

Abstract
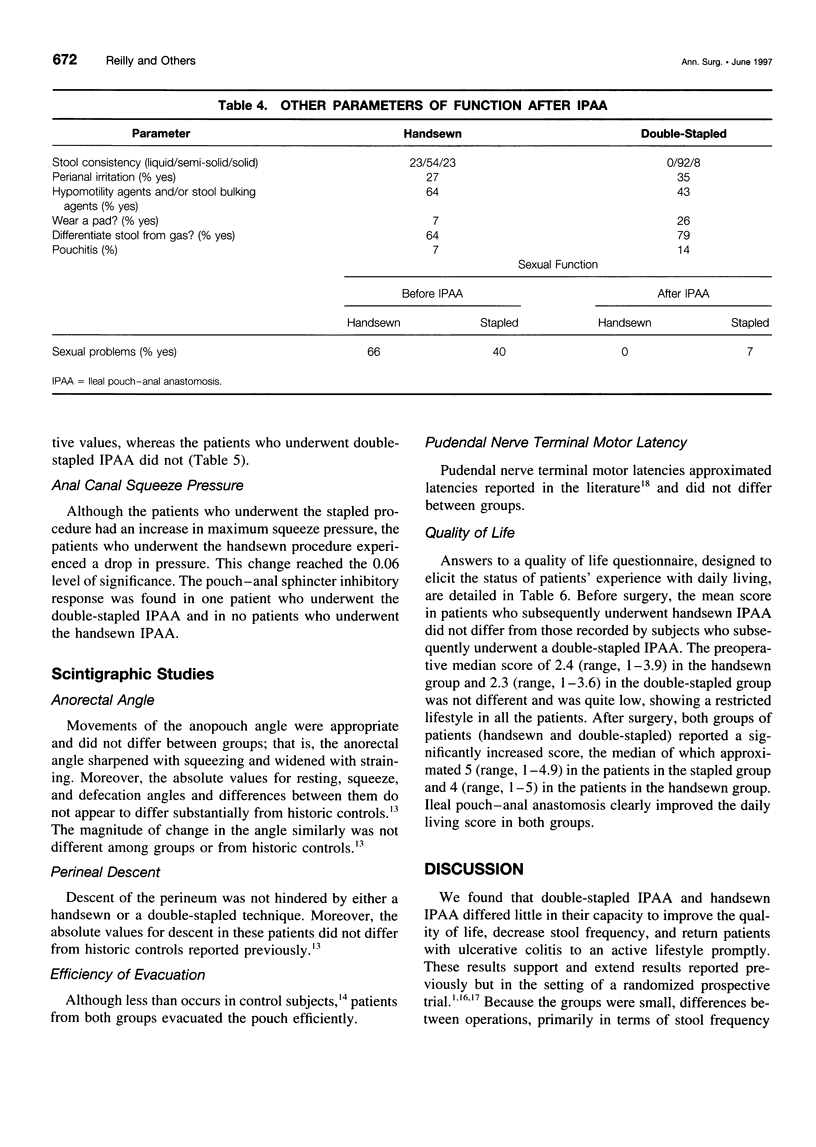
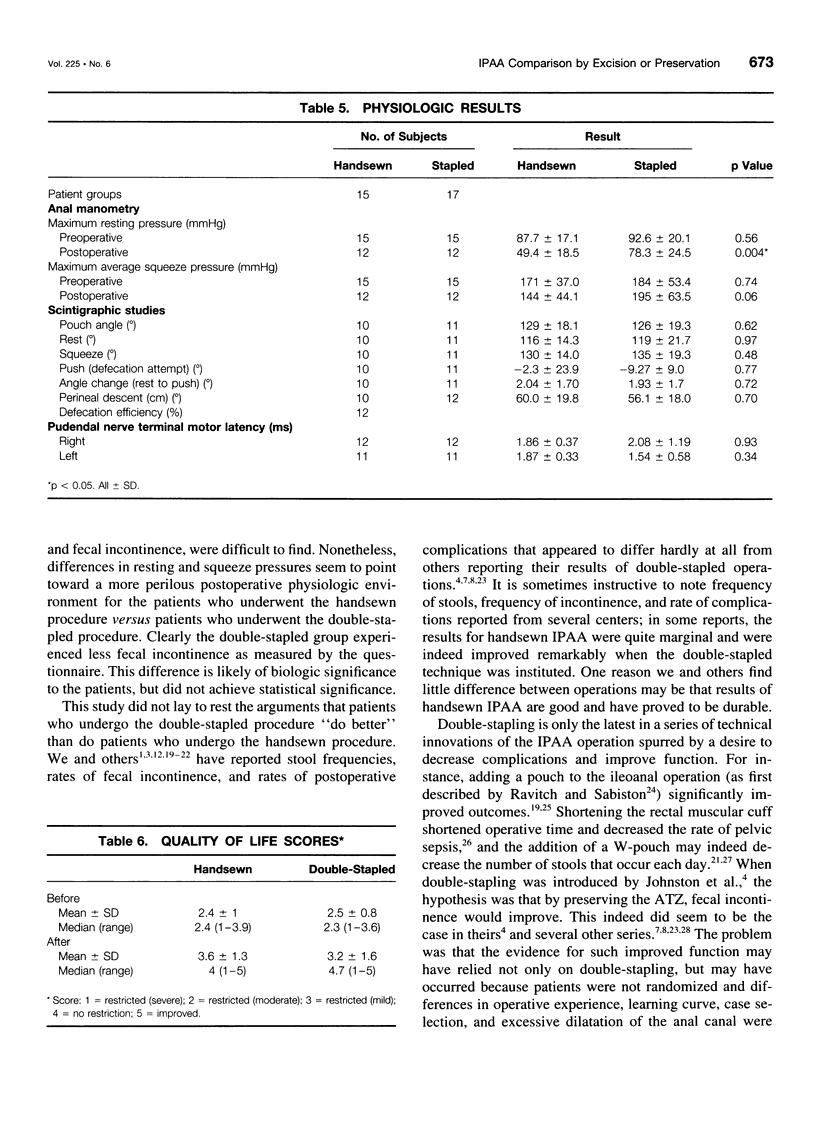
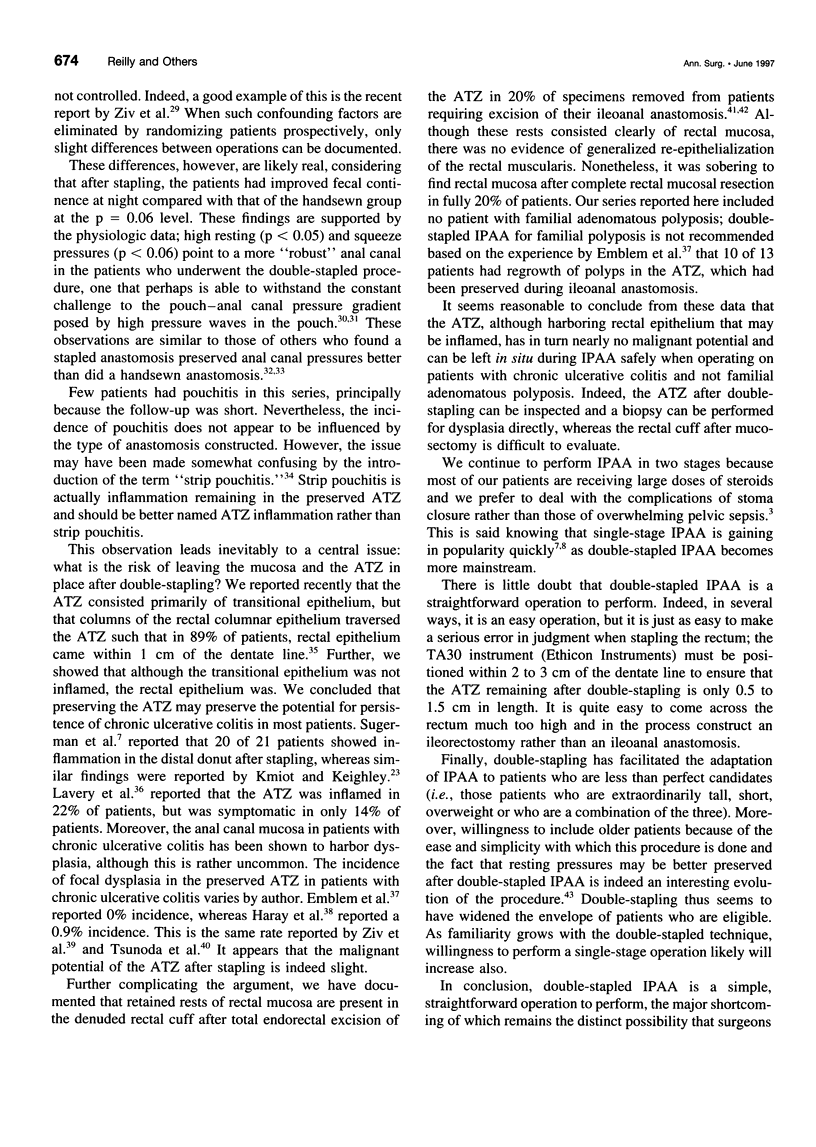
OBJECTIVE: The purpose of the study is to compare the results of ileal pouch-anal anastomosis (IPAA) in patients in whom the anal mucosa is excised by handsewn techniques to those in whom the mucosa is preserved using stapling techniques. SUMMARY BACKGROUND DATA: Ileal pouch-anal anastomosis is the operation of choice for patients with chronic ulcerative colitis requiring proctocolectomy. Controversy exists over whether preserving the transitional mucosa of the anal canal improves outcomes. METHODS: Forty-one patients (23 men, 18 women) were randomized to either endorectal mucosectomy and handsewn IPAA or to double-stapled IPAA, which spared the anal transition zone. All patients were diverted for 2 to 3 months. Nine patients were excluded. Preoperative functional status was assessed by questionnaire and anal manometry. Twenty-four patients underwent more extensive physiologic evaluation, including scintigraphic anopouch angle studies and pudendel never terminal motor latency a mean of 6 months after surgery. Quality of life similarly was estimated before surgery and after surgery. Univariate analysis using Wilcoxon test was used to assess differences between groups. RESULTS: The two groups were identical demographically. Overall outcomes in both groups were good. Thirty-three percent of patients who underwent the handsewn technique and 35% of patients who underwent the double-stapled technique experienced a postoperative complication. Resting anal canal pressures were higher in the patients who underwent the stapled technique, but other physiologic parameters were similar between groups. Night-time fecal incontinence occurred less frequently in the stapled group but not significantly. The number of stools per 24 hours decreased from preoperative values in both groups. After IPAA, quality of life improved promptly in both groups. CONCLUSIONS: Stapled IPAA, which preserves the mucosa of the anal transition zone, confers no apparent early advantage in terms of decreased stool frequency or fewer episodes of fecal incontinence compared to handsewn IPAA, which excises the mucosa. Higher resting pressures in the stapled group coupled with a trend toward less night-time incontinence, however, may portend better function in the stapled group over time. Both operations are safe and result in rapid and profound improvement in quality of life.
Full text
PDF




Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ambroze W. L., Jr, Pemberton J. H., Dozois R. R., Carpenter H. A., O'Rourke J. S., Ilstrup D. M. The histological pattern and pathological involvement of the anal transition zone in patients with ulcerative colitis. Gastroenterology. 1993 Feb;104(2):514–518. doi: 10.1016/0016-5085(93)90421-8. [DOI] [PubMed] [Google Scholar]
- Barkel D. C., Pemberton J. H., Pezim M. E., Phillips S. F., Kelly K. A., Brown M. L. Scintigraphic assessment of the anorectal angle in health and after ileal pouch-anal anastomosis. Ann Surg. 1988 Jul;208(1):42–49. doi: 10.1097/00000658-198807000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beart R. W., Jr, Dozois R. R., Wolff B. G., Pemberton J. H. Mechanisms of rectal continence. Lessons from the ileoanal procedure. Am J Surg. 1985 Jan;149(1):31–34. doi: 10.1016/s0002-9610(85)80005-2. [DOI] [PubMed] [Google Scholar]
- Becker J. M., Raymond J. L. Ileal pouch-anal anastomosis. A single surgeon's experience with 100 consecutive cases. Ann Surg. 1986 Oct;204(4):375–383. doi: 10.1097/00000658-198610000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Choen S., Tsunoda A., Nicholls R. J. Prospective randomized trial comparing anal function after hand sewn ileoanal anastomosis with mucosectomy versus stapled ileoanal anastomosis without mucosectomy in restorative proctocolectomy. Br J Surg. 1991 Apr;78(4):430–434. doi: 10.1002/bjs.1800780415. [DOI] [PubMed] [Google Scholar]
- DUTHIE H. L., GAIRNS F. W. Sensory nerve-endings and sensation in the anal region of man. Br J Surg. 1960 May;47:585–595. doi: 10.1002/bjs.18004720602. [DOI] [PubMed] [Google Scholar]
- Emblem R., Bergan A., Larsen S. Straight ileoanal anastomosis with preserved anal mucosa for ulcerative colitis and familial polyposis. Scand J Gastroenterol. 1988 Oct;23(8):913–919. doi: 10.3109/00365528809090146. [DOI] [PubMed] [Google Scholar]
- Ferrara A., Pemberton J. H., Grotz R. L., Hanson R. B. Motor determinants of incontinence after ileal pouch-anal anastomosis. Br J Surg. 1994 Feb;81(2):285–288. doi: 10.1002/bjs.1800810245. [DOI] [PubMed] [Google Scholar]
- Ferrara A., Pemberton J. H., Hanson R. B. Preservation of continence after ileoanal anastomosis by the coordination of ileal pouch and anal canal motor activity. Am J Surg. 1992 Jan;163(1):83–89. doi: 10.1016/0002-9610(92)90257-r. [DOI] [PubMed] [Google Scholar]
- Gemlo B. T., Belmonte C., Wiltz O., Madoff R. D. Functional assessment of ileal pouch-anal anastomotic techniques. Am J Surg. 1995 Jan;169(1):137–142. doi: 10.1016/s0002-9610(99)80122-6. [DOI] [PubMed] [Google Scholar]
- Haray P. N., Amarnath B., Weiss E. G., Nogueras J. J., Wexner S. D. Low malignant potential of the double-stapled ileal pouch-anal anastomosis. Br J Surg. 1996 Oct;83(10):1406–1406. doi: 10.1002/bjs.1800831026. [DOI] [PubMed] [Google Scholar]
- Harms B. A., Pellett J. R., Starling J. R. Modified quadruple-loop (W) ileal reservoir for restorative proctocolectomy. Surgery. 1987 Feb;101(2):234–237. [PubMed] [Google Scholar]
- Heald R. J., Allen D. R. Stapled ileo-anal anastomosis: a technique to avoid mucosal proctectomy in the ileal pouch operation. Br J Surg. 1986 Jul;73(7):571–572. doi: 10.1002/bjs.1800730719. [DOI] [PubMed] [Google Scholar]
- Heppell J., Weiland L. H., Perrault J., Pemberton J. H., Telander R. L., Beart R. W., Jr Fate of the rectal mucosa after rectal mucosectomy and ileoanal anastomosis. Dis Colon Rectum. 1983 Dec;26(12):768–771. doi: 10.1007/BF02554744. [DOI] [PubMed] [Google Scholar]
- Johnston D., Holdsworth P. J., Nasmyth D. G., Neal D. E., Primrose J. N., Womack N., Axon A. T. Preservation of the entire anal canal in conservative proctocolectomy for ulcerative colitis: a pilot study comparing end-to-end ileo-anal anastomosis without mucosal resection with mucosal proctectomy and endo-anal anastomosis. Br J Surg. 1987 Oct;74(10):940–944. doi: 10.1002/bjs.1800741020. [DOI] [PubMed] [Google Scholar]
- Kelly K. A., Pemberton J. H., Wolff B. G., Dozois R. R. Ileal pouch-anal anastomosis. Curr Probl Surg. 1992 Feb;29(2):57–131. doi: 10.1016/0011-3840(92)90012-r. [DOI] [PubMed] [Google Scholar]
- Kiff E. S., Swash M. Slowed conduction in the pudendal nerves in idiopathic (neurogenic) faecal incontinence. Br J Surg. 1984 Aug;71(8):614–616. doi: 10.1002/bjs.1800710817. [DOI] [PubMed] [Google Scholar]
- Kmiot W. A., Keighley M. R. Totally stapled abdominal restorative proctocolectomy. Br J Surg. 1989 Sep;76(9):961–964. doi: 10.1002/bjs.1800760931. [DOI] [PubMed] [Google Scholar]
- Köhler L. W., Pemberton J. H., Zinsmeister A. R., Kelly K. A. Quality of life after proctocolectomy. A comparison of Brooke ileostomy, Kock pouch, and ileal pouch-anal anastomosis. Gastroenterology. 1991 Sep;101(3):679–684. [PubMed] [Google Scholar]
- Lavery I. C., Sirimarco M. T., Ziv Y., Fazio V. W. Anal canal inflammation after ileal pouch-anal anastomosis. The need for treatment. Dis Colon Rectum. 1995 Aug;38(8):803–806. doi: 10.1007/BF02049836. [DOI] [PubMed] [Google Scholar]
- Luukkonen P., Järvinen H. Stapled vs hand-sutured ileoanal anastomosis in restorative proctocolectomy. A prospective, randomized study. Arch Surg. 1993 Apr;128(4):437–440. doi: 10.1001/archsurg.1993.01420160075012. [DOI] [PubMed] [Google Scholar]
- McGregor B., Colon S., Mutin M., Chignier E., Zech P., McGregor J. Thrombospondin in human glomerulopathies. A marker of inflammation and early fibrosis. Am J Pathol. 1994 Jun;144(6):1281–1287. [PMC free article] [PubMed] [Google Scholar]
- McIntyre P. B., Pemberton J. H., Beart R. W., Jr, Devine R. M., Nivatvongs S. Double-stapled vs. handsewn ileal pouch-anal anastomosis in patients with chronic ulcerative colitis. Dis Colon Rectum. 1994 May;37(5):430–433. doi: 10.1007/BF02076186. [DOI] [PubMed] [Google Scholar]
- Nicholls R. J., Pezim M. E. Restorative proctocolectomy with ileal reservoir for ulcerative colitis and familial adenomatous polyposis: a comparison of three reservoir designs. Br J Surg. 1985 Jun;72(6):470–474. doi: 10.1002/bjs.1800720622. [DOI] [PubMed] [Google Scholar]
- O'Connell P. R., Kelly K. A., Brown M. L. Scintigraphic assessment of neorectal motor function. J Nucl Med. 1986 Apr;27(4):460–464. [PubMed] [Google Scholar]
- O'Connell P. R., Pemberton J. H., Weiland L. H., Beart R. W., Jr, Dozois R. R., Wolff B. G., Telander R. L. Does rectal mucosa regenerate after ileoanal anastomosis? Dis Colon Rectum. 1987 Jan;30(1):1–5. doi: 10.1007/BF02556908. [DOI] [PubMed] [Google Scholar]
- Pemberton J. H., Kelly K. A., Beart R. W., Jr, Dozois R. R., Wolff B. G., Ilstrup D. M. Ileal pouch-anal anastomosis for chronic ulcerative colitis. Long-term results. Ann Surg. 1987 Oct;206(4):504–513. doi: 10.1097/00000658-198710000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pemberton J. H., Phillips S. F., Ready R. R., Zinsmeister A. R., Beahrs O. H. Quality of life after Brooke ileostomy and ileal pouch-anal anastomosis. Comparison of performance status. Ann Surg. 1989 May;209(5):620–628. doi: 10.1097/00000658-198905000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pemberton J. H. Surgery for ulcerative colitis. Surg Clin North Am. 1987 Jun;67(3):633–650. doi: 10.1016/s0039-6109(16)44236-2. [DOI] [PubMed] [Google Scholar]
- Rauh S. M., Schoetz D. J., Jr, Roberts P. L., Murray J. J., Coller J. A., Veidenheimer M. C. Pouchitis--is it a wastebasket diagnosis? Dis Colon Rectum. 1991 Aug;34(8):685–689. doi: 10.1007/BF02050351. [DOI] [PubMed] [Google Scholar]
- Reissman P., Piccirillo M., Ulrich A., Daniel N., Nogueras J. J., Wexner S. D. Functional results of the double-stapled ileoanal reservoir. J Am Coll Surg. 1995 Nov;181(5):444–450. [PubMed] [Google Scholar]
- Reissman P., Teoh T. A., Weiss E. G., Nogueras J. J., Wexner S. D. Functional outcome of the double stapled ileoanal reservoir in patients more than 60 years of age. Am Surg. 1996 Mar;62(3):178–183. [PubMed] [Google Scholar]
- Sagar P. M., Holdsworth P. J., Johnston D. Correlation between laboratory findings and clinical outcome after restorative proctocolectomy: serial studies in 20 patients with end-to-end pouch-anal anastomosis. Br J Surg. 1991 Jan;78(1):67–70. doi: 10.1002/bjs.1800780121. [DOI] [PubMed] [Google Scholar]
- Sugerman H. J., Newsome H. H., Decosta G., Zfass A. M. Stapled ileoanal anastomosis for ulcerative colitis and familial polyposis without a temporary diverting ileostomy. Ann Surg. 1991 Jun;213(6):606–619. doi: 10.1097/00000658-199106000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sugerman H. J., Newsome H. H. Stapled ileoanal anastomosis without a temporary ileostomy. Am J Surg. 1994 Jan;167(1):58–66. doi: 10.1016/0002-9610(94)90054-x. [DOI] [PubMed] [Google Scholar]
- Taylor B. M., Beart R. W., Jr, Dozois R. R., Kelly K. A., Phillips S. F. Straight ileoanal anastomosis v ileal pouch--anal anastomosis after colectomy and mucosal proctectomy. Arch Surg. 1983 Jun;118(6):696–701. doi: 10.1001/archsurg.1983.01390060018004. [DOI] [PubMed] [Google Scholar]
- Tsunoda A., Talbot I. C., Nicholls R. J. Incidence of dysplasia in the anorectal mucosa in patients having restorative proctocolectomy. Br J Surg. 1990 May;77(5):506–508. doi: 10.1002/bjs.1800770510. [DOI] [PubMed] [Google Scholar]
- Tuckson W., Lavery I., Fazio V., Oakley J., Church J., Milsom J. Manometric and functional comparison of ileal pouch anal anastomosis with and without anal manipulation. Am J Surg. 1991 Jan;161(1):90–96. doi: 10.1016/0002-9610(91)90366-l. [DOI] [PubMed] [Google Scholar]
- Utsunomiya J., Iwama T., Imajo M., Matsuo S., Sawai S., Yaegashi K., Hirayama R. Total colectomy, mucosal proctectomy, and ileoanal anastomosis. Dis Colon Rectum. 1980 Oct;23(7):459–466. doi: 10.1007/BF02987076. [DOI] [PubMed] [Google Scholar]
- Williams N. S. Restorative proctocolectomy is the first choice elective surgical treatment for ulcerative colitis. Br J Surg. 1989 Nov;76(11):1109–1110. doi: 10.1002/bjs.1800761103. [DOI] [PubMed] [Google Scholar]
- Ziv Y., Fazio V. W., Church J. M., Lavery I. C., King T. M., Ambrosetti P. Stapled ileal pouch anal anastomoses are safer than handsewn anastomoses in patients with ulcerative colitis. Am J Surg. 1996 Mar;171(3):320–323. doi: 10.1016/S0002-9610(97)89634-1. [DOI] [PubMed] [Google Scholar]