | 64% | 98% | 98% | 11% | 11% |
| Nipple retraction | 40% | 44% | 82% | 73% | 98% | 97% | 6% | 5% | |
| Skin thickening | 38% | 47% | 91% | 82% | 99% | 98% | 6% | 6% | |
| Others | Enlarged lymph nodes | 88% | 73% | 27% | 55% | 97% | 97% | 9% | 8% |
US=Ultrasonography, MG=Mammography, PPV=Positive predictive value, NPV=Negative predictive value
Figure 3.
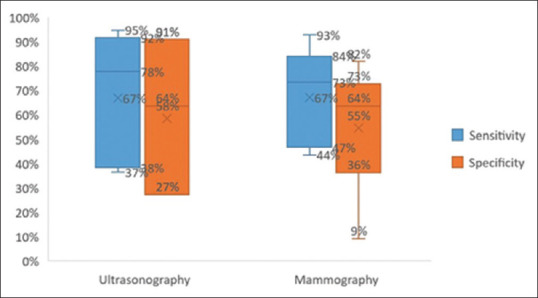
Poxplot shows that US’s highest sensitivity and specificity are 95% and 91%. However, MG’s highest sensitivity and specificity are 93% and 82%
The ROC curve shows the AUC of each feature of BC on US and MG, and it revealed convergence in the number of AUCs of each feature [Figures 4 and 5].
Figure 4.
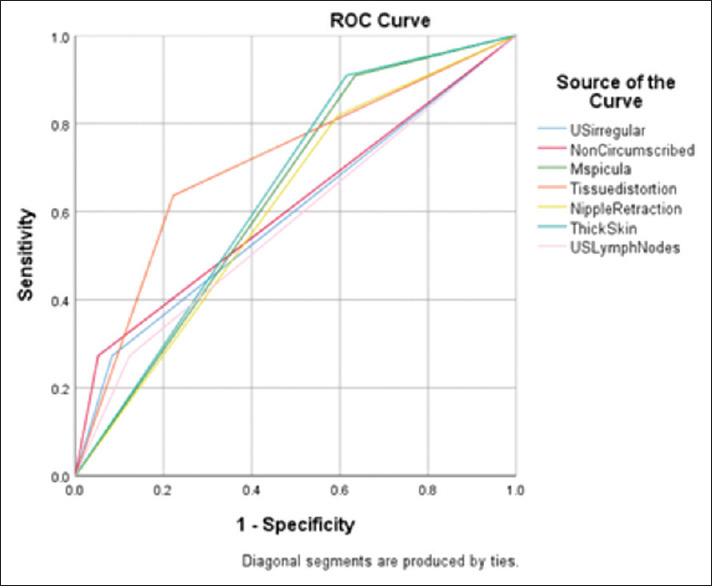
ROC curve shows the AUC of each feature of BC on US and revealed that AUC of irregular shape = 0.595, AUC of uncircumscribed = 0.611, AUC of speculated margins = 0.637, AUC of tissue distortion = 0.707, AUC of nipple retraction = 0.611, AUC of skin thickening = 0.647, AUC of lymphadenopathy = 0.575
Figure 5.
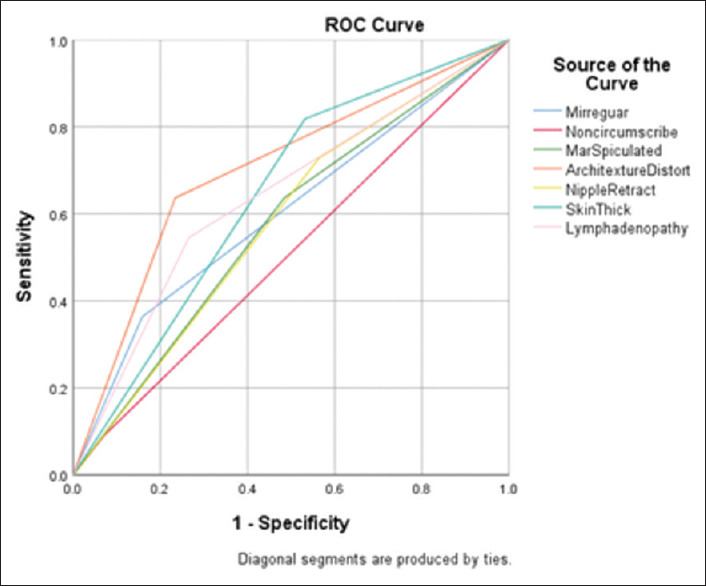
ROC curve shows the AUC of each feature of BC on MG and revealed that AUC of irregular shape = 0.602, AUC of uncircumscribed = 0.510, AUC of spiculated margins = 0.576, AUC of tissue distortion = 0.701, AUC of nipple retraction = 0.582, AUC of skin thickening = 0.643, AUC of lymphadenopathy = 0.640
Discussion
US and MG are commonly used to assess the typical features of breast lesions and to determine the likelihood of malignancy, including irregular shape, noncircumscribed spiculated, microlobulated or angular margins, taller than wider orientation, microcalcification, posterior acoustic shadowing, tissue distortion, skin thickening, and the presence of lymphadenopathy, which are the cornerstone to get the correct diagnosis of BC. This study compared the sensitivity and specificity of each medical imaging modality feature of malignancy to appear on US and MG in histopathological proved cases of BC.
This study revealed that irregular shape has 92% and 84% sensitivity with 27% and 36% specificity in US and MG, respectively. The ROC curve showed that the AUC was 0.595 and 0.602 in the US and MG, respectively. These results reflect high sensitivity to the occurrence of irregular shape in BC on both US and MG; however, irregular shape has low specificity for BC on both imaging modalities. These results were explained by Kim et al.,[12] who reported that irregular hypoechoic breast masses in the US did not always indicate BC and various benign breast lesions could show irregular shapes such as 1) inflammatory lesions including abscess, idiopathic granulomatous lobular mastitis, and diabetic mastopathy; 2) iatrogenic or trauma-related including fat necrosis, fibrotic scar, and foreign-body reaction; 3) sclerosing adenosis, apocrine metaplasia, and fibrocystic disease; and 4) benign breast lesions including intraductal papilloma, fibroadenoma, and tubular adenoma.
The study’s findings indicated that uncircumscribed margins are more sensitive in detecting BC in the US (95%) than in MG (93%). However, the specificity of uncircumscribed margins was low in the US (27%) and MG (9%). In other words, while uncircumscribed margins are better at detecting breast cancer in the US, they may also lead to more false positive results compared to MG. The ROC curve shows that the AUC for uncircumscribed margins was 0.611 and 0.510 in the US and MG, respectively. The spiculated margins have 37% and 52% sensitivity, with 91% and 64% specificity on US and MG, respectively. The ROC curve showed that the AUC for spiculated margins was 0.637 and 0.576 in the US and MG, respectively. The finding aligns with Choi et al.,[13] who reported that the irregular shape and noncircumscribed margins of breast lesions combined with contrast enhancement are reliable signs to distinguish malignant breast lesions incidentally discovered on routine chest CT. Bin Saeedan et al.[14] reported that speculated margins, irregular shape, and mass enhancement after contrast administration on CT have a high PPV for BC.
Architectural distortion is tissue distortion of the breast parenchyma with no accompanied definite mass or density. It is a localized mammographic sign of early BC that may be difficult to detect.[15] The study found that tissue distortion has 78% on US and 77% sensitivity on MG, with 64% specificity, 98% PPV, and 11% NPV on both modalities for BC. The ROC curve showed that the AUC was 0.607 and 0.601 for US and MG, respectively. Our findings showed that tissue distortion is the most significant sign of malignancy in both imaging modalities. In the literature, Nwammuo et al.[16] reported that irregular outline and architectural distortion were a feature of malignancy in 86.7% and 80% of MG. Sanmugasiva et al.[17] reported 92.8% PPV for architectural distortion for breast malignancy. Another study reported that architectural distortion was the third most common mammographic sign of nonpalpable BC.[18]
Regarding nipple retraction and skin thickening, our study found high specificity and PPV for these features. However, they had low sensitivity. ROC curve shows 0.611 and 0.582 AUC for nipple retraction and AUC of 0.647 and 0.643 for skin thickening for US and MG, respectively. Ebubedike et al.[19] reported that nipple retraction, tissue distortion, skin thickening, lymph node enlargement, and calcification within abreast mass were the mammographic findings of BC screening in patients with a family history of BC.
Enlarged lymph nodes have suspicious malignancy features, including diffuse or focal cortical thickening, effacement of the fatty hilum, and irregular margins.[20] Our study found that the presence of enlarged lymph nodes has 88% and 73% sensitivity with 27% and 55% specificity on US and MG, respectively. ROC curve shows 0.575 and 0.640 AUC for enlarged axillary lymphadenopathy. We attributed the low specificity of lymphadenopathy to the fact that it is not always a sign of malignancy. Pinheiro et al.[21] reported that lymph node cortical thickening and hilum effacement are US features of malignancy. However, other adjunctive techniques may be needed to differentiate malignant lymphadenopathy. Cho et al.[22] reported that the morphologic analysis of axillary lymph nodes on diffusion-weighted magnetic resonance imaging images, long diameter, short diameter, and cortical thickness help differentiate metastatic from benign lymph nodes.
MG is an effective screening modality for early detection of BC. However, more than 25% of nonmass breast lesions are missed on MG. US is an important complementary modality for BC screening, especially for dense breasts.[23] Our study revealed that while US and MG demonstrated high sensitivity in diagnosing BC, their specificity was moderate. A previous study by Li et al.[24] reported high specificity (84.6%) for MG to diagnose BC. Sood et al.[4] reported an overall 80.1% sensitivity and 88.4% specificity for US for diagnosis of BC. Zeeshan et al.[25] reported 97% and 64.5% sensitivity and specificity for digital MG for diagnosis of BC.
Ultimately, both US and MG exhibit high sensitivity, PPV, and acceptable specificity; conversely, they have low NPV. Previous studies explained this as many benign lesions can mimic breast cancer.[12,26] The US is preferred for its ability to provide real-time imaging and utilize color and pulsed Doppler techniques to study the blood supply to breast lesions, which enhances its diagnostic accuracy.[27] The ACR criteria of MG include Type 1, predominantly fatty (<25% dense tissue); Type 2, scattered fibroglandular tissue densities (25–50% dense tissue); Type 3, heterogeneous dense breast (50–75% dense tissue); and Type 4, extremely dense breast (>75% dense tissue).[28] This difference in tissue densities significantly affects MG’s sensitivity in detecting breast lesions, making it lower than the US in sensitivity and specificity. Parmar et al.[29] reported that US is more accurate than MG in young women with dense breast tissue, US has higher sensitivity than MG (95.5% vs 79.5%), and the combination of both imaging modalities has the highest sensitivity (97.7%), and specificity (95.6%).
Conclusion
The morphological changes on US and MG images, including the irregular shape of mass with uncircumscribed margins, tissue distortion, nipple retraction, skin thickening, and the presence of lymphadenopathy, occur with approximately equal sensitivity and specificity on both US and MG. The US has the advantage of describing the echogenicity of real-time imaging and using color and pulsed Doppler techniques to study the blood supply to the breast lesion and detect axillary lymphadenopathy, which increases its diagnostic accuracy. MG has the advantage of describing the types of calcifications, either microcalcification or macrocalcification. The gold standard for diagnosis of BC is histopathology examination, which depends on appropriate tissue sampling biopsy.
Ethical approval
This study is approved by the Institutional Ethics Committee of the NCCF (No. 154), Sana’a, Republic of Yemen. Due to the retrospective nature of the study, patients’ informed consent was waived.
Limitations
1-There is invalidity of all detailed features of the margins of the lesions (indistinct, angular, or microlobulated) in all the preserved US and MG reports of the involved patients, so we involved only the available features in this study.
2-The calcification type was not determined into microcalcification or another type in the available reports of the US, and the nature of this technique cannot detect calcification in all patients. Therefore, cross-tabulation between the presence of microcalcification on both techniques was also omitted.
3-The US describes the contents of the lesion using echogenicity, and MG describes the contents using density. Thus, the correlation could be more logical, and the omission of these features helps both imaging modalities’ overall calculated sensitivity and accuracy.
Authors contribution
SAA: Conceptualized idea, analyzed data and wrote the manuscript. AAA: performed US and MG examinations and collected data. MG and AG: revised data analysis. KDA and AFA: revised the manuscript and edited language.
Conflicts of interest
There are no conflicts of interest
Funding Statement
Nil.
References
- 1.Wilkinson L, Gathani T. Understanding breast cancer as a global health concern. Br J Radiol. 2022;95:20211033. doi: 10.1259/bjr.20211033. doi: 10.1259/bjr.20211033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nafie MS, Boraei ATA. Exploration of novel VEGFR2 tyrosine kinase inhibitors via design and synthesis of new alkylated indolyl-triazole Schiff bases for targeting breast cancer. Bioorg Chem. 2022;122:105708. doi: 10.1016/j.bioorg.2022.105708. doi: 10.1016/j.bioorg.2022.105708. [DOI] [PubMed] [Google Scholar]
- 3.Ginsburg O, Yip CH, Brooks A, Cabanes A, Caleffi M, Dunstan Yataco JA, et al. Breast cancer early detection: A phased approach to implementation. Cancer. 2020;126(Suppl 10):2379–93. doi: 10.1002/cncr.32887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sood R, Rositch AF, Shakoor D, Ambinder E, Pool KL, Pollack E, et al. Ultrasound for breast cancer detection globally: A systematic review and meta-analysis. J Glob Oncol. 2019;5:1–17. doi: 10.1200/JGO.19.00127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zhang W, Xu C, Li R, Cui G, Wang M, Wang M. Correlation analysis between ultrasonography and mammography with other risk factors related to breast cancer. Oncol Lett. 2019;17:5511–6. doi: 10.3892/ol.2019.10246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chen HL, Zhou JQ, Chen Q, Deng YC. Comparison of the sensitivity of mammography, ultrasound, magnetic resonance imaging and combinations of these imaging modalities for the detection of small (≤2?cm) breast cancer. Medicine (Baltimore) 2021;100:e26531. doi: 10.1097/MD.0000000000026531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ha R, Kim H, Mango V, Wynn R, Comstock C. Ultrasonographic features and clinical implications of benign palpable breast lesions in young women. Ultrasonography. 2015;34:66–70. doi: 10.14366/usg.14043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Agrawal G, Su MY, Nalcioglu O, Feig SA, Chen JH. Significance of breast lesion descriptors in the ACR BI-RADS MRI lexicon. Cancer. 2009;115:1363–80. doi: 10.1002/cncr.24156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mohapatra SK, Das PK, Nayak RB, Mishra A, Nayak B. Diagnostic accuracy of mammography in characterizing breast masses using the 5th edition of BI-RADS: A retrospective study. Cancer Res Stat Treat. 2022;5:52–8. [Google Scholar]
- 10.Jörg I, Wieler J, Elfgen C, Bolten K, Hutzli C, Talimi J, et al. Discrepancies between radiological and histological findings in preoperative core needle (CNB) and vacuum-assisted (VAB) breast biopsies. J Cancer Res Clin Oncol. 2021;147:749–54. doi: 10.1007/s00432-020-03481-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.McHugh ML. Interrater reliability: The kappa statistic. Biochem Med (Zagreb) 2012;22:276–82. [PMC free article] [PubMed] [Google Scholar]
- 12.Kim YR, Kim HS, Kim HW. Are irregular hypoechoic breast masses on ultrasound always malignancies?: A pictorial essay. Korean J Radiol. 2015;16:1266–75. doi: 10.3348/kjr.2015.16.6.1266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Choi YJ, Kim TH, Cha YJ, Son EJ, Gweon HM, Park CH. Incidental breast lesions on chest CT: Clinical significance and differential features requiring referral. J Korean Soc Radiol. 2018;79:303–10. [Google Scholar]
- 14.Bin Saeedan M, Mobara M, Arafah MA, Mohammed TL. Breast lesions on chest computed tomography: Pictorial review with mammography and ultrasound correlation. Curr Probl Diagn Radiol. 2015;44:144–54. doi: 10.1067/j.cpradiol.2014.09.002. [DOI] [PubMed] [Google Scholar]
- 15.Rangayyan RM, Banik S, Desautels JE. Detection of architectural distortion in prior mammograms via analysis of oriented patterns. J Vis Exp. 2013;50341 doi: 10.3791/50341. doi: 10.3791/50341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Nwammuo BC, Umeh EO, Ebubedike UR, Nwosu SC, Elendu KC, Umeokafor CC, et al. Accuracy of mammography in the diagnosis of breast cancer. Int J Med Health Dev. 2022;27:251–60. [Google Scholar]
- 17.Sanmugasiva VV, Ramli Hamid MT, Fadzli F, Rozalli FI, Yeong CH, Ab Mumin N, et al. Diagnostic accuracy of digital breast tomosynthesis in combination with 2D mammography for the characterisation of mammographic abnormalities. Sci Rep. 2020;10:20628. doi: 10.1038/s41598-020-77456-6. doi: 10.1038/s41598-020-77456-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rangayyan RM, Banik S, Desautels JE. Computer-aided detection of architectural distortion in prior mammograms of interval cancer. J Digit Imaging. 2010;23:611–31. doi: 10.1007/s10278-009-9257-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ebubedike UR, Umeh EO, C Anyanwu SN. Mammographic findings of breast cancer screening in patients with positive family history in South-East Nigeria. Niger J Clin Pract. 2018;21:801–6. doi: 10.4103/njcp.njcp_55_18. [DOI] [PubMed] [Google Scholar]
- 20.van Nijnatten TJA, Jochelson MS, Lobbes MBI. Axillary lymph node characteristics in breast cancer patients versus post-COVID-19 vaccination: Overview of current evidence per imaging modality. Eur J Radiol. 2022;152:110334. doi: 10.1016/j.ejrad.2022.110334. doi: 10.1016/j.ejrad.2022.110334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Pinheiro DJ, Elias S, Nazário AC. Axillary lymph nodes in breast cancer patients: Sonographic evaluation. Radiol Bras. 2014;47:240–4. doi: 10.1590/0100-3984.2013.1689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cho P, Park CS, Park GE, Kim SH, Kim HS, Oh SJ. Diagnostic usefulness of diffusion-weighted mri for axillary lymph node evaluation in patients with breast cancer. Diagnostics (Basel) 2023;13:513. doi: 10.3390/diagnostics13030513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zhang J, Cai L, Pan X, Chen L, Chen M, Yan D, et al. Comparison and risk factors analysis of multiple breast cancer screening methods in the evaluation of breast non-mass-like lesions. BMC Med Imaging. 2022;22:202. doi: 10.1186/s12880-022-00921-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Li H, Zhang S, Wang Q, Zhu R. Clinical value of mammography in diagnosis and identification of breast mass. Pak J Med Sci. 2016;32:1020–5. doi: 10.12669/pjms.324.9384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Zeeshan M, Salam B, Khalid QSB, Alam S, Sayani R. Diagnostic accuracy of digital mammography in the detection of breast cancer. Cureus. 2018;10:e2448. doi: 10.7759/cureus.2448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mario J, Venkataraman S, Dialani V, MD;Slanetz PJ. Benign breast lesions that mimic cancer: Determining radiologic-pathologic concordance. Appl Radiol. 2015;44:28–32. [Google Scholar]
- 27.Binnuhaid AA, Alshoabi SA, Alhazmi FH, Daqqaq TS, Salih SG, Al-Dubai SA. Predictive value of ultrasound imaging in differentiating benign from malignant breast lesions taking biopsy results as the standard. J Family Med Prim Care. 2019;8:3971–6. doi: 10.4103/jfmpc.jfmpc_827_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bargalló X, Velasco M, Santamaría G, Del Amo M, Arguis P, Sánchez Gómez S. Role of computer-aided detection in very small screening detected invasive breast cancers. J Digit Imaging. 2013;26:572–7. doi: 10.1007/s10278-012-9550-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Parmar J, Choudhary S, Zope A, Patel T, Chaudhari N, Shah S, et al. Comprehensive comparison of diagnostic accuracy of ultrasound and mammography in young women with radiographically dense breasts. Arch Clin Biomed Res. 2022;6:308–21. [Google Scholar]