

Abstract
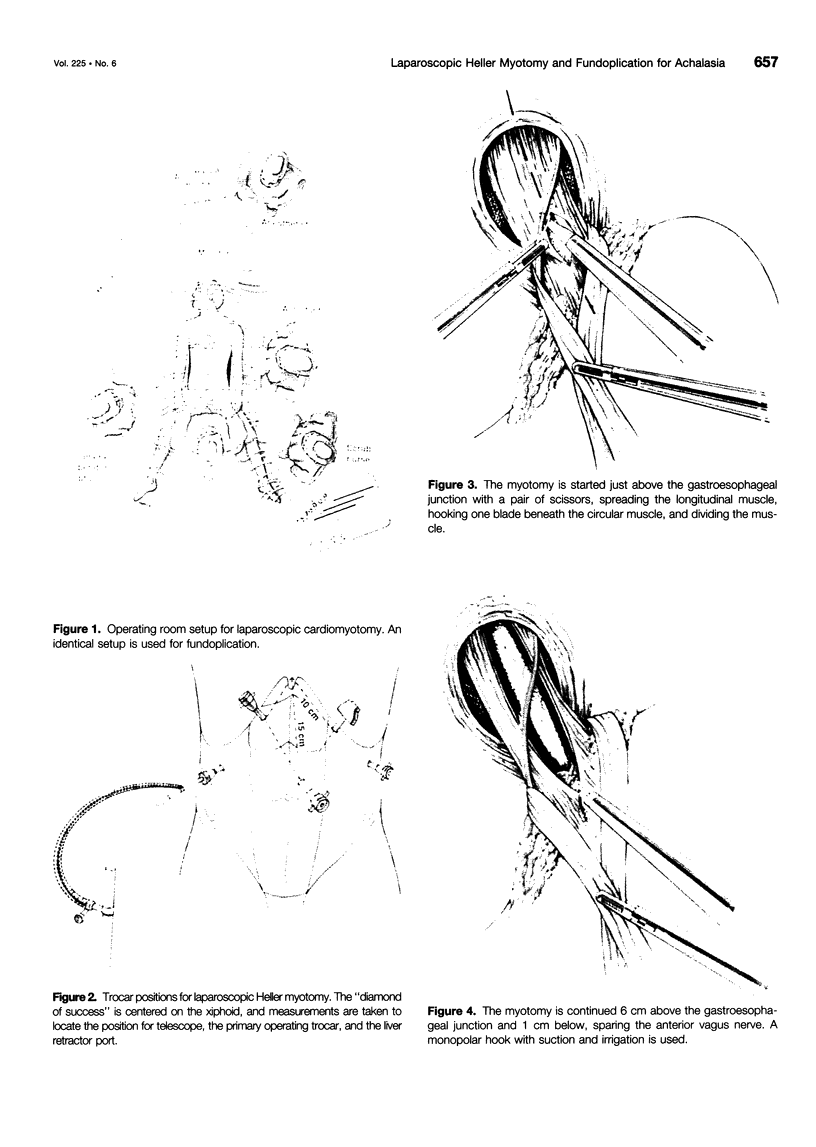
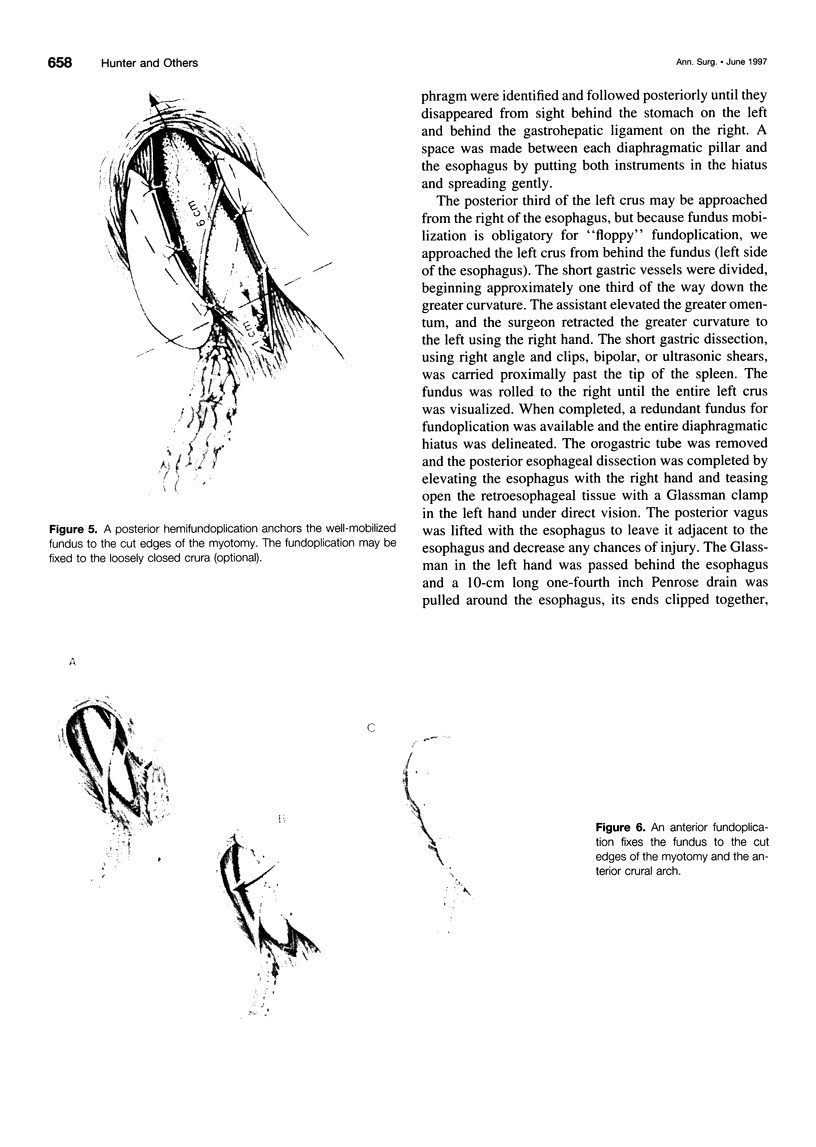
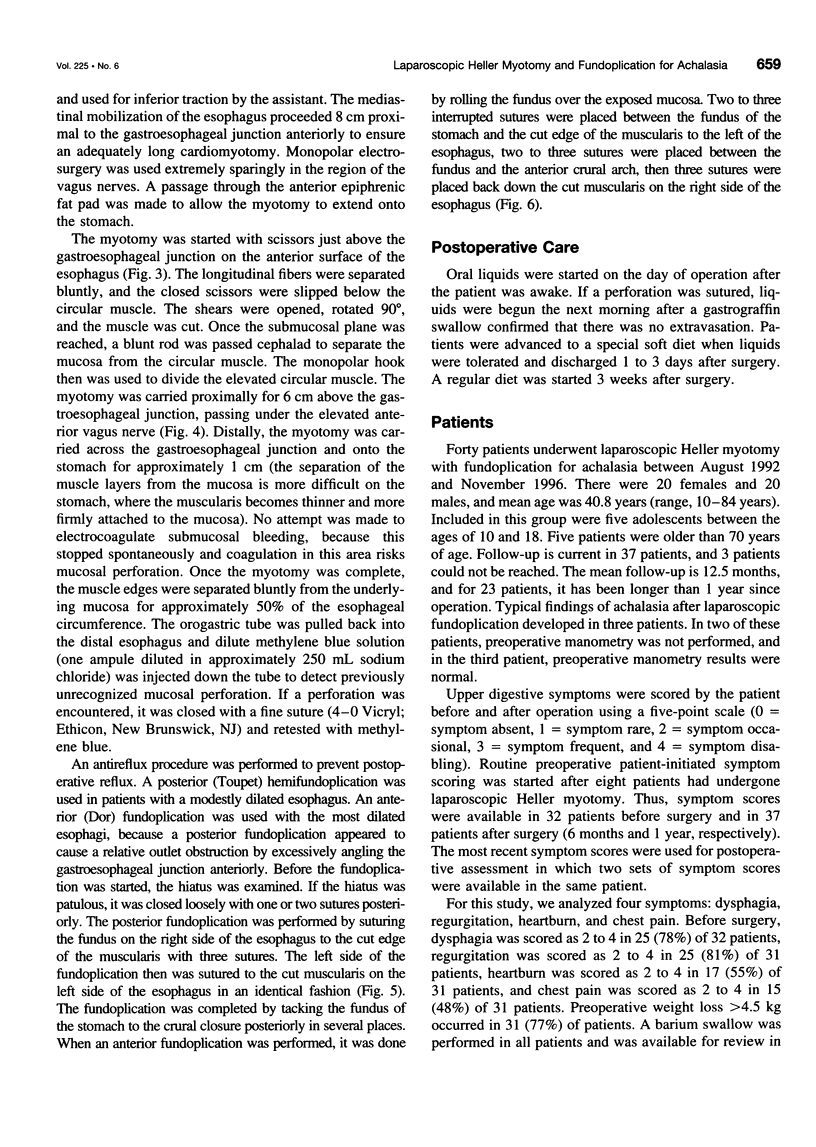
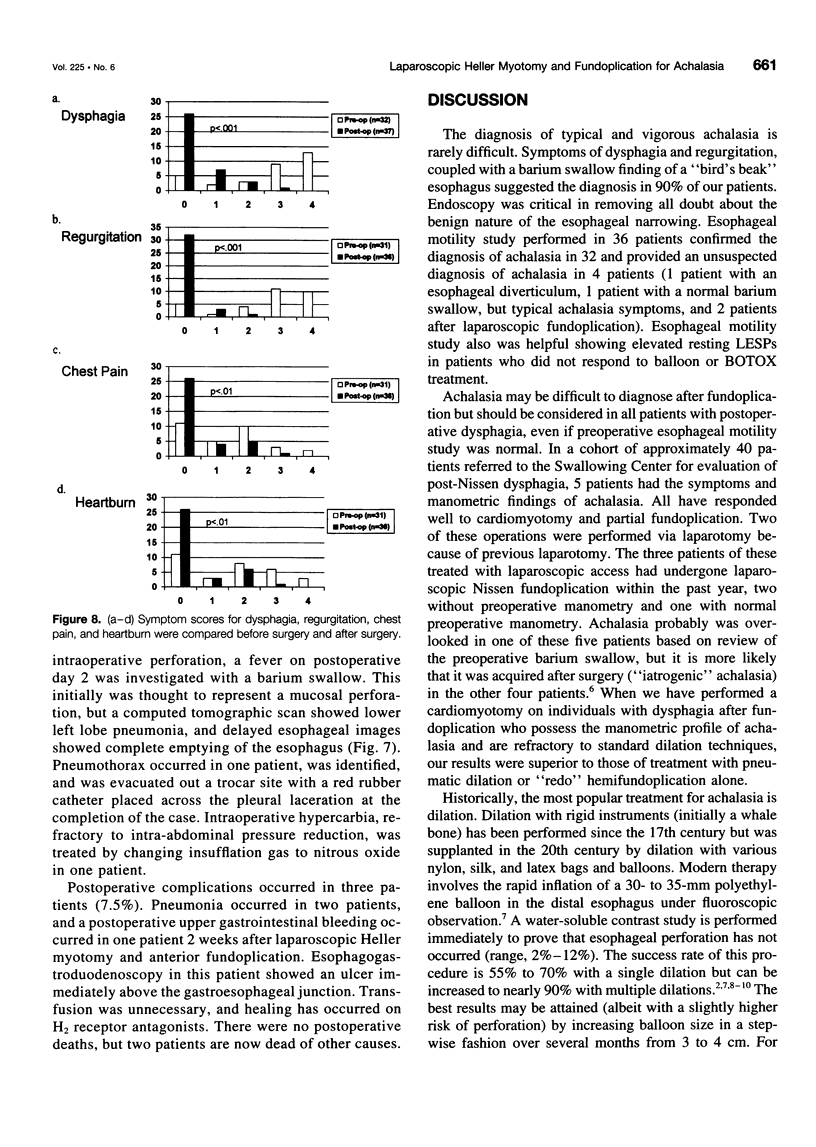
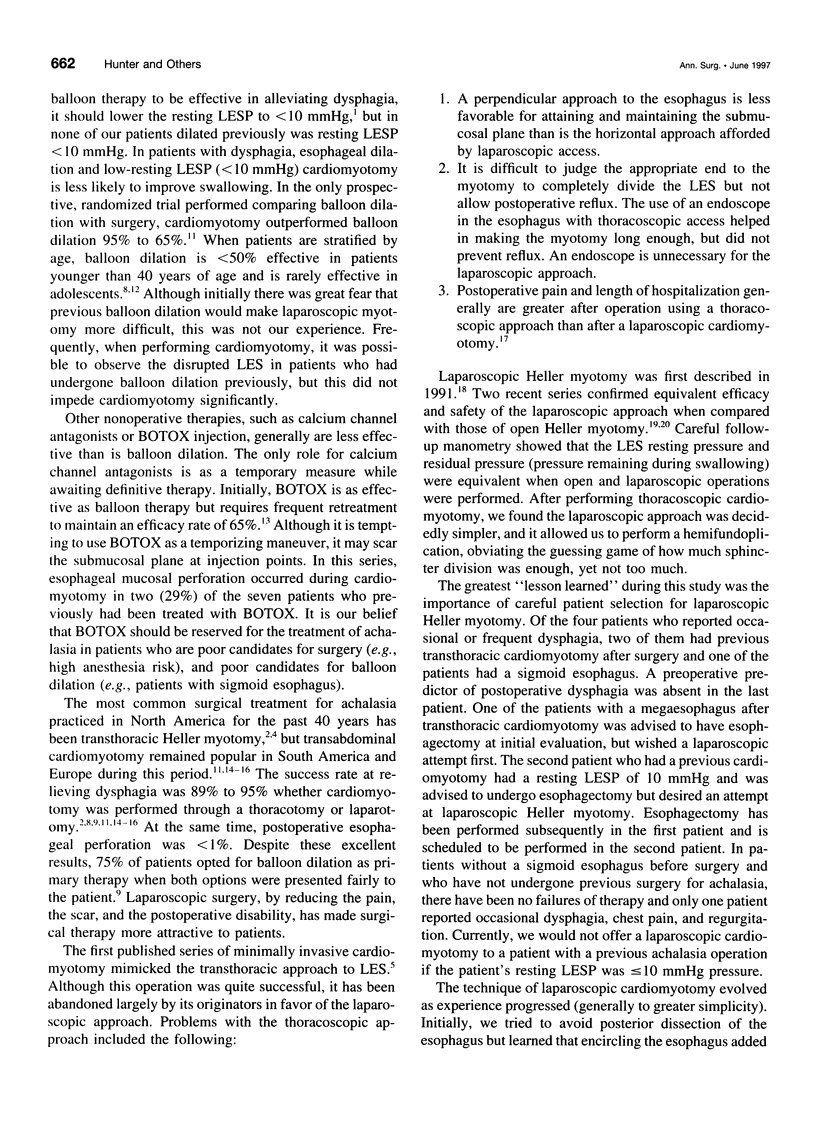
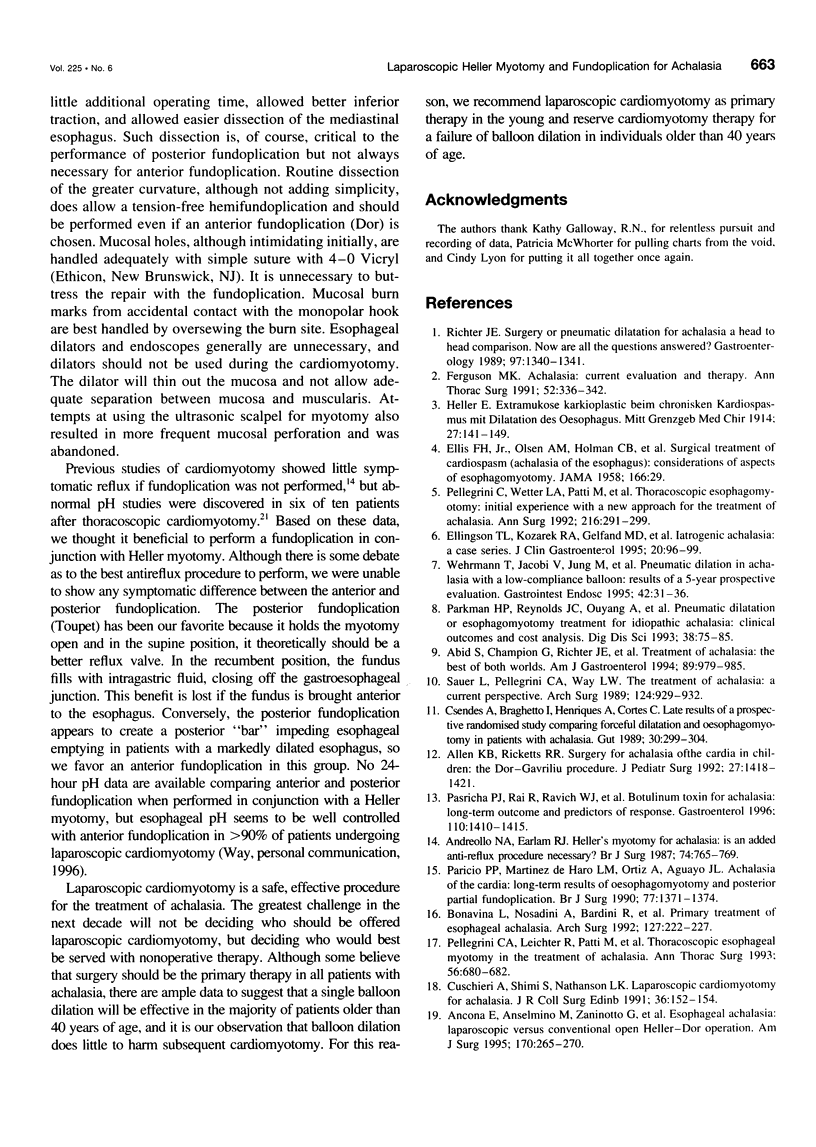
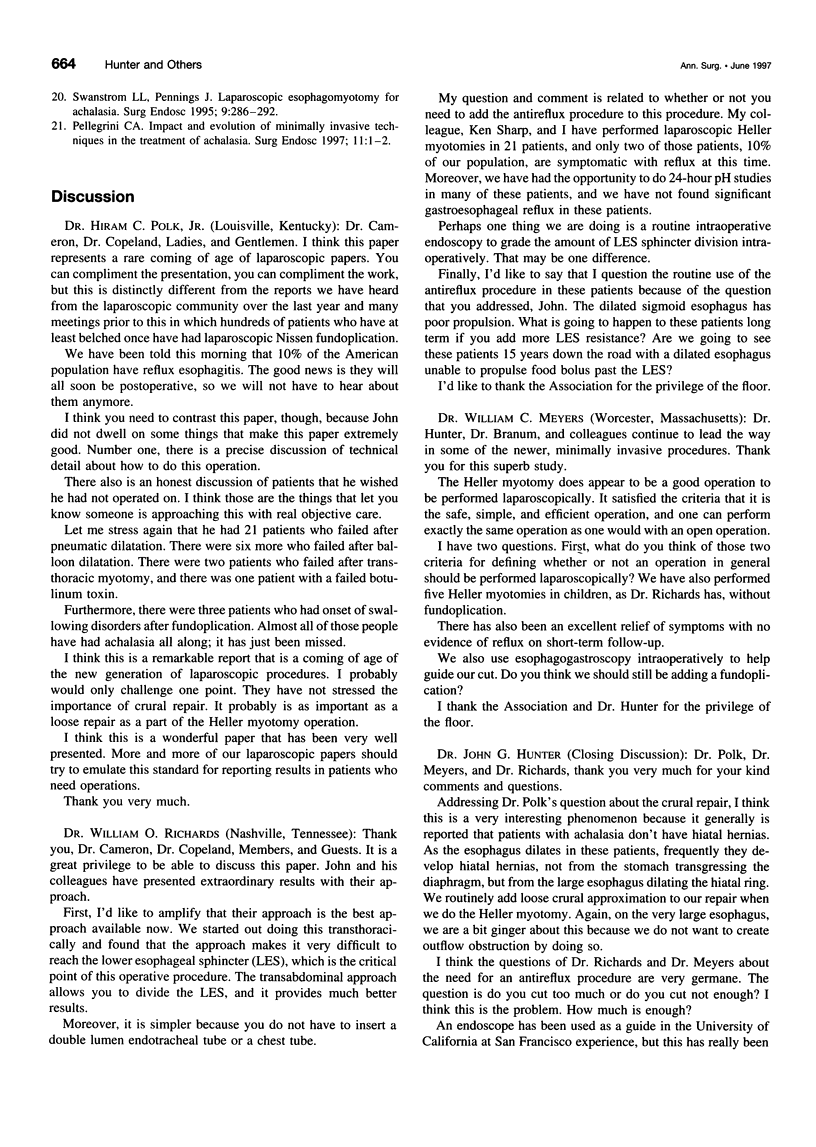
OBJECTIVE: The goal of this study was to review the authors' results with laparoscopic cardiomyotomy and partial fundoplication for achalasia. SUMMARY BACKGROUND DATA: Pneumatic dilatation and botulinum toxin (BOTOX) injection of the lower esophageal sphincter largely have replaced cardiomyotomy for treatment of achalasia. After a brief experience with a thoracoscopic approach, the authors elected to perform cardiomyotomy laparoscopically, in combination with a partial fundoplication (anterior or posterior). PATIENTS AND METHODS: Forty patients were treated between July 1992 and November 1996. Thirty patients had previous therapy of achalasia, 21 with pneumatic dilation, 1 with BOTOX, 6 with balloon and BOTOX, and 2 with transthoracic cardiomyotomy. Three patients had previous laparoscopic fundoplication for gastroesophageal reflux. Symptom scores (0 = none to 4 = disabling) were obtained before surgery and after surgery. Barium swallows and esophagogastroduodenoscopy were performed in all patients. Esophageal motility study was performed in 36 patients. Laparoscopic Heller myotomy and fundoplication was performed through five upper abdominal trocars. A 7-cm myotomy extended 6 cm above the GE junction and 1 cm below the GE junction. A posterior fundoplication was performed in 32 patients, anterior fundoplication in 7 patients, and no fundoplication in 1 patient. Statistical inference was performed with a Wilcoxon signed rank test. RESULTS: Mean operative duration was 199 +/- 36.2 minutes. Mean hospital stay was 2.75 days (range, 1-13 days). Dysphagia was alleviated in all but four patients (90%), and regurgitation in all but two patients (95%) (p < 0.001). Chest pain and heartburn improved significantly (p < 0.01) as well. Intraoperative complications included mucosal laceration in six patients and hypercarbia in one. Postoperative pneumonia developed in two patients, and one patient had moderate hemorrhage from an esophageal ulcer 2 weeks after surgery. CONCLUSIONS: Laparoscopic cardiomyotomy and fundoplication appears to provide definitive treatment of achalasia with rapid rehabilitation and few complications.
Full text
PDF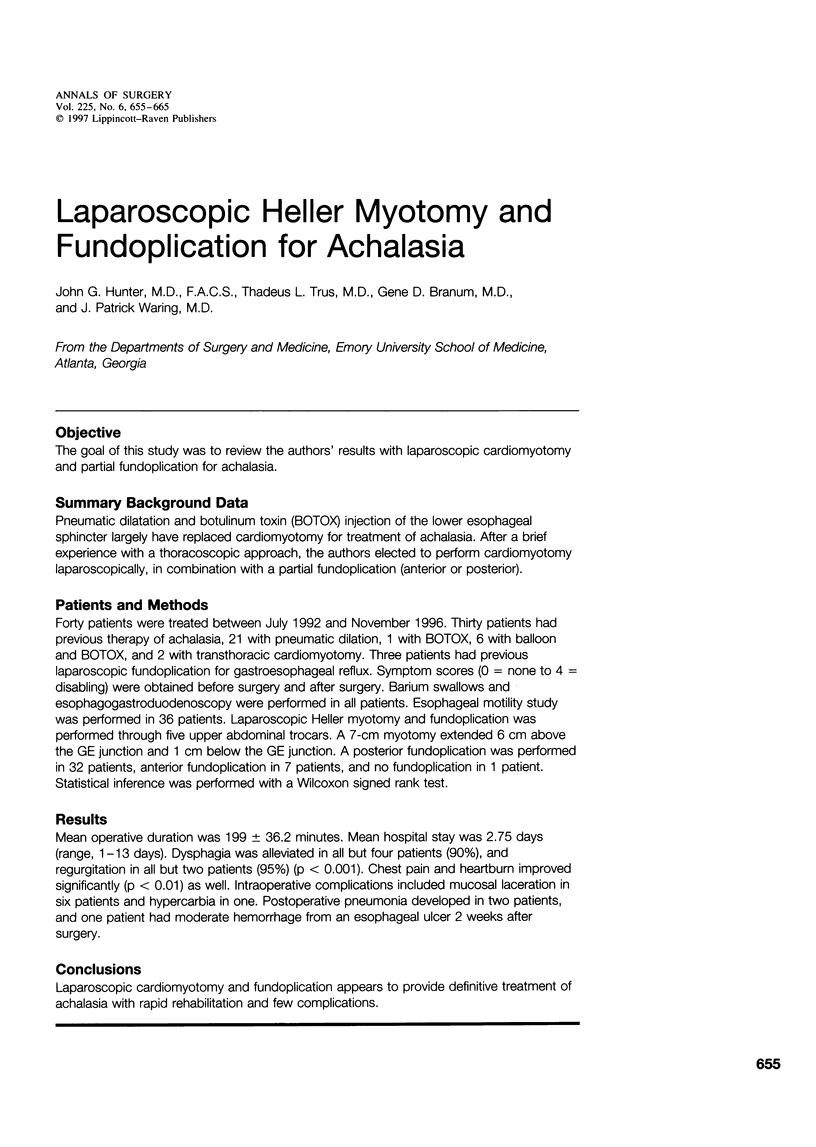


Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Abid S., Champion G., Richter J. E., McElvein R., Slaughter R. L., Koehler R. E. Treatment of achalasia: the best of both worlds. Am J Gastroenterol. 1994 Jul;89(7):979–985. [PubMed] [Google Scholar]
- Allen K. B., Ricketts R. R. Surgery for achalasia of the cardia in children: the Dor-Gavriliu procedure. J Pediatr Surg. 1992 Nov;27(11):1418–1421. doi: 10.1016/0022-3468(92)90190-i. [DOI] [PubMed] [Google Scholar]
- Ancona E., Anselmino M., Zaninotto G., Costantini M., Rossi M., Bonavina L., Boccu C., Buin F., Peracchia A. Esophageal achalasia: laparoscopic versus conventional open Heller-Dor operation. Am J Surg. 1995 Sep;170(3):265–270. doi: 10.1016/s0002-9610(05)80012-1. [DOI] [PubMed] [Google Scholar]
- Andreollo N. A., Earlam R. J. Heller's myotomy for achalasia: is an added anti-reflux procedure necessary? Br J Surg. 1987 Sep;74(9):765–769. doi: 10.1002/bjs.1800740903. [DOI] [PubMed] [Google Scholar]
- Bonavina L., Nosadini A., Bardini R., Baessato M., Peracchia A. Primary treatment of esophageal achalasia. Long-term results of myotomy and Dor fundoplication. Arch Surg. 1992 Feb;127(2):222–227. doi: 10.1001/archsurg.1992.01420020112016. [DOI] [PubMed] [Google Scholar]
- Csendes A., Braghetto I., Henríquez A., Cortés C. Late results of a prospective randomised study comparing forceful dilatation and oesophagomyotomy in patients with achalasia. Gut. 1989 Mar;30(3):299–304. doi: 10.1136/gut.30.3.299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellingson T. L., Kozarek R. A., Gelfand M. D., Botoman A. V., Patterson D. J. Iatrogenic achalasia. A case series. J Clin Gastroenterol. 1995 Mar;20(2):96–99. doi: 10.1097/00004836-199503000-00004. [DOI] [PubMed] [Google Scholar]
- Ferguson M. K. Achalasia: current evaluation and therapy. Ann Thorac Surg. 1991 Aug;52(2):336–342. doi: 10.1016/0003-4975(91)91373-4. [DOI] [PubMed] [Google Scholar]
- Parkman H. P., Reynolds J. C., Ouyang A., Rosato E. F., Eisenberg J. M., Cohen S. Pneumatic dilatation or esophagomyotomy treatment for idiopathic achalasia: clinical outcomes and cost analysis. Dig Dis Sci. 1993 Jan;38(1):75–85. doi: 10.1007/BF01296777. [DOI] [PubMed] [Google Scholar]
- Parrilla Paricio P., Martínez de Haro L., Ortiz A., Aguayo J. L. Achalasia of the cardia: long-term results of oesophagomyotomy and posterior partial fundoplication. Br J Surg. 1990 Dec;77(12):1371–1374. doi: 10.1002/bjs.1800771217. [DOI] [PubMed] [Google Scholar]
- Pasricha P. J., Rai R., Ravich W. J., Hendrix T. R., Kalloo A. N. Botulinum toxin for achalasia: long-term outcome and predictors of response. Gastroenterology. 1996 May;110(5):1410–1415. doi: 10.1053/gast.1996.v110.pm8613045. [DOI] [PubMed] [Google Scholar]
- Pellegrini C. A. Impact and evolution of minimally invasive techniques in the treatment of achalasia. Surg Endosc. 1997 Jan;11(1):1–2. doi: 10.1007/s004649900282. [DOI] [PubMed] [Google Scholar]
- Pellegrini C. A., Leichter R., Patti M., Somberg K., Ostroff J. W., Way L. Thoracoscopic esophageal myotomy in the treatment of achalasia. Ann Thorac Surg. 1993 Sep;56(3):680–682. doi: 10.1016/0003-4975(93)90950-m. [DOI] [PubMed] [Google Scholar]
- Pellegrini C., Wetter L. A., Patti M., Leichter R., Mussan G., Mori T., Bernstein G., Way L. Thoracoscopic esophagomyotomy. Initial experience with a new approach for the treatment of achalasia. Ann Surg. 1992 Sep;216(3):291–299. doi: 10.1097/00000658-199209000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Richter J. E. Surgery or pneumatic dilatation for achalasia: a head-to-head comparison. Now are all the questions answered? Gastroenterology. 1989 Nov;97(5):1340–1341. doi: 10.1016/0016-5085(89)91711-3. [DOI] [PubMed] [Google Scholar]
- Sauer L., Pellegrini C. A., Way L. W. The treatment of achalasia. A current perspective. Arch Surg. 1989 Aug;124(8):929–932. doi: 10.1001/archsurg.1989.01410080061009. [DOI] [PubMed] [Google Scholar]
- Shimi S., Nathanson L. K., Cuschieri A. Laparoscopic cardiomyotomy for achalasia. J R Coll Surg Edinb. 1991 Jun;36(3):152–154. [PubMed] [Google Scholar]
- Swanstrom L. L., Pennings J. Laparoscopic esophagomyotomy for achalasia. Surg Endosc. 1995 Mar;9(3):286–292. doi: 10.1007/BF00187770. [DOI] [PubMed] [Google Scholar]
- Wehrmann T., Jacobi V., Jung M., Lembcke B., Caspary W. F. Pneumatic dilation in achalasia with a low-compliance balloon: results of a 5-year prospective evaluation. Gastrointest Endosc. 1995 Jul;42(1):31–36. doi: 10.1016/s0016-5107(95)70239-3. [DOI] [PubMed] [Google Scholar]