

Abstract
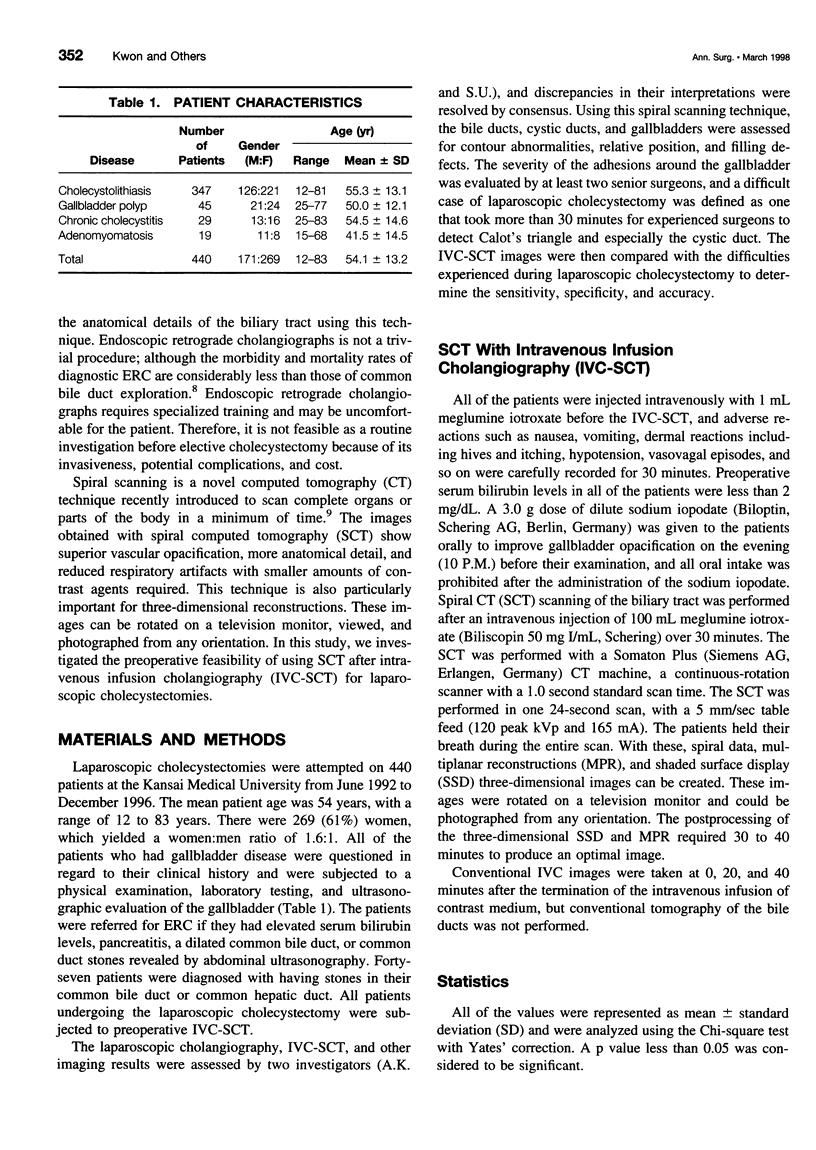
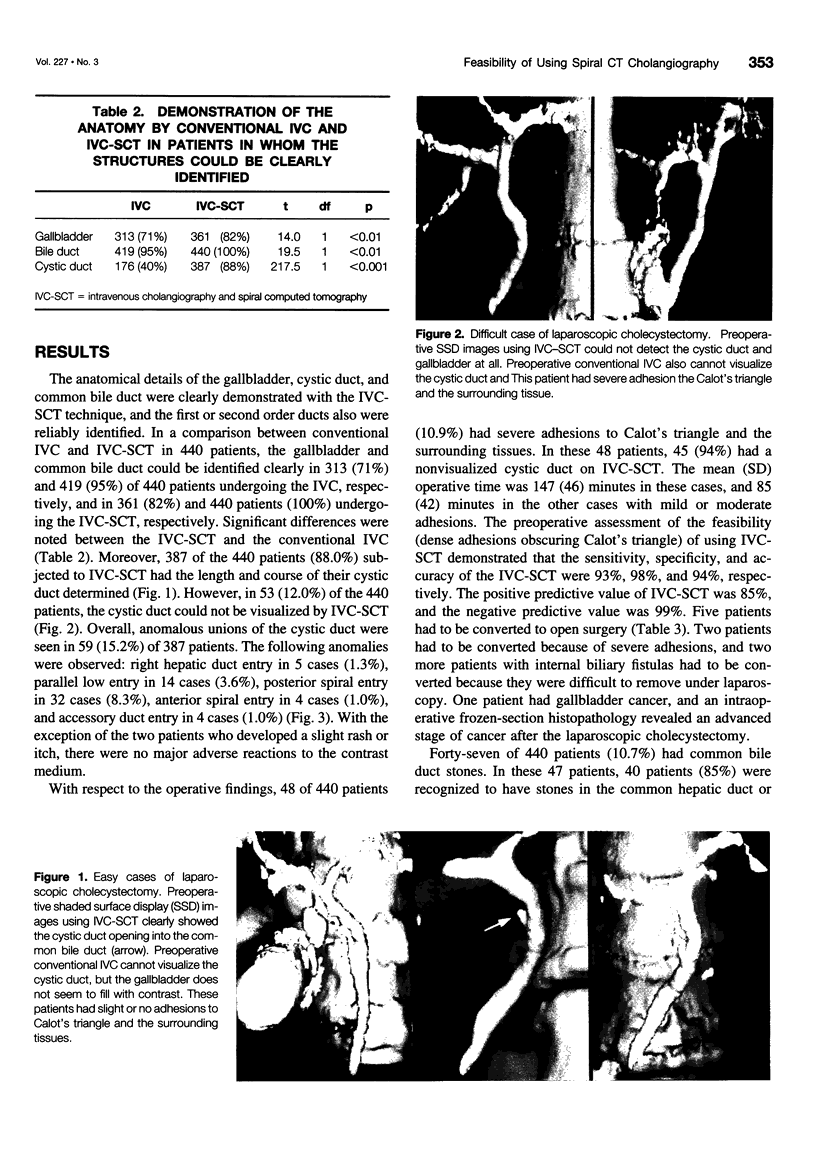
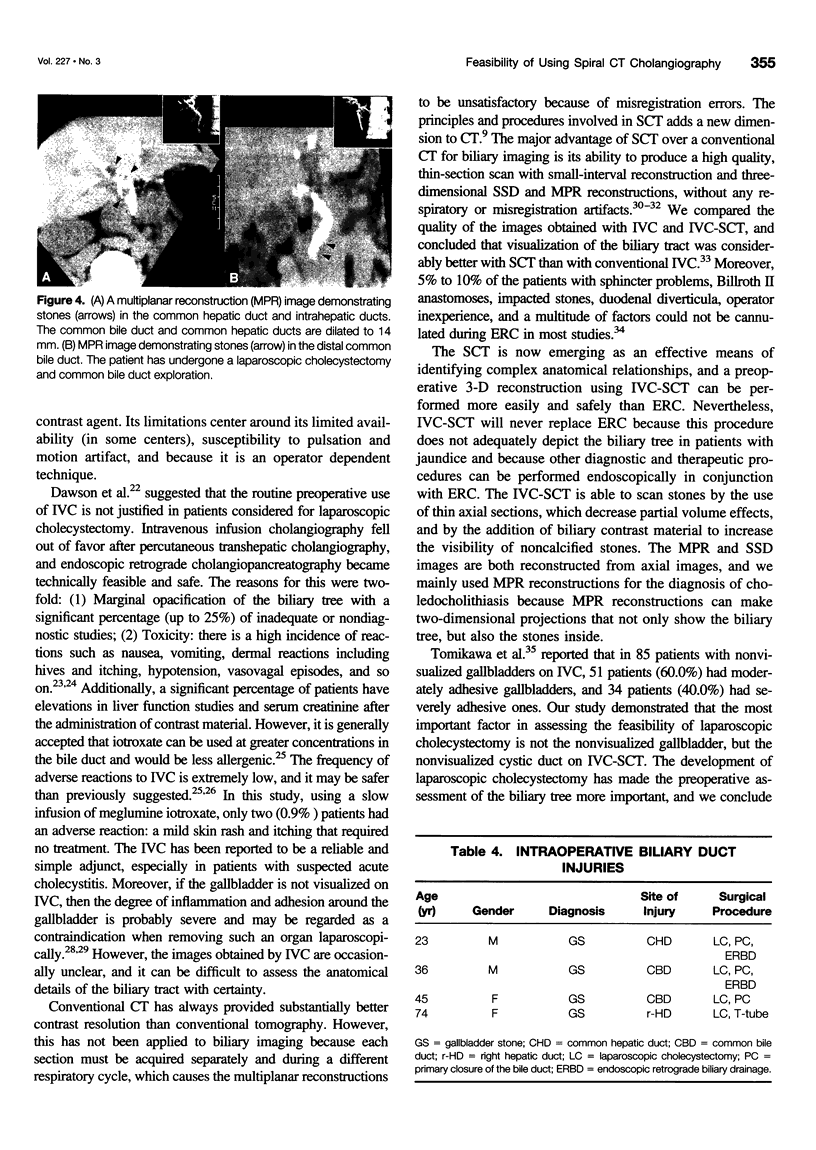
OBJECTIVE: The authors investigated the preoperative feasibility of using spiral computed tomography (SCT) after intravenous infusion cholangiography (IVC-SCT) for laparoscopic cholecystectomy. SUMMARY BACKGROUND DATA: In laparoscopic cholecystectomy, the aberrant or unusual anatomy of the bile duct and severe inflammation or adhesions around the gallbladder sometimes require a conversion to open surgery. METHODS: Laparoscopic cholecystectomies (LC's) were attempted on 440 patients, and preoperative IVC-SCT also was attempted in all of these patients. Using this spiral scanning technique, the bile ducts, cystic duct, and gallbladder were assessed for contour abnormalities, relative position, and filling defects. Forty-seven patients were diagnosed with having stones in their common bile duct or common hepatic duct. RESULTS: Three-hundred eighty-seven patients out of the 440 patients (88.0%) who were subjected to IVC-SCT had the length and course of their cystic duct successfully determined. Anomalous unions of the cystic duct were seen in 59 (15.2%) of 387 patients with respect to the operative findings, and 48 of 440 patients (10.9%) had severe adhesions to Calot's triangle and the surrounding tissues. In these 48 patients, 45 patients (94%) had a nonvisualized cystic duct on IVC-SCT. The preoperative assessment of the feasibility (dense adhesions obscuring Calot's triangle) of using IVC-SCT demonstrated that the sensitivity, specificity, and accuracy were 93%, 98%, and 94%, respectively. Five patients had to be converted to open surgery, and the overall morbidity rates for patients undergoing laparoscopic cholecystectomy was 0.9% (4 of 440). CONCLUSIONS: The most important factor in assessing the feasibility of using laparoscopic cholecystectomy is not the nonvisualized gallbladder, but the nonvisualized cystic duct on IVC-SCT. IVC-SCT may be of benefit to those patients scheduled to undergo laparoscopic cholecystectomy.
Full text
PDF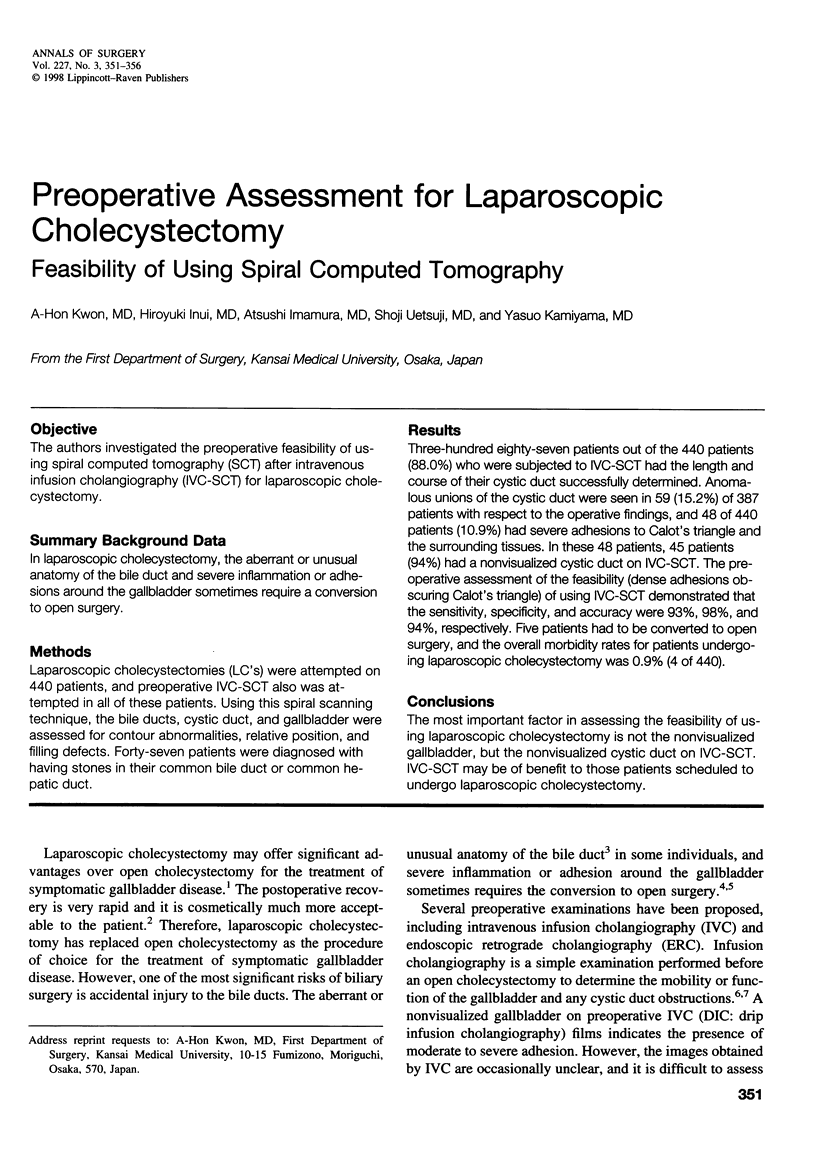
Images in this article


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Alinder G., Nilsson U., Lunderquist A., Herlin P., Holmin T. Pre-operative infusion cholangiography compared to routine operative cholangiography at elective cholecystectomy. Br J Surg. 1986 May;73(5):383–387. doi: 10.1002/bjs.1800730524. [DOI] [PubMed] [Google Scholar]
- Alinder G., Nilsson U., Lunderquist A., Herlin P., Holmin T. Pre-operative infusion cholangiography compared to routine operative cholangiography at elective cholecystectomy. Br J Surg. 1986 May;73(5):383–387. doi: 10.1002/bjs.1800730524. [DOI] [PubMed] [Google Scholar]
- Bailey R. W., Zucker K. A., Flowers J. L., Scovill W. A., Graham S. M., Imbembo A. L. Laparoscopic cholecystectomy. Experience with 375 consecutive patients. Ann Surg. 1991 Oct;214(4):531–541. doi: 10.1097/00000658-199110000-00017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheslyn-Curtis S., Emberton M., Ahmed H., Williamson R. C., Habib N. A. Bile duct injury following laparoscopic cholecystectomy. Br J Surg. 1992 Mar;79(3):231–232. doi: 10.1002/bjs.1800790314. [DOI] [PubMed] [Google Scholar]
- Cuschieri A., Dubois F., Mouiel J., Mouret P., Becker H., Buess G., Trede M., Troidl H. The European experience with laparoscopic cholecystectomy. Am J Surg. 1991 Mar;161(3):385–387. doi: 10.1016/0002-9610(91)90603-b. [DOI] [PubMed] [Google Scholar]
- Dawson P., Adam A., Benjamin I. S. Intravenous cholangiography revisited. Clin Radiol. 1993 Apr;47(4):223–225. doi: 10.1016/s0009-9260(05)81127-4. [DOI] [PubMed] [Google Scholar]
- Dubois F., Berthelot G., Levard H. Laparoscopic cholecystectomy: historic perspective and personal experience. Surg Laparosc Endosc. 1991 Mar;1(1):52–57. [PubMed] [Google Scholar]
- Dubois F., Icard P., Berthelot G., Levard H. Coelioscopic cholecystectomy. Preliminary report of 36 cases. Ann Surg. 1990 Jan;211(1):60–62. doi: 10.1097/00000658-199001000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goor D. A., Ebert P. A. Anomalies of the biliary tree. Report of a repair of an accessory bile duct and review of the literature. Arch Surg. 1972 Mar;104(3):302–309. doi: 10.1001/archsurg.1972.04180030050012. [DOI] [PubMed] [Google Scholar]
- HAYES M. A., GOLDENBERG I. S., BISHOP C. C. The developmental basis for bile duct anomalies. Surg Gynecol Obstet. 1958 Oct;107(4):447–456. [PubMed] [Google Scholar]
- HEALEY J. E., Jr, SCHROY P. C. Anatomy of the biliary ducts within the human liver; analysis of the prevailing pattern of branchings and the major variations of the biliary ducts. AMA Arch Surg. 1953 May;66(5):599–616. doi: 10.1001/archsurg.1953.01260030616008. [DOI] [PubMed] [Google Scholar]
- Heiken J. P., Brink J. A., Vannier M. W. Spiral (helical) CT. Radiology. 1993 Dec;189(3):647–656. doi: 10.1148/radiology.189.3.8234684. [DOI] [PubMed] [Google Scholar]
- Hermann R. E. Editorial: A plea for a safer technique of cholecystectomy. Surgery. 1976 Jun;79(6):609–611. [PubMed] [Google Scholar]
- Kalender W. A., Seissler W., Klotz E., Vock P. Spiral volumetric CT with single-breath-hold technique, continuous transport, and continuous scanner rotation. Radiology. 1990 Jul;176(1):181–183. doi: 10.1148/radiology.176.1.2353088. [DOI] [PubMed] [Google Scholar]
- Klein H. M., Wein B., Truong S., Pfingsten F. P., Günther R. W. Computed tomographic cholangiography using spiral scanning and 3D image processing. Br J Radiol. 1993 Sep;66(789):762–767. doi: 10.1259/0007-1285-66-789-762. [DOI] [PubMed] [Google Scholar]
- Kwon A. H., Uetsuji S., Yamada O., Inoue T., Kamiyama Y., Boku T. Three-dimensional reconstruction of the biliary tract using spiral computed tomography. Br J Surg. 1995 Feb;82(2):260–263. doi: 10.1002/bjs.1800820241. [DOI] [PubMed] [Google Scholar]
- MOOSMAN D. A. ACCESSORY BILE DUCTS: THEIR SIGNIFICANCE DURING CHOLECYSTECTOMY. J Mich State Med Soc. 1964 May;63:355–358. [PubMed] [Google Scholar]
- McCormick J. S., Bremner D. N., Thomson J. W., McNair T. J., Philp T. The operative cholangiogram: its interpretation, accuracy and value in association with cholecystectomy. Ann Surg. 1974 Dec;180(6):902–906. doi: 10.1097/00000658-197412000-00019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McSherry C. K. Cholecystectomy: the gold standard. Am J Surg. 1989 Sep;158(3):174–178. doi: 10.1016/0002-9610(89)90246-8. [DOI] [PubMed] [Google Scholar]
- Napel S., Marks M. P., Rubin G. D., Dake M. D., McDonnell C. H., Song S. M., Enzmann D. R., Jeffrey R. B., Jr CT angiography with spiral CT and maximum intensity projection. Radiology. 1992 Nov;185(2):607–610. doi: 10.1148/radiology.185.2.1410382. [DOI] [PubMed] [Google Scholar]
- Nilsson U. Adverse reactions to iotroxate at intravenous cholangiography. A prospective clinical investigation and review of the literature. Acta Radiol. 1987 Sep-Oct;28(5):571–575. [PubMed] [Google Scholar]
- Ott D. J., Gelfand D. W. Complications of gastrointestinal radiologic procedures: II. Complications related to biliary tract studies. Gastrointest Radiol. 1981 Jan 15;6(1):47–56. doi: 10.1007/BF01890221. [DOI] [PubMed] [Google Scholar]
- Pasquale M. D., Nauta R. J. Selective vs routine use of intraoperative cholangiography. An argument. Arch Surg. 1989 Sep;124(9):1041–1042. doi: 10.1001/archsurg.1989.01410090047010. [DOI] [PubMed] [Google Scholar]
- Pollack E. L., Tabrisky J. The aberrant divisional bile duct: a surgical hazard. Surgery. 1973 Feb;73(2):234–239. [PubMed] [Google Scholar]
- Raute M., Schaupp W. Iatrogene Schäden an den Gallenwegen infolge Cholecystektomie. Behandlung und Ergebnisse. Langenbecks Arch Chir. 1988;373(6):345–354. doi: 10.1007/BF01272553. [DOI] [PubMed] [Google Scholar]
- Reddick E. J., Olsen D., Spaw A., Baird D., Asbun H., O'Reilly M., Fisher K., Saye W. Safe performance of difficult laparoscopic cholecystectomies. Am J Surg. 1991 Mar;161(3):377–381. doi: 10.1016/0002-9610(91)90601-9. [DOI] [PubMed] [Google Scholar]
- Rholl K. S., Smathers R. L., McClennan B. L., Lee J. K. Intravenous cholangiography in the CT era. Gastrointest Radiol. 1985;10(1):69–74. doi: 10.1007/BF01893073. [DOI] [PubMed] [Google Scholar]
- Sackier J. M., Berci G., Phillips E., Carroll B., Shapiro S., Paz-Partlow M. The role of cholangiography in laparoscopic cholecystectomy. Arch Surg. 1991 Aug;126(8):1021–1026. doi: 10.1001/archsurg.1991.01410320111016. [DOI] [PubMed] [Google Scholar]
- Salky B. A., Bauer J. J., Kreel I., Gelernt I. M., Gorfine S. R. Laparoscopic cholecystectomy: an initial report. Gastrointest Endosc. 1991 Jan-Feb;37(1):1–4. doi: 10.1016/s0016-5107(91)70611-1. [DOI] [PubMed] [Google Scholar]
- Sherman S., Lehman G. A. ERCP- and endoscopic sphincterotomy-induced pancreatitis. Pancreas. 1991 May;6(3):350–367. doi: 10.1097/00006676-199105000-00013. [DOI] [PubMed] [Google Scholar]
- Tomikawa M., Kitano S., Iso Y., Hashizume M., Moriyama M., Ohta M., Higashi H., Sugimachi K. Feasibility of laparoscopic cholecystectomy for patients with a nonvisualized gallbladder on drip infusion cholangiography. Surg Laparosc Endosc. 1995 Apr;5(2):121–124. [PubMed] [Google Scholar]