

Abstract
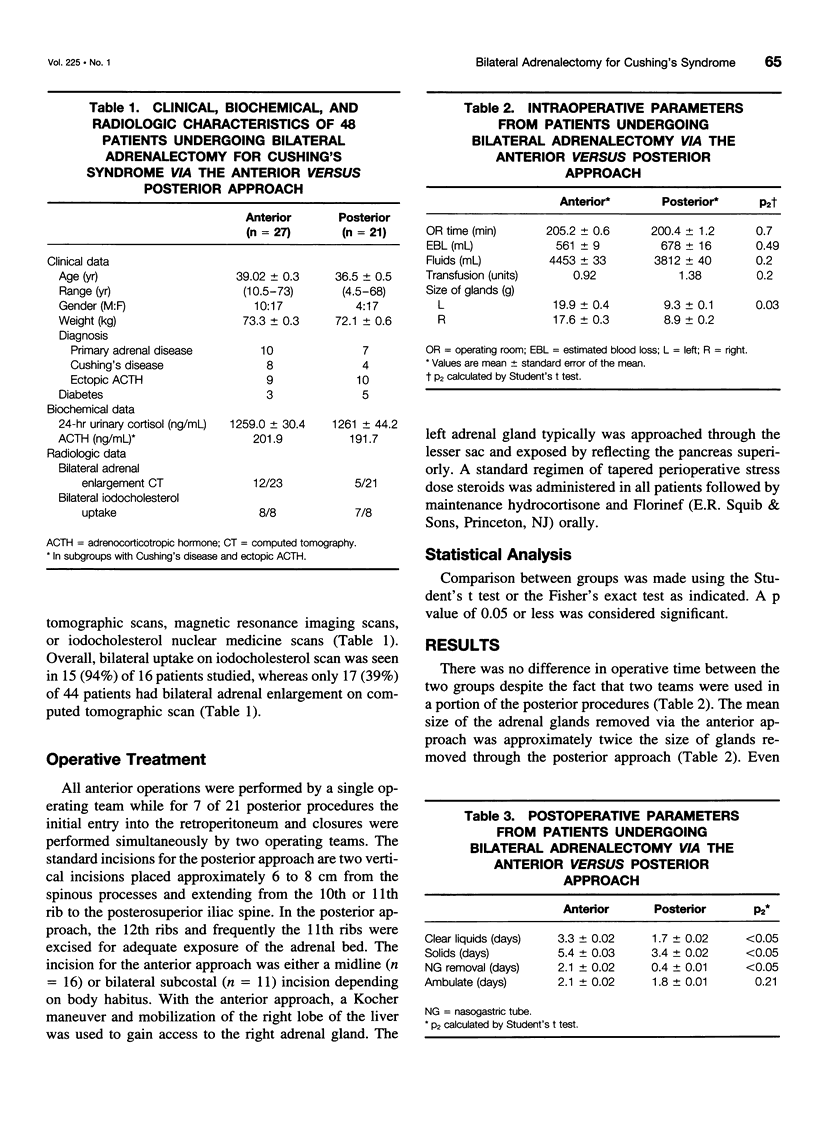
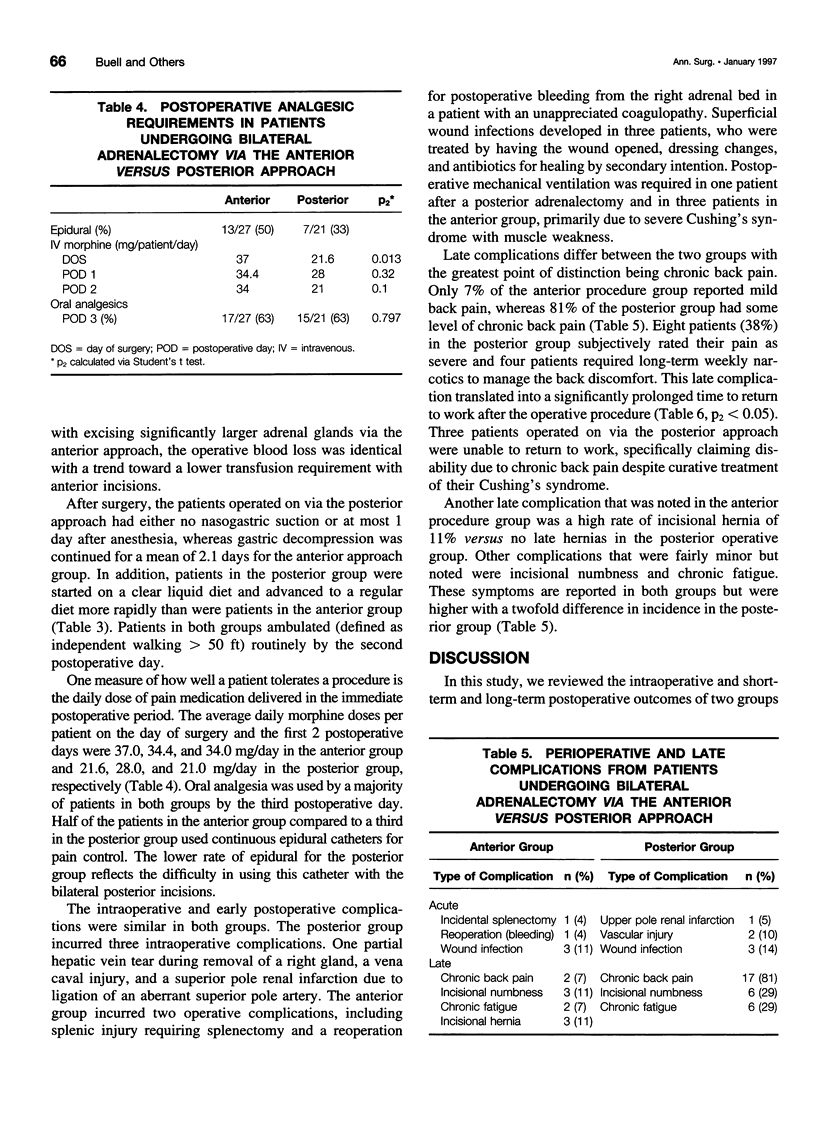
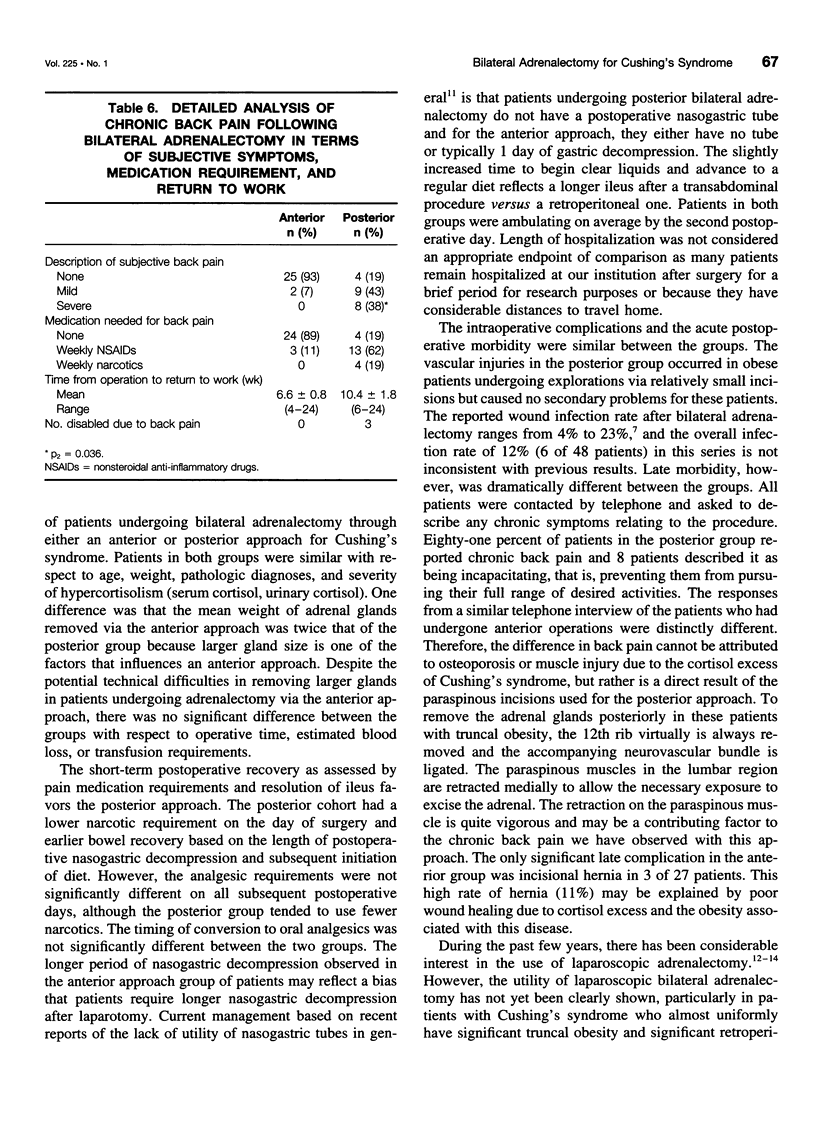
OBJECTIVE: This study evaluates the intraoperative and postoperative complications in patients with Cushing's syndrome who underwent bilateral adrenalectomy comparing the posterior or anterior operative approach. BACKGROUND: The posterior approach for bilateral adrenalectomy has been advocated over the anterior approach because of rapid recovery and decreased morbidity, but the long-term complications associated with each procedure are not well described. METHODS: The intraoperative profiles and morbidity in 48 patients undergoing bilateral adrenalectomy for Cushing's disease through either the anterior or posterior approach from 1985 to the present were reviewed comparing the intraoperative complication and early and late postoperative complication rate and morbidity. RESULTS: Twenty-seven patients underwent an anterior transabdominal procedure, whereas 21 underwent a posterior retroperitoneal procedure via bilateral incisions. Age, weight, and diagnostic categories of Cushing's syndrome were similar between the two groups as well as serum cortisol and 24-hour urinary cortisol levels. Operative time, estimated blood loss, and transfusion requirements were not different between the groups, even though adrenal glands excised through the anterior approach were significantly larger. Acute morbidity was similar between the groups. However, 17 (81%) of 21 patients who underwent posterior bilateral adrenalectomy suffered from chronic back pain, compared with 2 (7%) of 27 via the anterior approach. Five of these patients in the posterior group considered the pain incapacitating, and the mean time to return to work was significantly longer in the posterior group because of back pain. CONCLUSIONS: The anterior approach to bilateral adrenalectomy has comparable intraoperative complications and early morbidity compared to the posterior approach. The posterior approach has a very high incidence of chronic incision-related back pain. The anterior approach is the preferred open surgical technique in most patients undergoing bilateral adrenalectomy for Cushing's syndrome without other contraindications for undergoing laparotomy.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cheatham M. L., Chapman W. C., Key S. P., Sawyers J. L. A meta-analysis of selective versus routine nasogastric decompression after elective laparotomy. Ann Surg. 1995 May;221(5):469–478. doi: 10.1097/00000658-199505000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen K. L., Noth R. H., Pechinski T. Incidence of pituitary tumors following adrenalectomy. A long-term follow-up study of patients treated for Cushing's disease. Arch Intern Med. 1978 Apr;138(4):575–579. doi: 10.1001/archinte.138.4.575. [DOI] [PubMed] [Google Scholar]
- Evans R. M., Hulbert J. C., Reddy P. K. Complications of laparoscopy. Semin Urol. 1992 Aug;10(3):164–168. [PubMed] [Google Scholar]
- Gagner M., Lacroix A., Prinz R. A., Bolté E., Albala D., Potvin C., Hamet P., Kuchel O., Quérin S., Pomp A. Early experience with laparoscopic approach for adrenalectomy. Surgery. 1993 Dec;114(6):1120–1125. [PubMed] [Google Scholar]
- Go H., Takeda M., Takahashi H., Imai T., Tsutsui T., Mizusawa T., Nishiyama T., Morishita H., Nakajima Y., Sato S. Laparoscopic adrenalectomy for primary aldosteronism: a new operative method. J Laparoendosc Surg. 1993 Oct;3(5):455–459. doi: 10.1089/lps.1993.3.455. [DOI] [PubMed] [Google Scholar]
- Lairmore T. C., Ball D. W., Baylin S. B., Wells S. A., Jr Management of pheochromocytomas in patients with multiple endocrine neoplasia type 2 syndromes. Ann Surg. 1993 Jun;217(6):595–603. doi: 10.1097/00000658-199306000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'Riordain D. S., Farley D. R., Young W. F., Jr, Grant C. S., van Heerden J. A. Long-term outcome of bilateral adrenalectomy in patients with Cushing's syndrome. Surgery. 1994 Dec;116(6):1088–1094. [PubMed] [Google Scholar]
- Russell C. F., Hamberger B., van Heerden J. A., Edis A. J., Ilstrup D. M. Adrenalectomy: anterior or posterior approach? Am J Surg. 1982 Sep;144(3):322–324. doi: 10.1016/0002-9610(82)90010-1. [DOI] [PubMed] [Google Scholar]
- Sarkar R., Thompson N. W., McLeod M. K. The role of adrenalectomy in Cushing's syndrome. Surgery. 1990 Dec;108(6):1079–1084. [PubMed] [Google Scholar]
- Suzuki K., Kageyama S., Ueda D., Ushiyama T., Kawabe K., Tajima A., Aso Y. Laparoscopic adrenalectomy: clinical experience with 12 cases. J Urol. 1993 Oct;150(4):1099–1102. doi: 10.1016/s0022-5347(17)35696-3. [DOI] [PubMed] [Google Scholar]
- Zeiger M. A., Fraker D. L., Pass H. I., Nieman L. K., Cutler G. B., Jr, Chrousos G. P., Norton J. A. Effective reversibility of the signs and symptoms of hypercortisolism by bilateral adrenalectomy. Surgery. 1993 Dec;114(6):1138–1143. [PubMed] [Google Scholar]
- van Heerden J. A., Sheps S. G., Hamberger B., Sheedy P. F., 2nd, Poston J. G., ReMine W. H. Pheochromocytoma: current status and changing trends. Surgery. 1982 Apr;91(4):367–373. [PubMed] [Google Scholar]
- van Heerden J. A., Young W. F., Jr, Grant C. S., Carpenter P. C. Adrenal surgery for hypercortisolism--surgical aspects. Surgery. 1995 Apr;117(4):466–472. doi: 10.1016/s0039-6060(05)80069-8. [DOI] [PubMed] [Google Scholar]