

Abstract
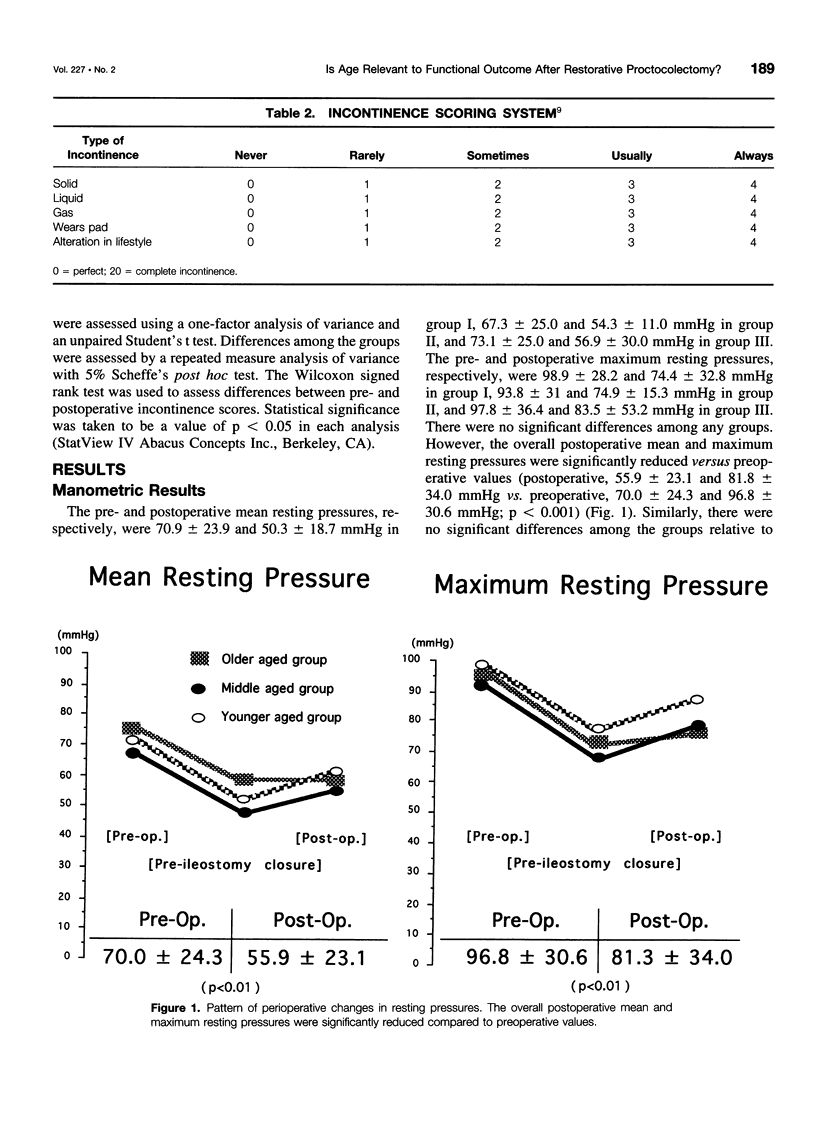
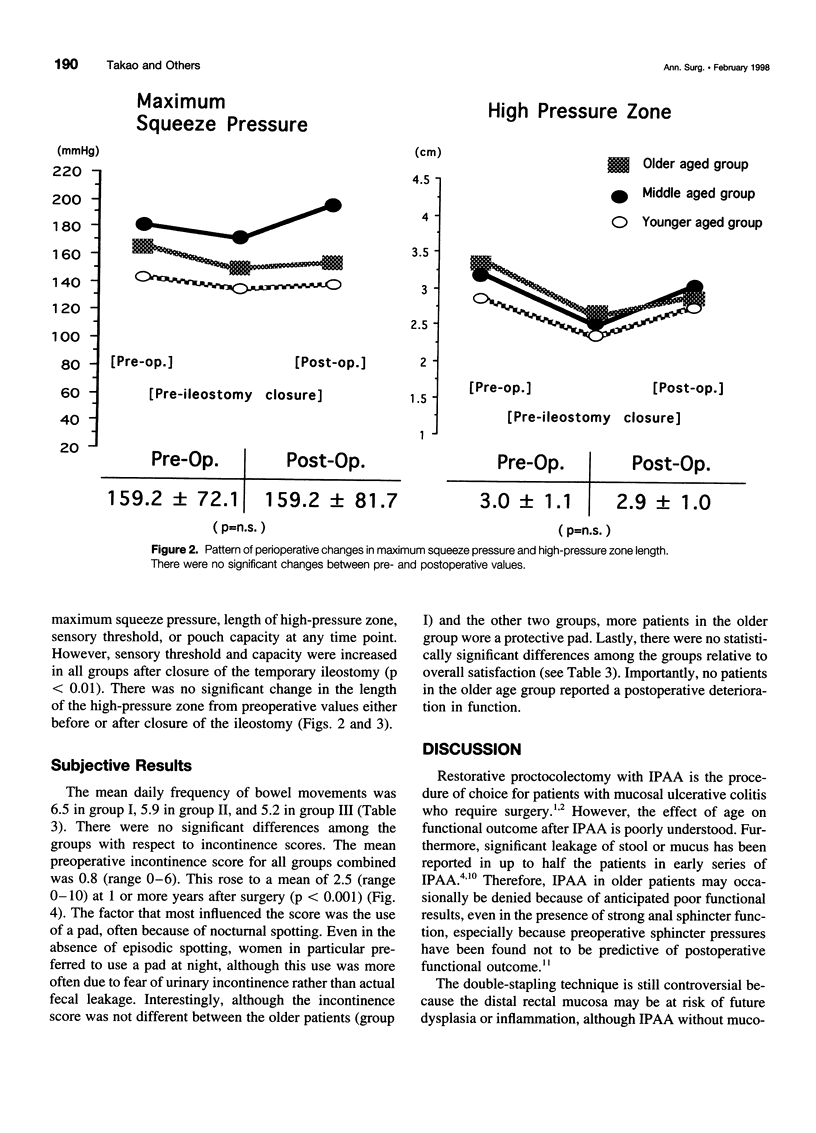
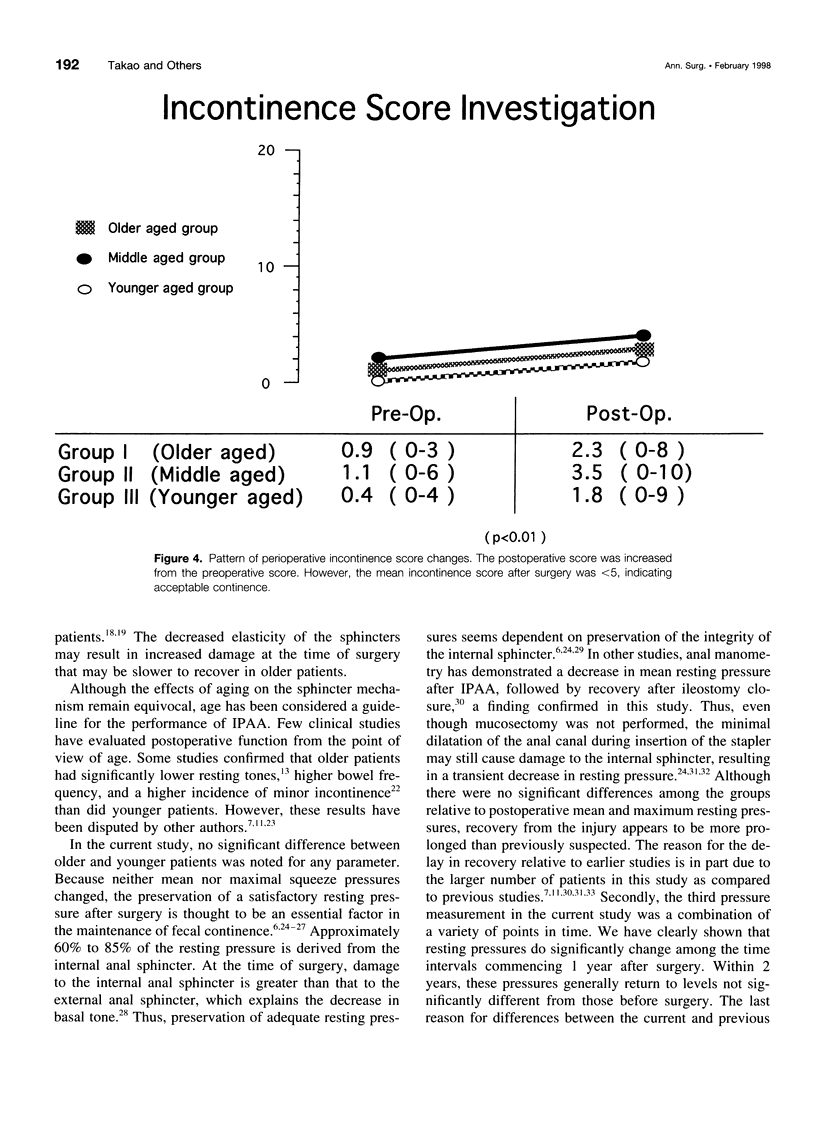
OBJECTIVE: Restorative proctocolectomy for mucosal ulcerative colitis is well established. However, the effect of age on physiologic sphincter parameters is poorly understood. Our objective was to determine whether age at the time of restorative proctocolectomy correlates with physiologic changes. SUMMARY BACKGROUND DATA: In the approximately 20 years during which restorative proctocolectomy has been performed for ulcerative colitis, the indications have changed. Initially, the procedure was recommended only in patients under approximately 50 years. However, the procedure has been considered in older patients because of the increasing age of our population, the increasing frequency of recognition of patients during the "second peak" of mucosal ulcerative colitis, and the decreasing morbidity rates, due to the learning curve and to newer techniques, such as double-stapling. Few authors have presented data analyzing the effects of this operation in older patients. METHODS: One hundred twenty-two patients who had undergone a two-stage restorative proctocolectomy for mucosal ulcerative colitis were divided into three groups according to age: group I (>60 years), 11 men, 6 women; group II (40-60 years), 29 men, 18 women; and group III (<40 years) 29 men, 29 women. The patients were prospectively evaluated using anal manometry and subjective functional results. Comparisons were made before surgery, after colectomy and before closure of ileostomy, and at 1 or more years after surgery. RESULTS: There were no significant differences among the groups relative to manometric results, frequency of bowel movements, incontinence scores, or overall patient satisfaction. The postoperative mean and maximum resting pressures were significantly reduced (p < 0.001), and conversely the sensory threshold (p < 0.005) and capacity (p < 0.001) were increased in all groups up to 1 year after surgery. There were no statistically significant changes in the squeeze pressure or length of the high-pressure zone in any group at any point in time. After surgery, the mean and maximum resting pressures had returned to 80% of their original values. CONCLUSION: Although anorectal function is transiently somewhat impaired after restorative proctocolectomy, the impairment is not an age-related phenomenon.
Full text
PDF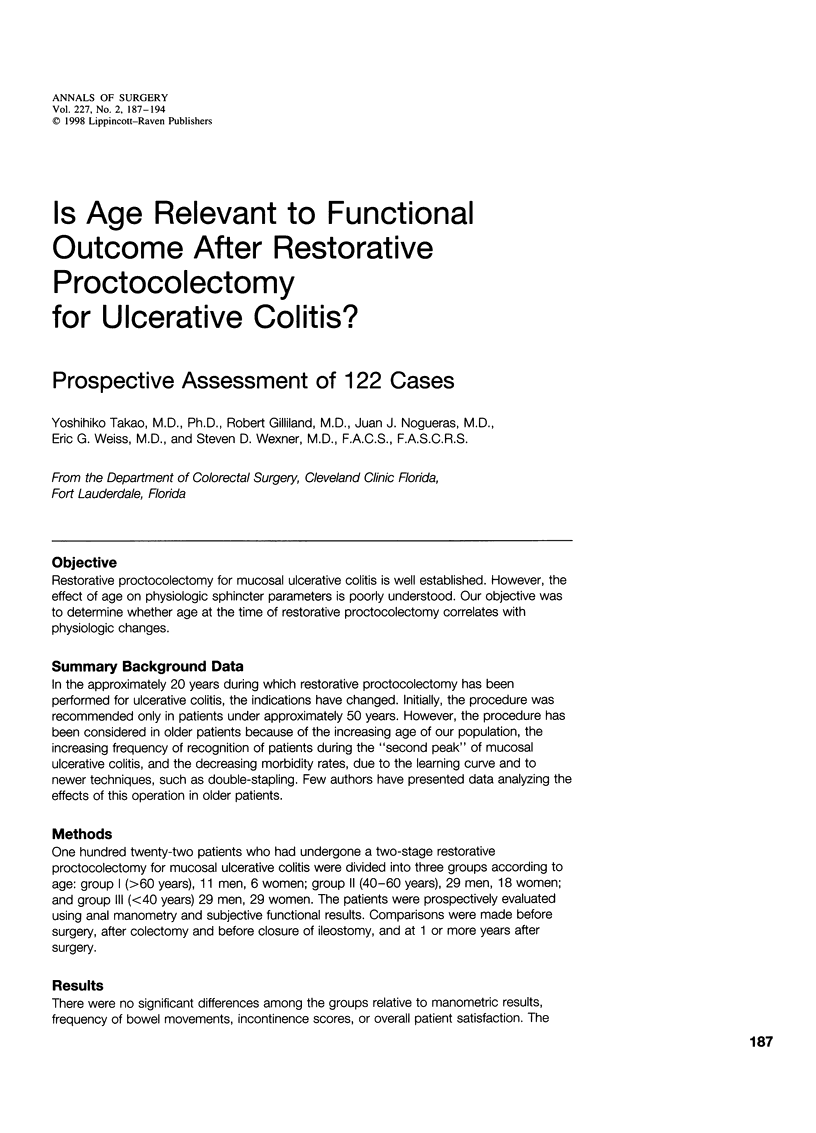

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bannister J. J., Abouzekry L., Read N. W. Effect of aging on anorectal function. Gut. 1987 Mar;28(3):353–357. doi: 10.1136/gut.28.3.353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Becker J. M. Anal sphincter function after colectomy, mucosal proctectomy, and endorectal ileoanal pull-through. Arch Surg. 1984 May;119(5):526–531. doi: 10.1001/archsurg.1984.01390170026006. [DOI] [PubMed] [Google Scholar]
- Becker J. M., Raymond J. L. Ileal pouch-anal anastomosis. A single surgeon's experience with 100 consecutive cases. Ann Surg. 1986 Oct;204(4):375–383. doi: 10.1097/00000658-198610000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dayton M. T., Morrell D. G. Factors associated with nighttime incontinence following ileoanal pullthrough. Am J Surg. 1991 Dec;162(6):599–602. doi: 10.1016/0002-9610(91)90117-v. [DOI] [PubMed] [Google Scholar]
- Goes R., Beart R. W., Jr Physiology of ileal pouch-anal anastomosis. Current concepts. Dis Colon Rectum. 1995 Sep;38(9):996–1005. doi: 10.1007/BF02049741. [DOI] [PubMed] [Google Scholar]
- Horgan P. G., O'Connell P. R., Shinkwin C. A., Kirwan W. O. Effect of anterior resection on anal sphincter function. Br J Surg. 1989 Aug;76(8):783–786. doi: 10.1002/bjs.1800760805. [DOI] [PubMed] [Google Scholar]
- Jagelman D. G. Surgical alternatives for ulcerative colitis. Med Clin North Am. 1990 Jan;74(1):155–167. doi: 10.1016/s0025-7125(16)30592-2. [DOI] [PubMed] [Google Scholar]
- Jameson J. S., Chia Y. W., Kamm M. A., Speakman C. T., Chye Y. H., Henry M. M. Effect of age, sex and parity on anorectal function. Br J Surg. 1994 Nov;81(11):1689–1692. doi: 10.1002/bjs.1800811143. [DOI] [PubMed] [Google Scholar]
- Johnston D., Holdsworth P. J., Nasmyth D. G., Neal D. E., Primrose J. N., Womack N., Axon A. T. Preservation of the entire anal canal in conservative proctocolectomy for ulcerative colitis: a pilot study comparing end-to-end ileo-anal anastomosis without mucosal resection with mucosal proctectomy and endo-anal anastomosis. Br J Surg. 1987 Oct;74(10):940–944. doi: 10.1002/bjs.1800741020. [DOI] [PubMed] [Google Scholar]
- Jorge J. M., Wexner S. D. Etiology and management of fecal incontinence. Dis Colon Rectum. 1993 Jan;36(1):77–97. doi: 10.1007/BF02050307. [DOI] [PubMed] [Google Scholar]
- Jorge J. M., Wexner S. D., James K., Nogueras J. J., Jagelman D. G. Recovery of anal sphincter function after the ileoanal reservoir procedure in patients over the age of fifty. Dis Colon Rectum. 1994 Oct;37(10):1002–1005. doi: 10.1007/BF02049312. [DOI] [PubMed] [Google Scholar]
- Keighley M. R., Yoshioka K., Kmiot W., Heyen F. Physiological parameters influencing function in restorative proctocolectomy and ileo-pouch-anal anastomosis. Br J Surg. 1988 Oct;75(10):997–1002. doi: 10.1002/bjs.1800751017. [DOI] [PubMed] [Google Scholar]
- Klosterhalfen B., Offner F., Topf N., Vogel P., Mittermayer C. Sclerosis of the internal anal sphincter--a process of aging. Dis Colon Rectum. 1990 Jul;33(7):606–609. doi: 10.1007/BF02052217. [DOI] [PubMed] [Google Scholar]
- Kmiot W. A., Keighley M. R. Totally stapled abdominal restorative proctocolectomy. Br J Surg. 1989 Sep;76(9):961–964. doi: 10.1002/bjs.1800760931. [DOI] [PubMed] [Google Scholar]
- Laurberg S., Swash M. Effects of aging on the anorectal sphincters and their innervation. Dis Colon Rectum. 1989 Sep;32(9):737–742. doi: 10.1007/BF02562120. [DOI] [PubMed] [Google Scholar]
- Lavery I. C., Tuckson W. B., Easley K. A. Internal anal sphincter function after total abdominal colectomy and stapled ileal pouch-anal anastomosis without mucosal proctectomy. Dis Colon Rectum. 1989 Nov;32(11):950–953. doi: 10.1007/BF02552271. [DOI] [PubMed] [Google Scholar]
- Lindquist K. Anal manometry with microtransducer technique before and after restorative proctocolectomy. Sphincter function and clinical correlations. Dis Colon Rectum. 1990 Feb;33(2):91–98. doi: 10.1007/BF02055534. [DOI] [PubMed] [Google Scholar]
- McHugh S. M., Diamant N. E. Effect of age, gender, and parity on anal canal pressures. Contribution of impaired anal sphincter function to fecal incontinence. Dig Dis Sci. 1987 Jul;32(7):726–736. doi: 10.1007/BF01296139. [DOI] [PubMed] [Google Scholar]
- McHugh S. M., Diamant N. E., McLeod R., Cohen Z. S-pouches vs. J-pouches. A comparison of functional outcomes. Dis Colon Rectum. 1987 Sep;30(9):671–677. doi: 10.1007/BF02561686. [DOI] [PubMed] [Google Scholar]
- Morgado P. J., Jr, Wexner S. D., James K., Nogueras J. J., Jagelman D. G. Ileal pouch-anal anastomosis: is preoperative anal manometry predictive of postoperative functional outcome? Dis Colon Rectum. 1994 Mar;37(3):224–228. doi: 10.1007/BF02048159. [DOI] [PubMed] [Google Scholar]
- Nasmyth D. G., Johnston D., Godwin P. G., Dixon M. F., Smith A., Williams N. S. Factors influencing bowel function after ileal pouch-anal anastomosis. Br J Surg. 1986 Jun;73(6):469–473. doi: 10.1002/bjs.1800730617. [DOI] [PubMed] [Google Scholar]
- Neill M. E., Swash M. Increased motor unit fibre density in the external anal sphincter muscle in ano-rectal incontinence: a single fibre EMG study. J Neurol Neurosurg Psychiatry. 1980 Apr;43(4):343–347. doi: 10.1136/jnnp.43.4.343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nicholls R. J. Restorative proctocolectomy with various types of reservoir. World J Surg. 1987 Dec;11(6):751–762. doi: 10.1007/BF01656598. [DOI] [PubMed] [Google Scholar]
- O'Connell P. R., Pemberton J. H., Brown M. L., Kelly K. A. Determinants of stool frequency after ileal pouch-anal anastomosis. Am J Surg. 1987 Feb;153(2):157–164. doi: 10.1016/0002-9610(87)90807-5. [DOI] [PubMed] [Google Scholar]
- O'Connell P. R., Stryker S. J., Metcalf A. M., Pemberton J. H., Kelly K. A. Anal canal pressure and motility after ileoanal anastomosis. Surg Gynecol Obstet. 1988 Jan;166(1):47–54. [PubMed] [Google Scholar]
- Oresland T., Fasth S., Nordgren S., Akervall S., Hultén L. Pouch size: the important functional determinant after restorative proctocolectomy. Br J Surg. 1990 Mar;77(3):265–269. doi: 10.1002/bjs.1800770310. [DOI] [PubMed] [Google Scholar]
- Reissman P., Piccirillo M., Ulrich A., Daniel N., Nogueras J. J., Wexner S. D. Functional results of the double-stapled ileoanal reservoir. J Am Coll Surg. 1995 Nov;181(5):444–450. [PubMed] [Google Scholar]
- Reissman P., Teoh T. A., Weiss E. G., Nogueras J. J., Wexner S. D. Functional outcome of the double stapled ileoanal reservoir in patients more than 60 years of age. Am Surg. 1996 Mar;62(3):178–183. [PubMed] [Google Scholar]
- Schmitt S. L., Wexner S. D., Lucas F. V., James K., Nogueras J. J., Jagelman D. G. Retained mucosa after double-stapled ileal reservoir and ileoanal anastomosis. Dis Colon Rectum. 1992 Nov;35(11):1051–1056. doi: 10.1007/BF02252995. [DOI] [PubMed] [Google Scholar]
- Stryker S. J., Kelly K. A., Phillips S. F., Dozois R. R., Beart R. W., Jr Anal and neorectal function after ileal pouch-anal anastomosis. Ann Surg. 1986 Jan;203(1):55–61. doi: 10.1097/00000658-198601000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tuckson W. B., Fazio V. W. Functional comparison between double and triple ileal loop pouches. Dis Colon Rectum. 1991 Jan;34(1):17–21. doi: 10.1007/BF02050201. [DOI] [PubMed] [Google Scholar]
- Tuckson W. B., McNamara M. J., Fazio V. W., Lavery I. C., Oakley J. R. Impact of anal manipulation and pouch design on ileal pouch function. J Natl Med Assoc. 1991 Dec;83(12):1089–1092. [PMC free article] [PubMed] [Google Scholar]
- Tuckson W., Lavery I., Fazio V., Oakley J., Church J., Milsom J. Manometric and functional comparison of ileal pouch anal anastomosis with and without anal manipulation. Am J Surg. 1991 Jan;161(1):90–96. doi: 10.1016/0002-9610(91)90366-l. [DOI] [PubMed] [Google Scholar]
- Vasilevsky C. A., Rothenberger D. A., Goldberg S. M. The S ileal pouch-anal anastomosis. World J Surg. 1987 Dec;11(6):742–750. doi: 10.1007/BF01656597. [DOI] [PubMed] [Google Scholar]
- Wexner S. D., James K., Jagelman D. G. The double-stapled ileal reservoir and ileoanal anastomosis. A prospective review of sphincter function and clinical outcome. Dis Colon Rectum. 1991 Jun;34(6):487–494. doi: 10.1007/BF02049935. [DOI] [PubMed] [Google Scholar]
- Wexner S. D., Wong W. D., Rothenberger D. A., Goldberg S. M. The ileoanal reservoir. Am J Surg. 1990 Jan;159(1):178–185. doi: 10.1016/s0002-9610(05)80625-7. [DOI] [PubMed] [Google Scholar]
- Williams N. S., Marzouk D. E., Hallan R. I., Waldron D. J. Function after ileal pouch and stapled pouch-anal anastomosis for ulcerative colitis. Br J Surg. 1989 Nov;76(11):1168–1171. doi: 10.1002/bjs.1800761119. [DOI] [PubMed] [Google Scholar]