

Abstract
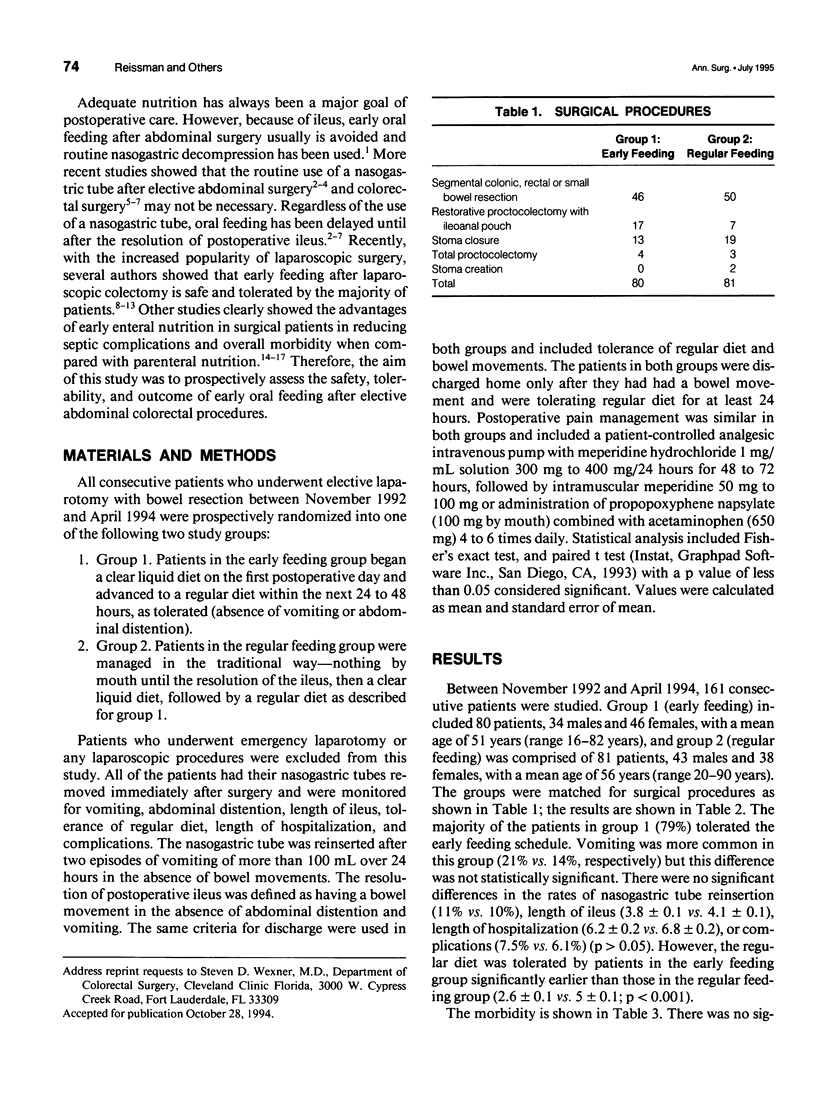
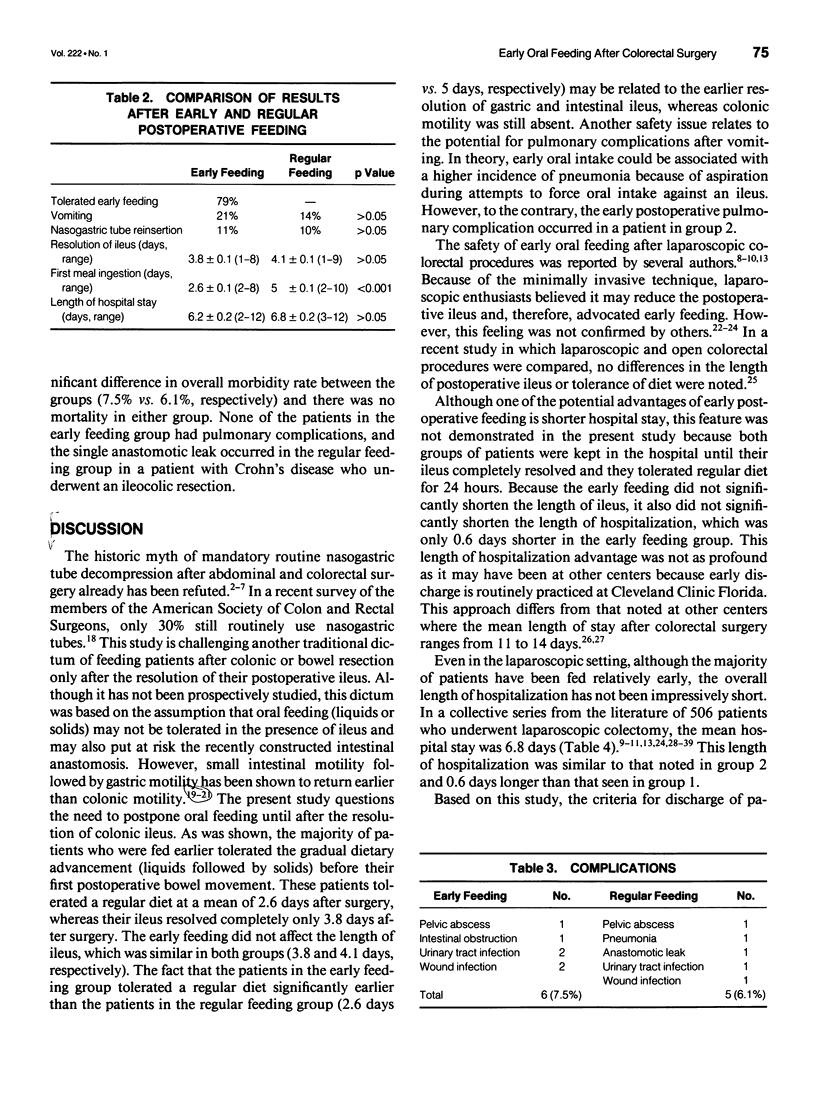
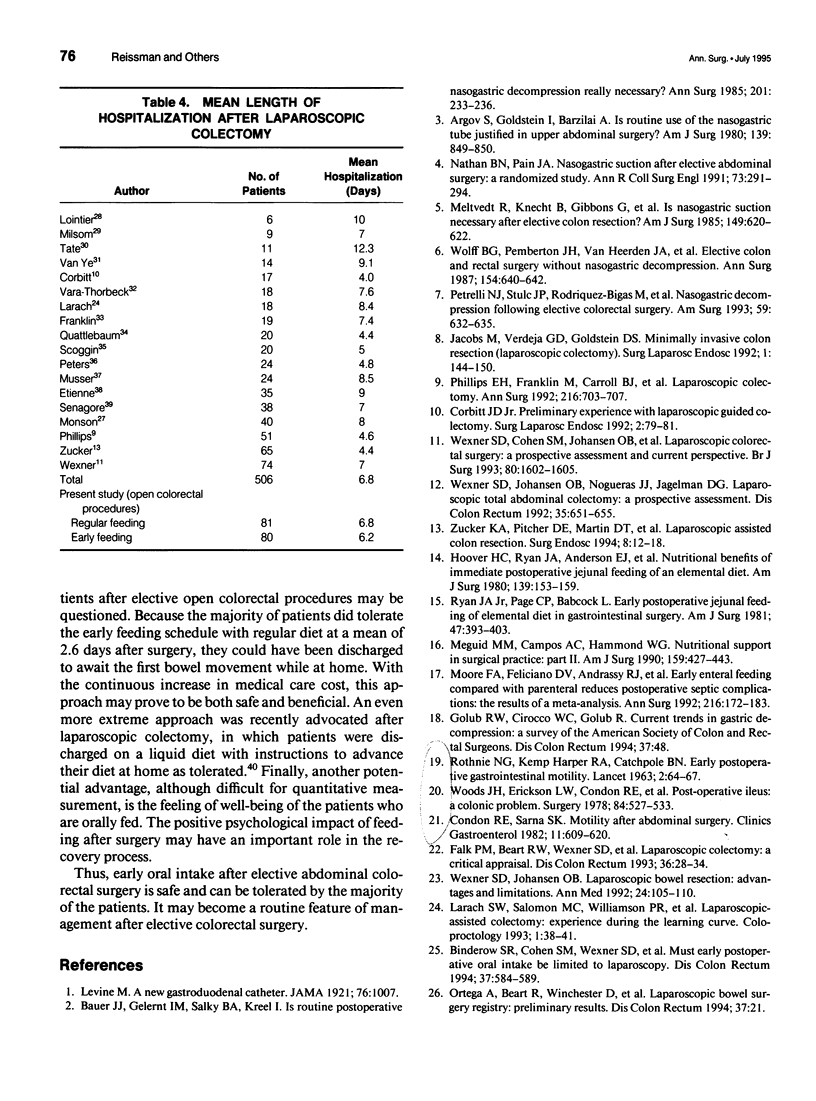
INTRODUCTION: The routine use of a nasogastric tube after elective colorectal surgery is no longer mandatory. More recently, early feeding after laparoscopic colectomy has been shown to be safe and well tolerated. Therefore, the aim of our study was to prospectively assess the safety and tolerability of early oral feeding after elective "open" abdominal colorectal operations. MATERIALS AND METHODS: All patients who underwent elective laparotomy with either colon or small bowel resection between November 1992 and April 1994 were prospectively randomized to one of the following two groups: group 1: early oral feeding--all patients received a clear liquid diet on the first postoperative day followed by a regular diet as tolerated; group 2: regular feeding--all patients were treated in the "traditional" way, with feeding only after the resolution of their postoperative ileus. The nasogastric tube was removed from all patients in both groups immediately after surgery. The patients were monitored for vomiting, bowel movements, nasogastric tube reinsertion, time of regular diet consumption, complications, and length of hospitalization. The nasogastric tube was reinserted if two or more episodes of vomiting of more than 100 mL occurred in the absence of bowel movement. Ileus was considered resolved after a bowel movement in the absence of abdominal distention or vomiting. RESULTS: One hundred sixty-one consecutive patients were studied, 80 patients in group 1 (34 males and 46 females, mean age 51 years [range 16-82 years]), and 81 patients in group 2 (43 males and 38 females, mean age 56 years [range 20-90 years]). Sixty-three patients (79%) in the early feeding group tolerated the early feeding schedule and were advanced to regular diet within the next 24 to 48 hours. There were no significant differences between the early and regular feeding groups in the rate of vomiting (21% vs. 14%), nasogastric tube reinsertion (11% vs. 10%), length of ileus (3.8 +/- 0.1 days vs. 4.1 +/- 0.1 days), length of hospitalization (6.2 +/- 0.2 days vs. 6.8 +/- 0.2 days), or overall complications (7.5% vs. 6.1%), respectively, (p = NS for all). However, the patients in the early feeding group tolerated a regular diet significantly earlier than did the patients in the regular feeding group (2.6 +/- 0.1 days vs. 5 +/- 0.1 days; p < 0.001). CONCLUSION: Early oral feeding after elective colorectal surgery is safe and can be tolerated by the majority of patients. Thus, it may become a routine feature of postoperative management in these patients.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Argov S., Goldstein I., Barzilai A. Is routine use of the nasogastric tube justified in upper abdominal surgery? Am J Surg. 1980 Jun;139(6):849–850. doi: 10.1016/0002-9610(80)90395-5. [DOI] [PubMed] [Google Scholar]
- Bauer J. J., Gelernt I. M., Salky B. A., Kreel I. Is routine postoperative nasogastric decompression really necessary? Ann Surg. 1985 Feb;201(2):233–236. doi: 10.1097/00000658-198502000-00017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Binderow S. R., Cohen S. M., Wexner S. D., Nogueras J. J. Must early postoperative oral intake be limited to laparoscopy? Dis Colon Rectum. 1994 Jun;37(6):584–589. doi: 10.1007/BF02050994. [DOI] [PubMed] [Google Scholar]
- Condon R. E., Sarna S. K. Motility after abdominal surgery. Clin Gastroenterol. 1982 Sep;11(3):609–620. [PubMed] [Google Scholar]
- Corbitt J. D., Jr Preliminary experience with laparoscopic-guided colectomy. Surg Laparosc Endosc. 1992 Mar;2(1):79–81. [PubMed] [Google Scholar]
- Falk P. M., Beart R. W., Jr, Wexner S. D., Thorson A. G., Jagelman D. G., Lavery I. C., Johansen O. B., Fitzgibbons R. J., Jr Laparoscopic colectomy: a critical appraisal. Dis Colon Rectum. 1993 Jan;36(1):28–34. doi: 10.1007/BF02050298. [DOI] [PubMed] [Google Scholar]
- Franklin M. E., Jr, Ramos R., Rosenthal D., Schuessler W. Laparoscopic colonic procedures. World J Surg. 1993 Jan-Feb;17(1):51–56. doi: 10.1007/BF01655705. [DOI] [PubMed] [Google Scholar]
- Hoover H. C., Jr, Ryan J. A., Anderson E. J., Fischer J. E. Nutritional benefits of immediate postoperative jejunal feeding of an elemental diet. Am J Surg. 1980 Jan;139(1):153–159. doi: 10.1016/0002-9610(80)90245-7. [DOI] [PubMed] [Google Scholar]
- Jacobs M., Verdeja J. C., Goldstein H. S. Minimally invasive colon resection (laparoscopic colectomy). Surg Laparosc Endosc. 1991 Sep;1(3):144–150. [PubMed] [Google Scholar]
- Lointier P. H., Lautard M., Massoni C., Ferrier C., Dapoigny M. Laparoscopically assisted subtotal colectomy. J Laparoendosc Surg. 1993 Oct;3(5):439–453. doi: 10.1089/lps.1993.3.439. [DOI] [PubMed] [Google Scholar]
- Meguid M. M., Campos A. C., Hammond W. G. Nutritional support in surgical practice: Part II. Am J Surg. 1990 Apr;159(4):427–443. doi: 10.1016/s0002-9610(05)81290-5. [DOI] [PubMed] [Google Scholar]
- Meltvedt R., Jr, Knecht B., Gibbons G., Stahler C., Stojowski A., Johansen K. Is nasogastric suction necessary after elective colon resection? Am J Surg. 1985 May;149(5):620–622. doi: 10.1016/s0002-9610(85)80140-9. [DOI] [PubMed] [Google Scholar]
- Milsom J. W., Lavery I. C., Böhm B., Fazio V. W. Laparoscopically assisted ileocolectomy in Crohn's disease. Surg Laparosc Endosc. 1993 Apr;3(2):77–80. [PubMed] [Google Scholar]
- Monson J. R., Darzi A., Carey P. D., Guillou P. J. Prospective evaluation of laparoscopic-assisted colectomy in an unselected group of patients. Lancet. 1992 Oct 3;340(8823):831–833. doi: 10.1016/0140-6736(92)92694-b. [DOI] [PubMed] [Google Scholar]
- Moore F. A., Feliciano D. V., Andrassy R. J., McArdle A. H., Booth F. V., Morgenstein-Wagner T. B., Kellum J. M., Jr, Welling R. E., Moore E. E. Early enteral feeding, compared with parenteral, reduces postoperative septic complications. The results of a meta-analysis. Ann Surg. 1992 Aug;216(2):172–183. doi: 10.1097/00000658-199208000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Musser D. J., Boorse R. C., Madera F., Reed J. F., 3rd Laparoscopic colectomy: at what cost? Surg Laparosc Endosc. 1994 Feb;4(1):1–5. [PubMed] [Google Scholar]
- Nathan B. N., Pain J. A. Nasogastric suction after elective abdominal surgery: a randomised study. Ann R Coll Surg Engl. 1991 Sep;73(5):291–294. [PMC free article] [PubMed] [Google Scholar]
- Peters W. R., Bartels T. L. Minimally invasive colectomy: are the potential benefits realized? Dis Colon Rectum. 1993 Aug;36(8):751–756. doi: 10.1007/BF02048366. [DOI] [PubMed] [Google Scholar]
- Petrelli N. J., Stulc J. P., Rodriguez-Bigas M., Blumenson L. Nasogastric decompression following elective colorectal surgery: a prospective randomized study. Am Surg. 1993 Oct;59(10):632–635. [PubMed] [Google Scholar]
- Phillips E. H., Franklin M., Carroll B. J., Fallas M. J., Ramos R., Rosenthal D. Laparoscopic colectomy. Ann Surg. 1992 Dec;216(6):703–707. doi: 10.1097/00000658-199212000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quattlebaum J. K., Jr, Flanders H. D., Usher C. H., 3rd Laparoscopically assisted colectomy. Surg Laparosc Endosc. 1993 Apr;3(2):81–87. [PubMed] [Google Scholar]
- ROTHNIE N. G., HARPER R. A., CATCHPOLE B. N. Early postoperative gastrointestinal activity. Lancet. 1963 Jul 13;2(7298):64–67. doi: 10.1016/s0140-6736(63)90064-3. [DOI] [PubMed] [Google Scholar]
- Ryan J. A., Jr, Page C. P., Babcock L. Early postoperative jejunal feeding of elemental diet in gastrointestinal surgery. Am Surg. 1981 Sep;47(9):393–403. [PubMed] [Google Scholar]
- Scoggin S. D., Frazee R. C., Snyder S. K., Hendricks J. C., Roberts J. W., Symmonds R. E., Smith R. W. Laparoscopic-assisted bowel surgery. Dis Colon Rectum. 1993 Aug;36(8):747–750. doi: 10.1007/BF02048365. [DOI] [PubMed] [Google Scholar]
- Senagore A. J., Luchtefeld M. A., Mackeigan J. M., Mazier W. P. Open colectomy versus laparoscopic colectomy: are there differences? Am Surg. 1993 Aug;59(8):549–554. [PubMed] [Google Scholar]
- Tate J. J., Kwok S., Dawson J. W., Lau W. Y., Li A. K. Prospective comparison of laparoscopic and conventional anterior resection. Br J Surg. 1993 Nov;80(11):1396–1398. doi: 10.1002/bjs.1800801113. [DOI] [PubMed] [Google Scholar]
- Van Ye T. M., Cattey R. P., Henry L. G. Laparoscopically assisted colon resections compare favorably with open technique. Surg Laparosc Endosc. 1994 Feb;4(1):25–31. [PubMed] [Google Scholar]
- Vara-Thorbeck C., Garcia-Caballero M., Salvi M., Gutstein D., Toscano R., Gómez A., Vara-Thorbeck R. Indications and advantages of laparoscopy-assisted colon resection for carcinoma in elderly patients. Surg Laparosc Endosc. 1994 Apr;4(2):110–118. [PubMed] [Google Scholar]
- Wexner S. D., Cohen S. M., Johansen O. B., Nogueras J. J., Jagelman D. G. Laparoscopic colorectal surgery: a prospective assessment and current perspective. Br J Surg. 1993 Dec;80(12):1602–1605. doi: 10.1002/bjs.1800801238. [DOI] [PubMed] [Google Scholar]
- Wexner S. D., Johansen O. B. Laparoscopic bowel resection: advantages and limitations. Ann Med. 1992 Apr;24(2):105–110. doi: 10.3109/07853899209148335. [DOI] [PubMed] [Google Scholar]
- Wexner S. D., Johansen O. B., Nogueras J. J., Jagelman D. G. Laparoscopic total abdominal colectomy. A prospective trial. Dis Colon Rectum. 1992 Jul;35(7):651–655. doi: 10.1007/BF02053755. [DOI] [PubMed] [Google Scholar]
- Woods J. H., Erickson L. W., Condon R. E., Schulte W. J., Sillin L. F. Postoperative ileus: a colonic problem? Surgery. 1978 Oct;84(4):527–533. [PubMed] [Google Scholar]
- Zucker K. A., Pitcher D. E., Martin D. T., Ford R. S. Laparoscopic-assisted colon resection. Surg Endosc. 1994 Jan;8(1):12–18. doi: 10.1007/BF02909486. [DOI] [PubMed] [Google Scholar]