

Abstract
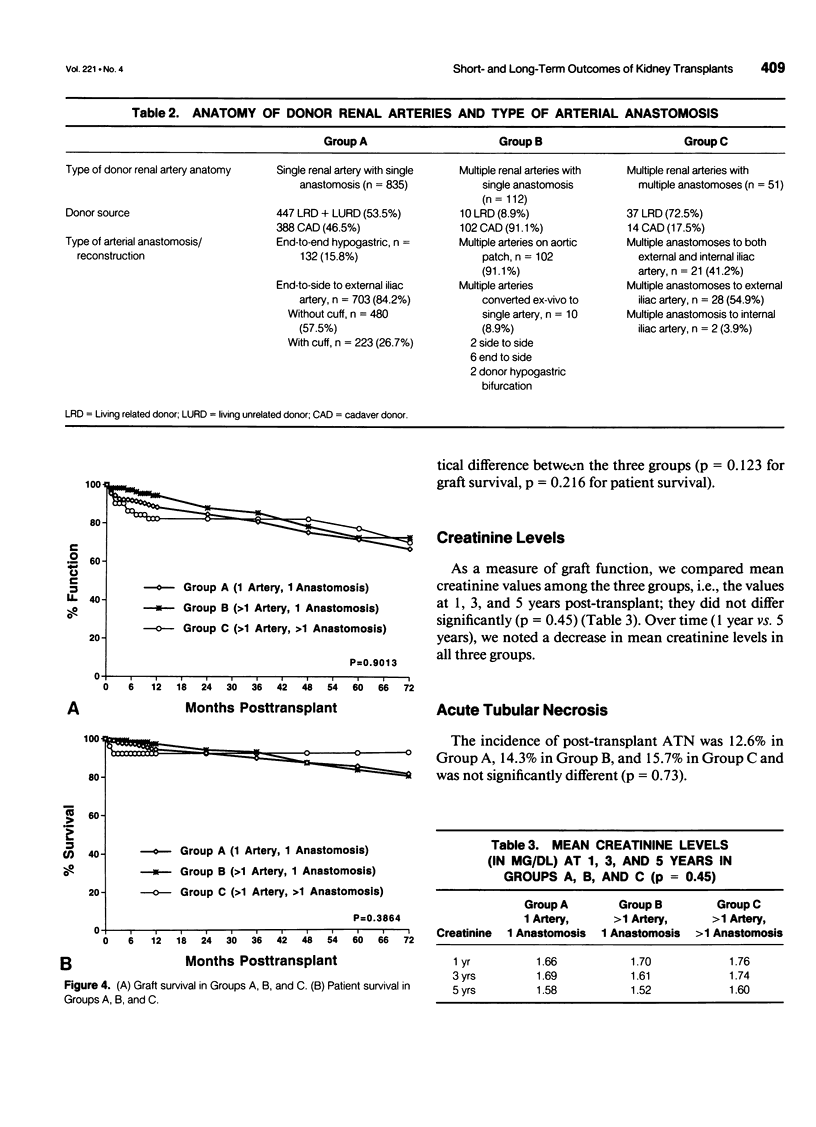
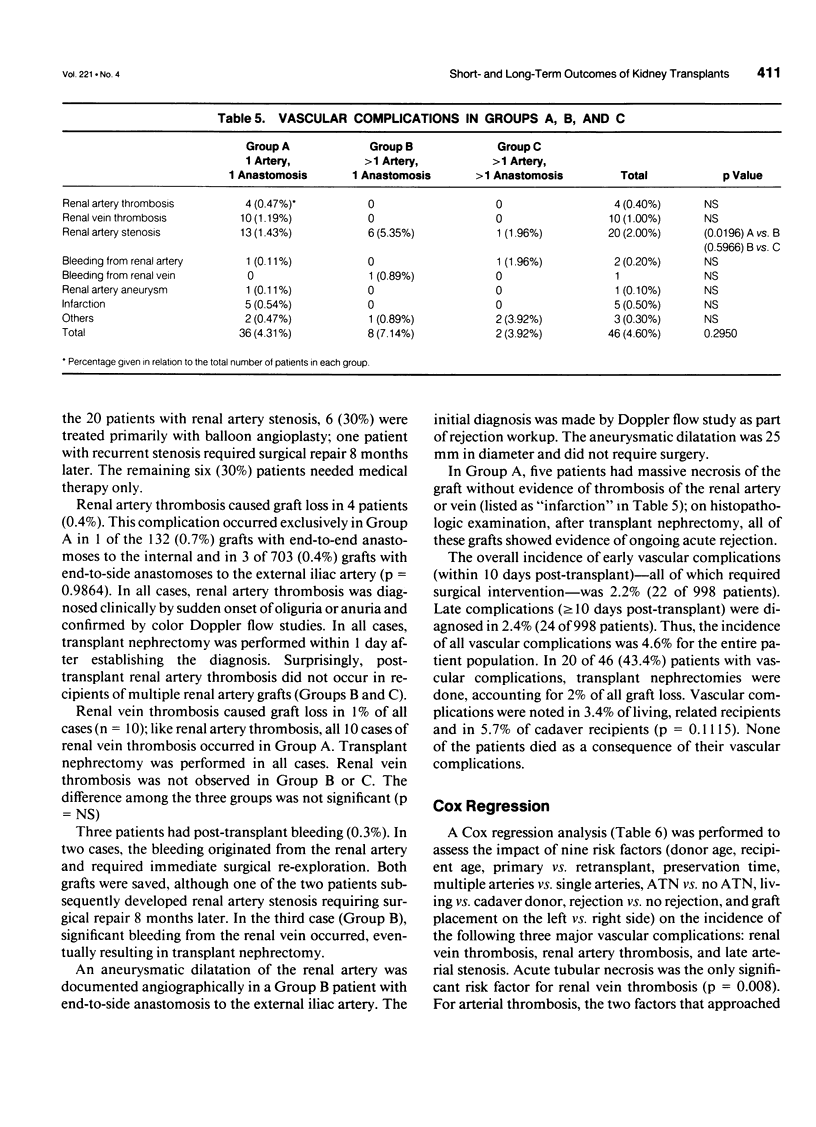
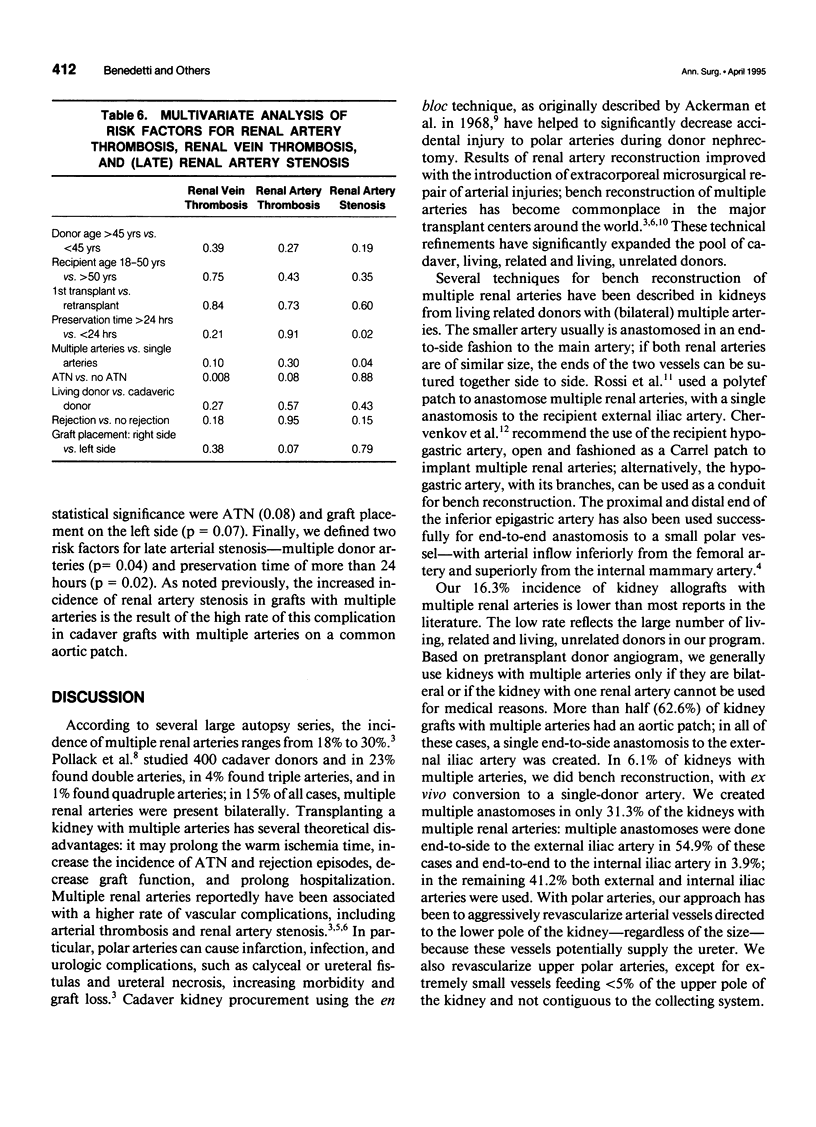
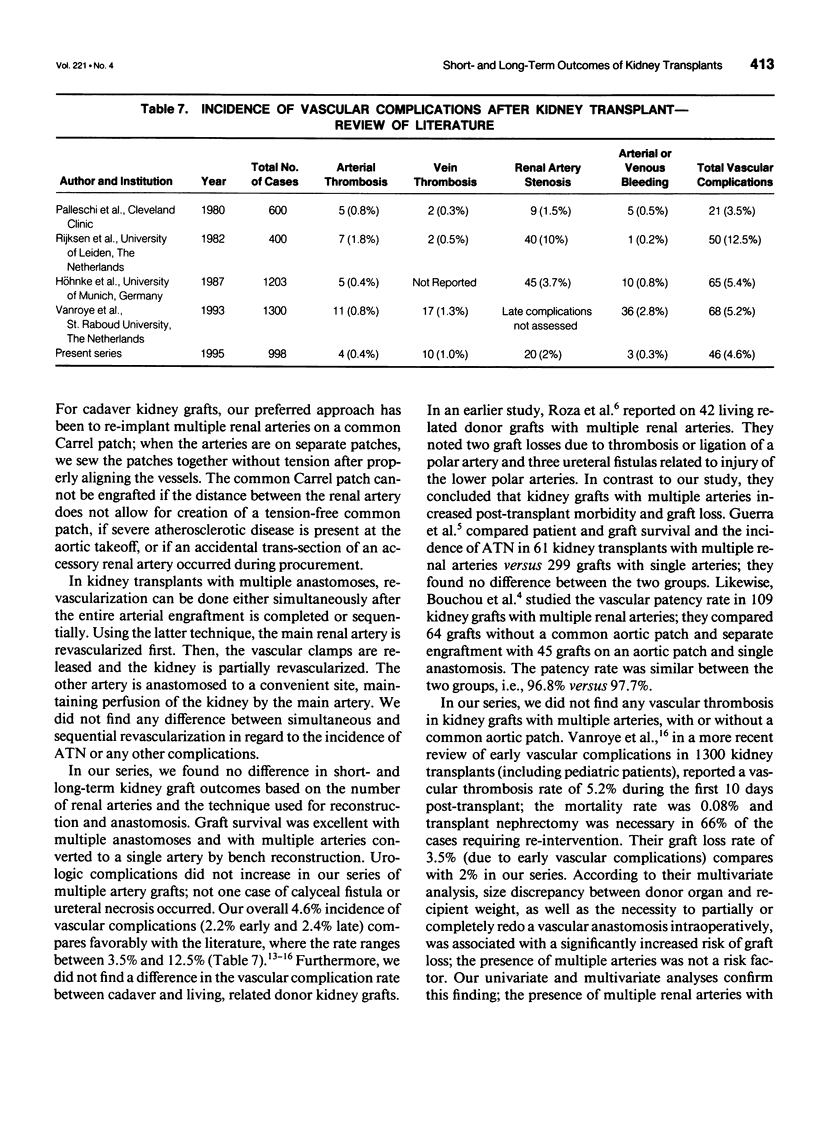
OBJECTIVE: The authors determined whether the use of kidney allografts with multiple renal arteries adversely effects post-transplant graft and patient outcome or increases the incidence of vascular and urologic complications. BACKGROUND: Kidney grafts with multiple renal arteries have been associated with an increased incidence of early vascular and urologic complications. Kidney transplants with single versus multiple renal arteries have not been compared in regard to long-term graft and patient outcome or post-transplant incidence of hypertension, acute tubular necrosis, rejection, and late vascular and urologic complications. METHODS: We analyzed 998 adult kidney transplants done from December 1, 1985 through June 30, 1993, in which only the recipient's external or internal iliac artery was used for anastomosis. We divided the study population into 3 groups: Group A-1 renal artery, 1 arterial anastomosis (n = 835), Group B-->1 renal artery, 1 arterial anastomosis (n = 112), Group C-->1 renal artery, > 1 arterial anastomosis (n = 51). We compared the incidence of post-transplant hypertension, acute tubular necrosis, acute rejection, and vascular and urologic complications; mean creatinine levels at 1, 3, and 5 years post-transplant; and patient and graft survival. Univariate and multivariate analyses were done to identify risk factors for vascular complications. RESULTS: We found no significant differences among the three groups for the following variables: post-transplant hypertension, acute tubular necrosis, acute rejection, creatinine levels, early vascular and urologic complications, and graft and patient survival. In kidneys with single arteries, the presence (vs. absence) of an aortic patch and the type of the arterial anastomosis (end-to-end to the hypogastric vs. end-to-side to the external iliac artery) did not have an impact on the incidence of early or late vascular complications. In kidneys with multiple arteries, only the rate of late renal artery stenosis was higher, the rate of early vascular and urologic complications was not different. Our multivariate analysis identified acute tubular necrosis as a risk factor for renal artery and vein thrombosis; graft placement on the left side for arterial thrombosis; and preservation time > or = 24 hours and multiple renal arteries for renal artery stenosis. CONCLUSIONS: Results of kidney transplants using allografts with multiple versus single arteries are similar.
Full text
PDF

Images in this article


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ackermann J. R., Snell M. E. Cadaveric renal transplantation: a technique for donor kidney removal. Br J Urol. 1968 Oct;40(5):515–521. doi: 10.1111/j.1464-410x.1968.tb11842.x. [DOI] [PubMed] [Google Scholar]
- Aguiló J., Rodriguez O., Gaete J., Galleguillos I. Vascular anastomosis techniques in renal transplants. Int Angiol. 1991 Jan-Mar;10(1):39–43. [PubMed] [Google Scholar]
- Belli L., De Carlis L., Belli L. S., Del Favero E., Puttini M., Aseni P., Rondinaria G. F., Meroni A., Beati C. Thromboendarterectomy (TEA) in the recipient as a major risk of arterial complication after kidney transplantation. Int Angiol. 1989 Oct-Dec;8(4):206–209. [PubMed] [Google Scholar]
- Guerra E. E., Didoné E. C., Zanotelli M. L., Vitola S. P., Cantisani G. P., Goldani J. C., Keitel E., Garcia V. D. Renal transplants with multiple arteries. Transplant Proc. 1992 Oct;24(5):1868–1868. [PubMed] [Google Scholar]
- Höhnke C., Abendroth D., Schleibner S., Land W. Vascular complications in 1,200 kidney transplantations. Transplant Proc. 1987 Oct;19(5):3691–3692. [PubMed] [Google Scholar]
- Oakes D. D., Spees E. K., Jr, Light J. A. Renovascular hypertension after transplantation of a kidney perfused via multiple renal arteries. Am Surg. 1981 Jun;47(6):272–274. [PubMed] [Google Scholar]
- Oesterwitz H., Strobelt V., Scholz D., Mebel M. Extracorporeal microsurgical repair of injured multiple donor kidney arteries prior to cadaveric allotransplantation. Eur Urol. 1985;11(2):100–105. doi: 10.1159/000472465. [DOI] [PubMed] [Google Scholar]
- Palleschi J., Novick A. C., Braun W. E., Magnusson M. O. Vascular complications of renal transplantation. Urology. 1980 Jul;16(1):61–67. doi: 10.1016/0090-4295(80)90333-7. [DOI] [PubMed] [Google Scholar]
- Pollak R., Prusak B. F., Mozes M. F. Anatomic abnormalities of cadaver kidneys procured for purposes of transplantation. Am Surg. 1986 May;52(5):233–235. [PubMed] [Google Scholar]
- Pourmand G., Mehraban D., Ameli P. J., Ayati M., Naderi G. Donor polar kidney arteries: experience with 10 cases among 140 living-related kidney transplants. Transplant Proc. 1992 Oct;24(5):1867–1867. [PubMed] [Google Scholar]
- Rijksen J. F., Koolen M. I., Walaszewski J. E., Terpstra J. L., Vink M. Vascular complications in 400 consecutive renal allotransplants. J Cardiovasc Surg (Torino) 1982 Mar-Apr;23(2):91–98. [PubMed] [Google Scholar]
- Rossi M., Alfani D., Berloco P., Bruzzone P., Caricato M., Casciaro G., Poli L., Iappelli M., Pecorella I., Pretagostini R. Bench surgery for multiple renal arteries in kidney transplantation from living donor. Transplant Proc. 1991 Oct;23(5):2328–2329. [PubMed] [Google Scholar]
- Roza A. M., Perloff L. J., Naji A., Grossman R. A., Barker C. F. Living-related donors with bilateral multiple renal arteries. A twenty-year experience. Transplantation. 1989 Feb;47(2):397–399. [PubMed] [Google Scholar]
- Tchervenkov J. I., Munda R. The use of the hypogastric artery in the anastomosis of multiple renal arteries in the transplant patient. Transpl Int. 1990 Jul;3(2):116–117. doi: 10.1007/BF00336216. [DOI] [PubMed] [Google Scholar]