

Abstract
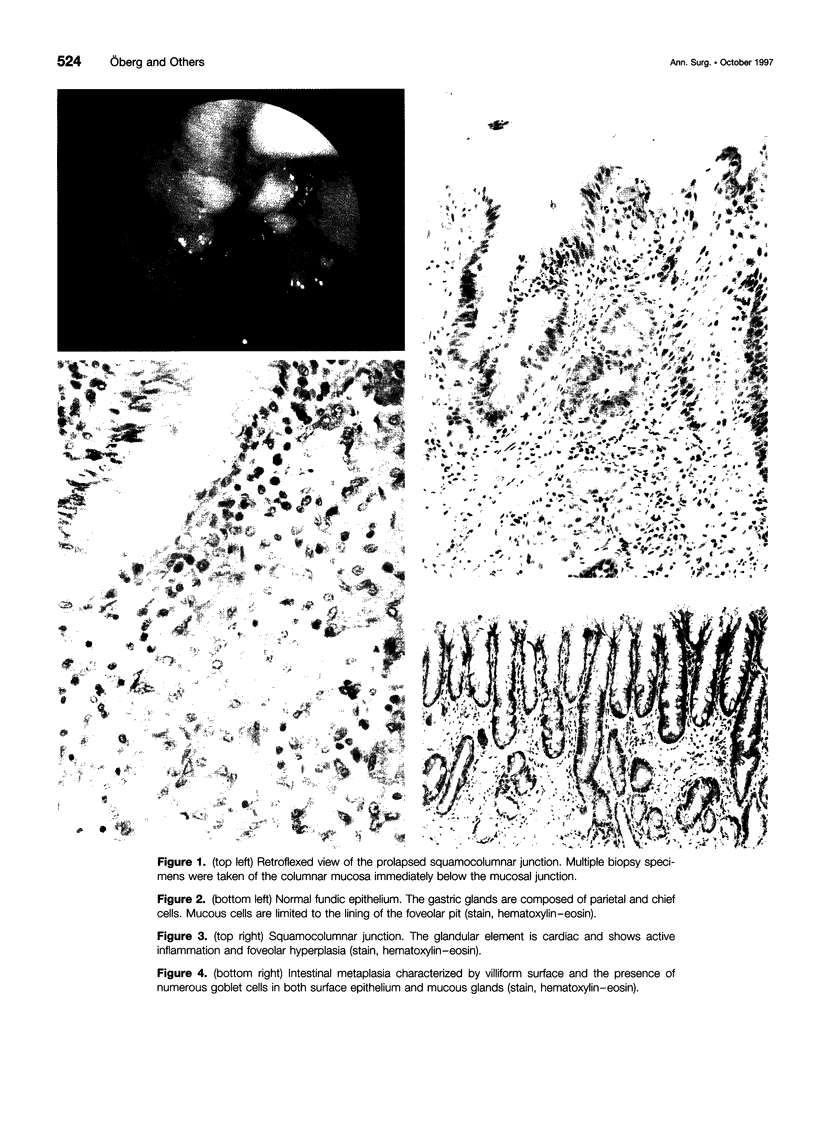
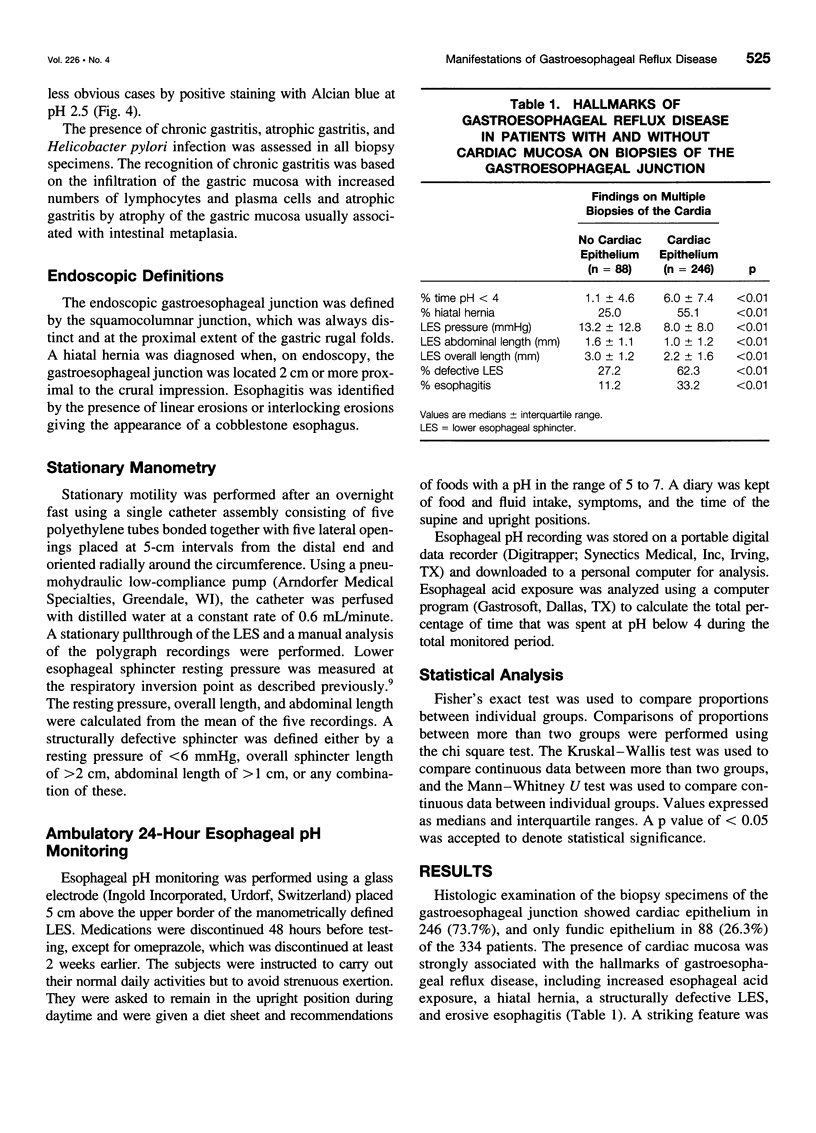
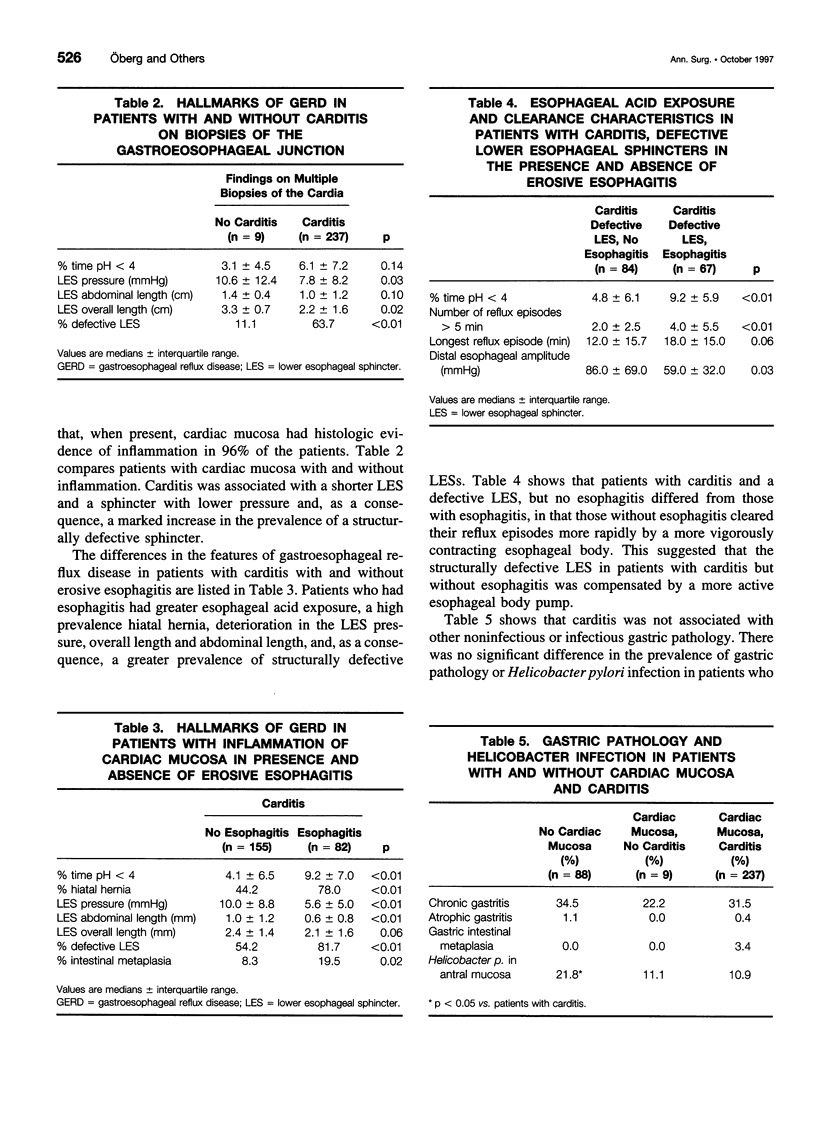
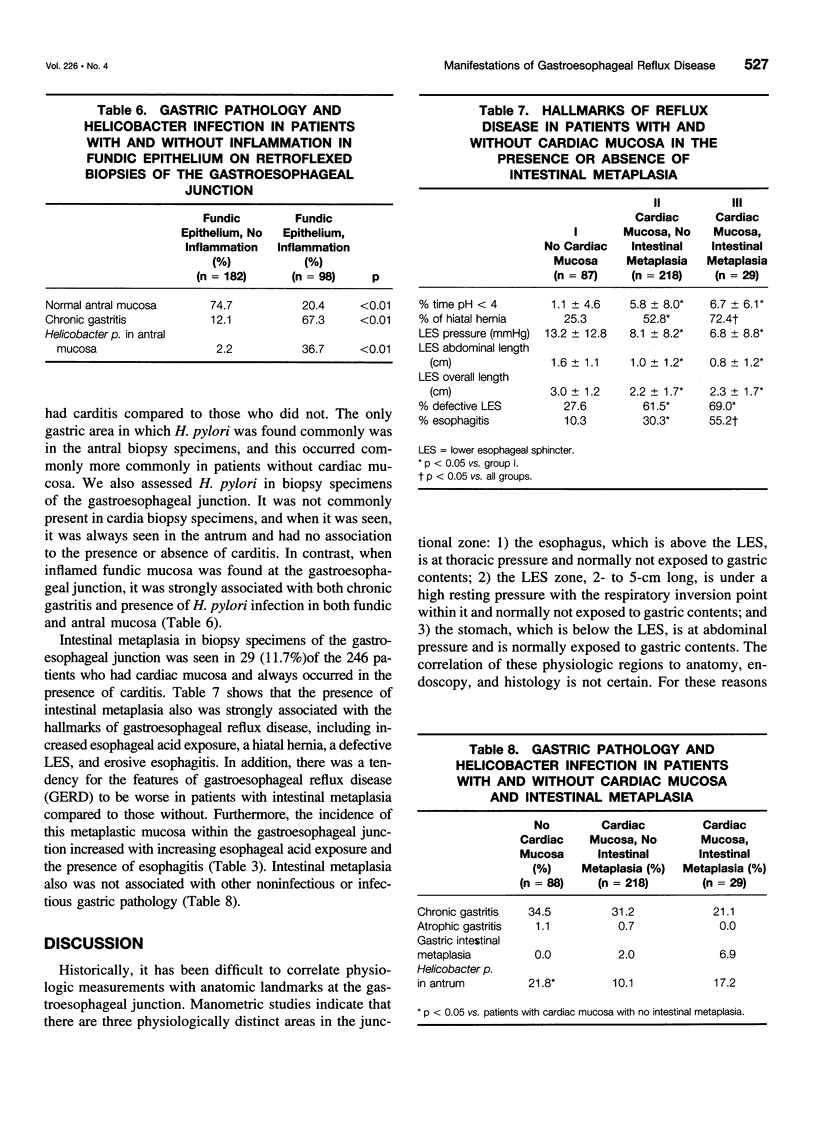
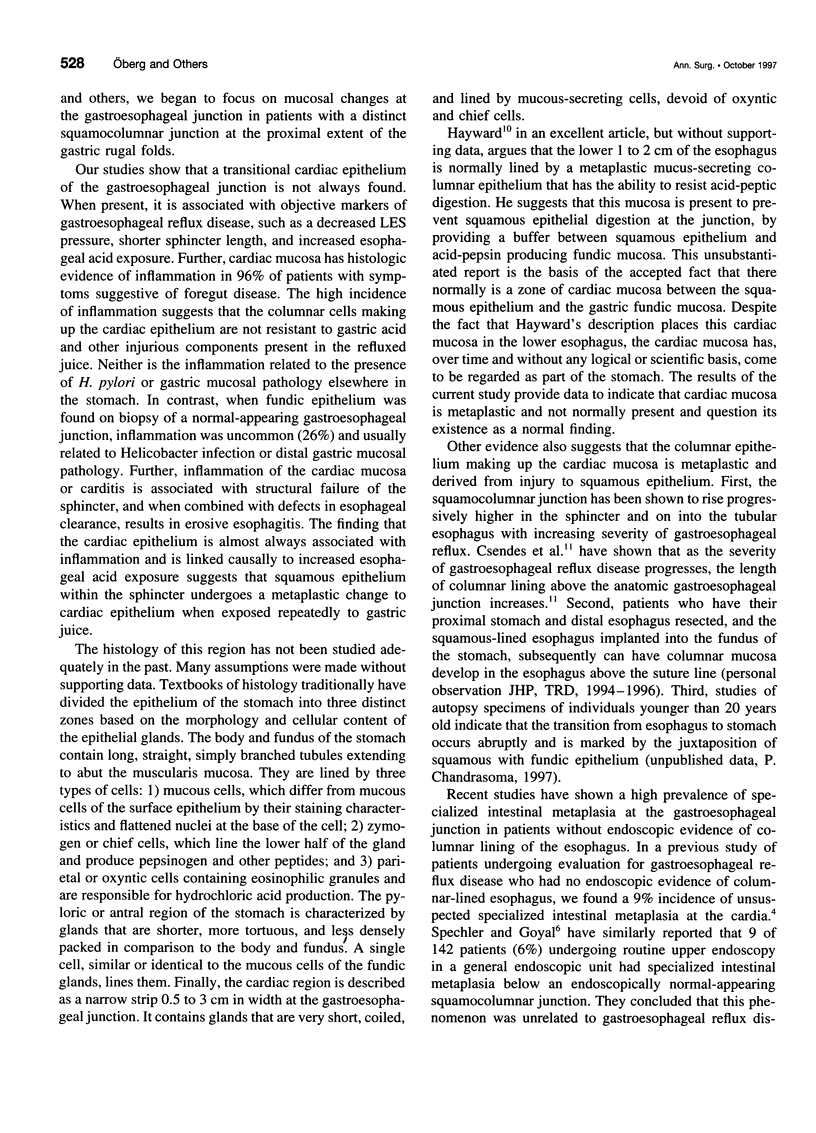
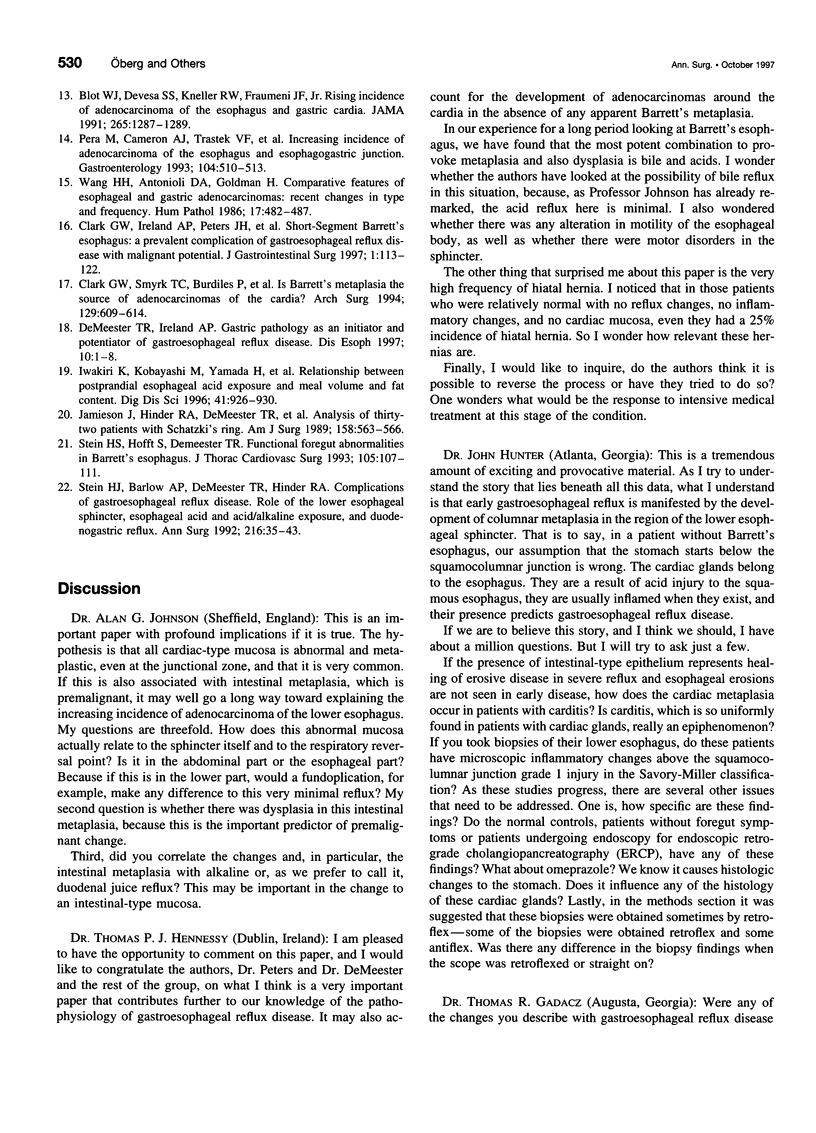
OBJECTIVE: The purpose of the study was to test the hypothesis that cardiac mucosa, carditis, and specialized intestinal metaplasia at an endoscopically normal-appearing cardia are manifestations of gastroesophageal reflux disease. SUMMARY BACKGROUND DATA: In the absence of esophageal mucosal injury, the diagnosis of gastroesophageal reflux disease currently rests on 24-hour pH monitoring. Histologic examination of the esophagus is not useful. The recent identification of specialized intestinal metaplasia at the cardia, along with the observation that it occurs in inflamed cardiac mucosa, led the authors to focus on the type and condition of the mucosa at the gastroesophageal junction and its relation to gastroesophageal reflux disease. METHODS: Three hundred thirty-four consecutive patients with symptoms of foregut disease, no evidence of columnar-lined esophagus, and no history of gastric or esophageal surgery were evaluated by 1) endoscopic biopsies above, at, and below the gastroesophageal junction; 2) esophageal motility; and 3) 24-hour esophageal pH monitoring. The patients were divided into groups depending on the histologic presence of cardiac epithelium with and without inflammation or associated intestinal metaplasia. Markers of gastroesophageal reflux disease were compared between groups (i.e., lower esophageal sphincter characteristics, esophageal acid exposure, the presence of endoscopic erosive esophagitis, and hiatal hernia). RESULTS: When cardiac epithelium was found, it was inflamed in 96% of the patients. The presence of cardiac epithelium and carditis was associated with deterioration of lower esophageal sphincter characteristics and increased esophageal acid exposure. Esophagitis occurred more commonly in patients with carditis whose sphincter, on manometry, was structurally defective. Specialized intestinal metaplasia at the cardia was only seen in inflamed cardiac mucosa, and its prevalence increased both with increasing acid exposure and with the presence of esophagitis. CONCLUSION: The findings of cardiac mucosa, carditis, and intestinal metaplasia in an endoscopically normal-appearing gastroesophageal junction are histologic indicators of gastroesophageal reflux disease. These findings may be among the earliest signs of gastroesophageal reflux and contribute to the authors understanding of the pathophysiology of the disease process.
Full text
PDF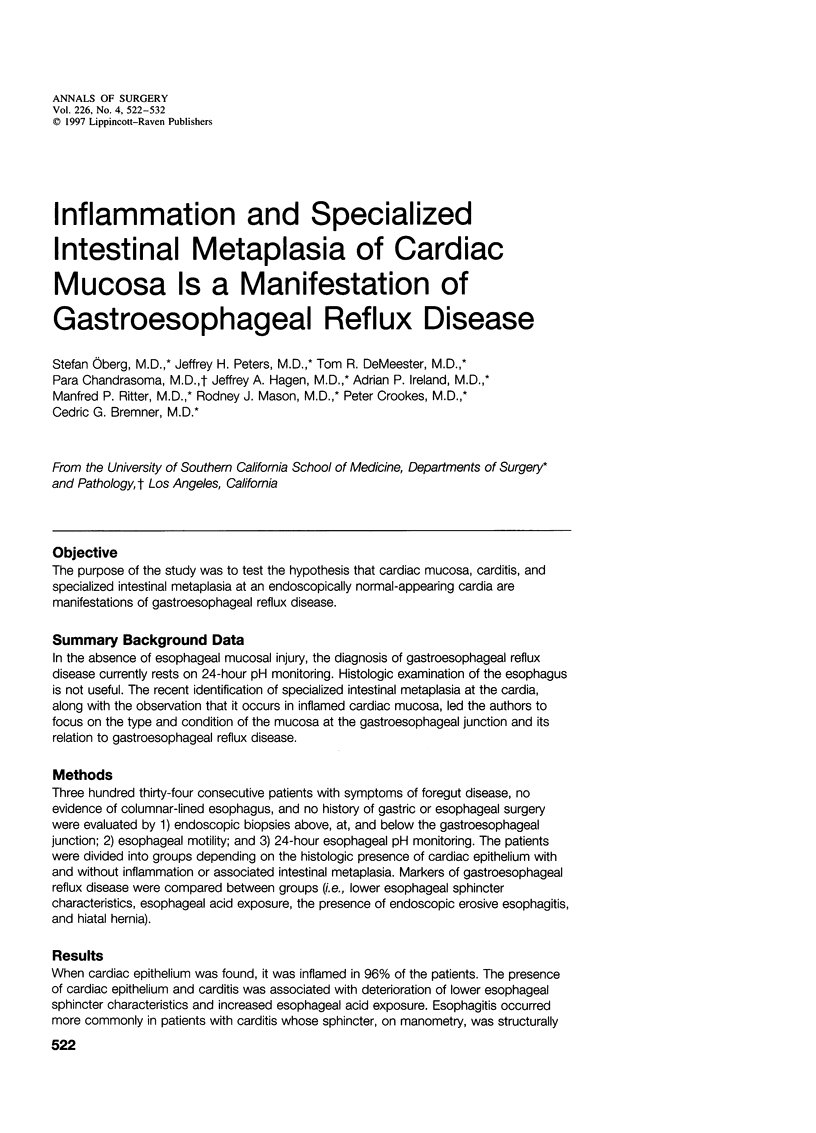


Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Blot W. J., Devesa S. S., Kneller R. W., Fraumeni J. F., Jr Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA. 1991 Mar 13;265(10):1287–1289. [PubMed] [Google Scholar]
- Clark G. W., Ireland A. P., Peters J. H., Chandrasoma P., DeMeester T. R., Bremner C. G. Short-segment Barrett's esophagus: A prevalent complication of gastroesophageal reflux disease with malignant potential. J Gastrointest Surg. 1997 Mar-Apr;1(2):113–122. doi: 10.1016/s1091-255x(97)80098-4. [DOI] [PubMed] [Google Scholar]
- Clark G. W., Smyrk T. C., Burdiles P., Hoeft S. F., Peters J. H., Kiyabu M., Hinder R. A., Bremner C. G., DeMeester T. R. Is Barrett's metaplasia the source of adenocarcinomas of the cardia? Arch Surg. 1994 Jun;129(6):609–614. doi: 10.1001/archsurg.1994.01420300051007. [DOI] [PubMed] [Google Scholar]
- Csendes A., Maluenda F., Braghetto I., Csendes P., Henriquez A., Quesada M. S. Location of the lower oesophageal sphincter and the squamous columnar mucosal junction in 109 healthy controls and 778 patients with different degrees of endoscopic oesophagitis. Gut. 1993 Jan;34(1):21–27. doi: 10.1136/gut.34.1.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeMeester T. R., Ireland A. P. Gastric pathology as an initiator and potentiator of gastroesophageal reflux disease. Dis Esophagus. 1997 Jan;10(1):1–8. doi: 10.1093/dote/10.1.1. [DOI] [PubMed] [Google Scholar]
- HAYWARD J. The lower end of the oesophagus. Thorax. 1961 Mar;16:36–41. doi: 10.1136/thx.16.1.36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Howard P. J., Heading R. C. Epidemiology of gastro-esophageal reflux disease. World J Surg. 1992 Mar-Apr;16(2):288–293. doi: 10.1007/BF02071535. [DOI] [PubMed] [Google Scholar]
- Iwakiri K., Kobayashi M., Kotoyori M., Yamada H., Sugiura T., Nakagawa Y. Relationship between postprandial esophageal acid exposure and meal volume and fat content. Dig Dis Sci. 1996 May;41(5):926–930. doi: 10.1007/BF02091532. [DOI] [PubMed] [Google Scholar]
- Jamieson J. R., Stein H. J., DeMeester T. R., Bonavina L., Schwizer W., Hinder R. A., Albertucci M. Ambulatory 24-h esophageal pH monitoring: normal values, optimal thresholds, specificity, sensitivity, and reproducibility. Am J Gastroenterol. 1992 Sep;87(9):1102–1111. [PubMed] [Google Scholar]
- Jamieson J., Hinder R. A., DeMeester T. R., Litchfield D., Barlow A., Bailey R. T., Jr Analysis of thirty-two patients with Schatzki's ring. Am J Surg. 1989 Dec;158(6):563–566. doi: 10.1016/0002-9610(89)90193-1. [DOI] [PubMed] [Google Scholar]
- Morales T. G., Sampliner R. E., Bhattacharyya A. Intestinal metaplasia of the gastric cardia. Am J Gastroenterol. 1997 Mar;92(3):414–418. [PubMed] [Google Scholar]
- Pera M., Cameron A. J., Trastek V. F., Carpenter H. A., Zinsmeister A. R. Increasing incidence of adenocarcinoma of the esophagus and esophagogastric junction. Gastroenterology. 1993 Feb;104(2):510–513. doi: 10.1016/0016-5085(93)90420-h. [DOI] [PubMed] [Google Scholar]
- Schindlbeck N. E., Wiebecke B., Klauser A. G., Voderholzer W. A., Müller-Lissner S. A. Diagnostic value of histology in non-erosive gastro-oesophageal reflux disease. Gut. 1996 Aug;39(2):151–154. doi: 10.1136/gut.39.2.151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spechler S. J., Goyal R. K. Barrett's esophagus. N Engl J Med. 1986 Aug 7;315(6):362–371. doi: 10.1056/NEJM198608073150605. [DOI] [PubMed] [Google Scholar]
- Stein H. J., Barlow A. P., DeMeester T. R., Hinder R. A. Complications of gastroesophageal reflux disease. Role of the lower esophageal sphincter, esophageal acid and acid/alkaline exposure, and duodenogastric reflux. Ann Surg. 1992 Jul;216(1):35–43. doi: 10.1097/00000658-199207000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stein H. J., Hoeft S., DeMeester T. R. Functional foregut abnormalities in Barrett's esophagus. J Thorac Cardiovasc Surg. 1993 Jan;105(1):107–111. [PubMed] [Google Scholar]
- Wang H. H., Antonioli D. A., Goldman H. Comparative features of esophageal and gastric adenocarcinomas: recent changes in type and frequency. Hum Pathol. 1986 May;17(5):482–487. doi: 10.1016/s0046-8177(86)80038-7. [DOI] [PubMed] [Google Scholar]
- Weston A. P., Krmpotich P. T., Cherian R., Dixon A., Topalovski M. Prospective evaluation of intestinal metaplasia and dysplasia within the cardia of patients with Barrett's esophagus. Dig Dis Sci. 1997 Mar;42(3):597–602. doi: 10.1023/a:1018811512939. [DOI] [PubMed] [Google Scholar]
- Weston A. P., Krmpotich P., Makdisi W. F., Cherian R., Dixon A., McGregor D. H., Banerjee S. K. Short segment Barrett's esophagus: clinical and histological features, associated endoscopic findings, and association with gastric intestinal metaplasia. Am J Gastroenterol. 1996 May;91(5):981–986. [PubMed] [Google Scholar]
- Zaninotto G., DeMeester T. R., Schwizer W., Johansson K. E., Cheng S. C. The lower esophageal sphincter in health and disease. Am J Surg. 1988 Jan;155(1):104–111. doi: 10.1016/s0002-9610(88)80266-6. [DOI] [PubMed] [Google Scholar]