

Abstract
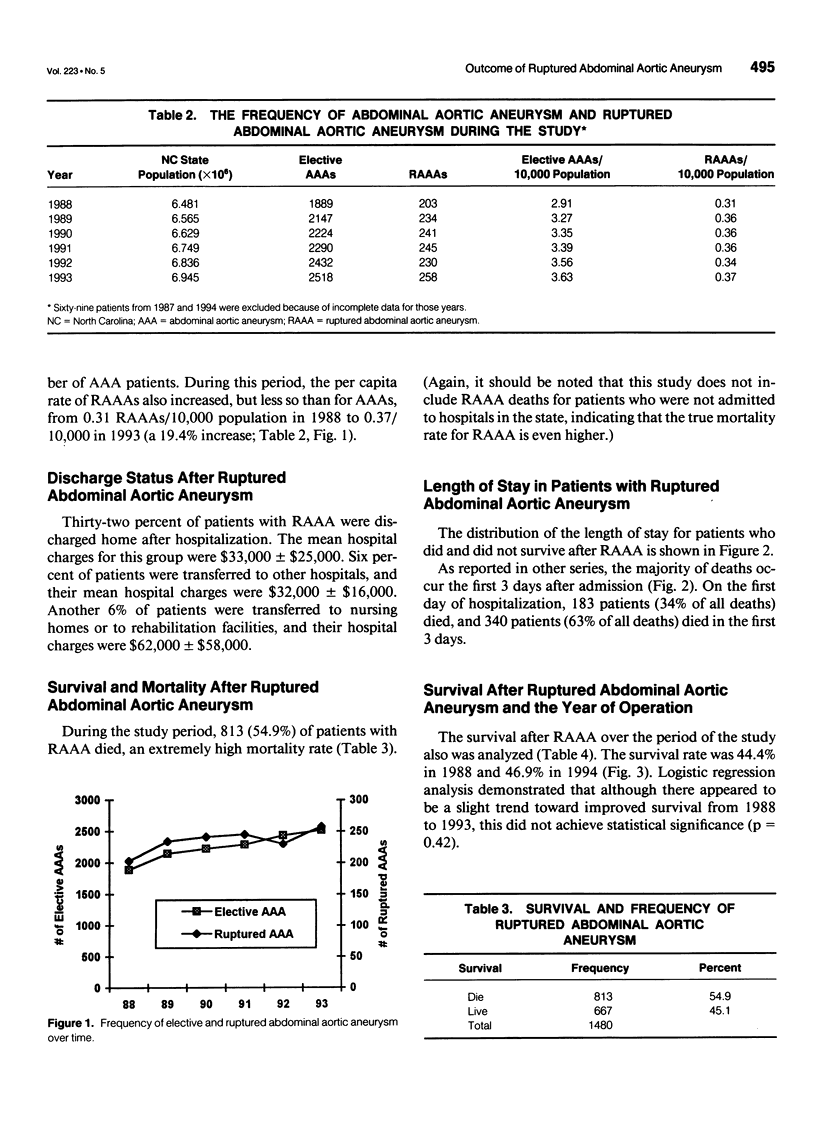
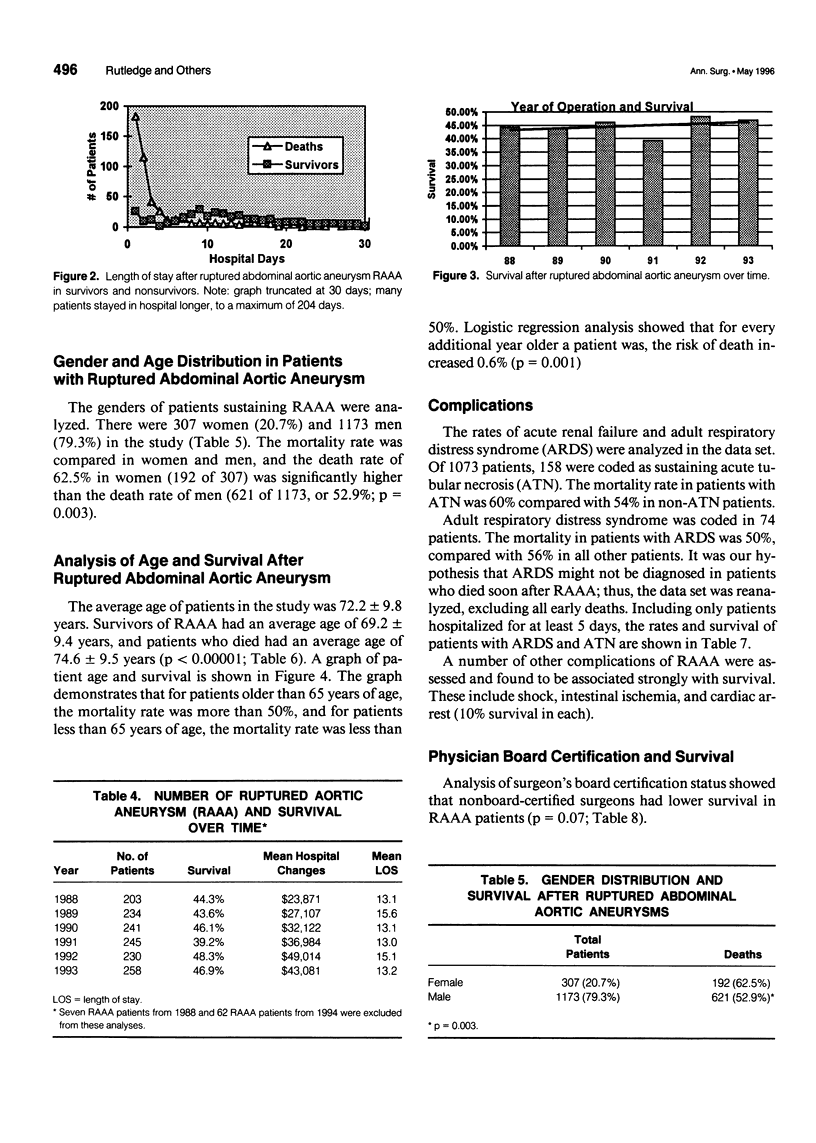
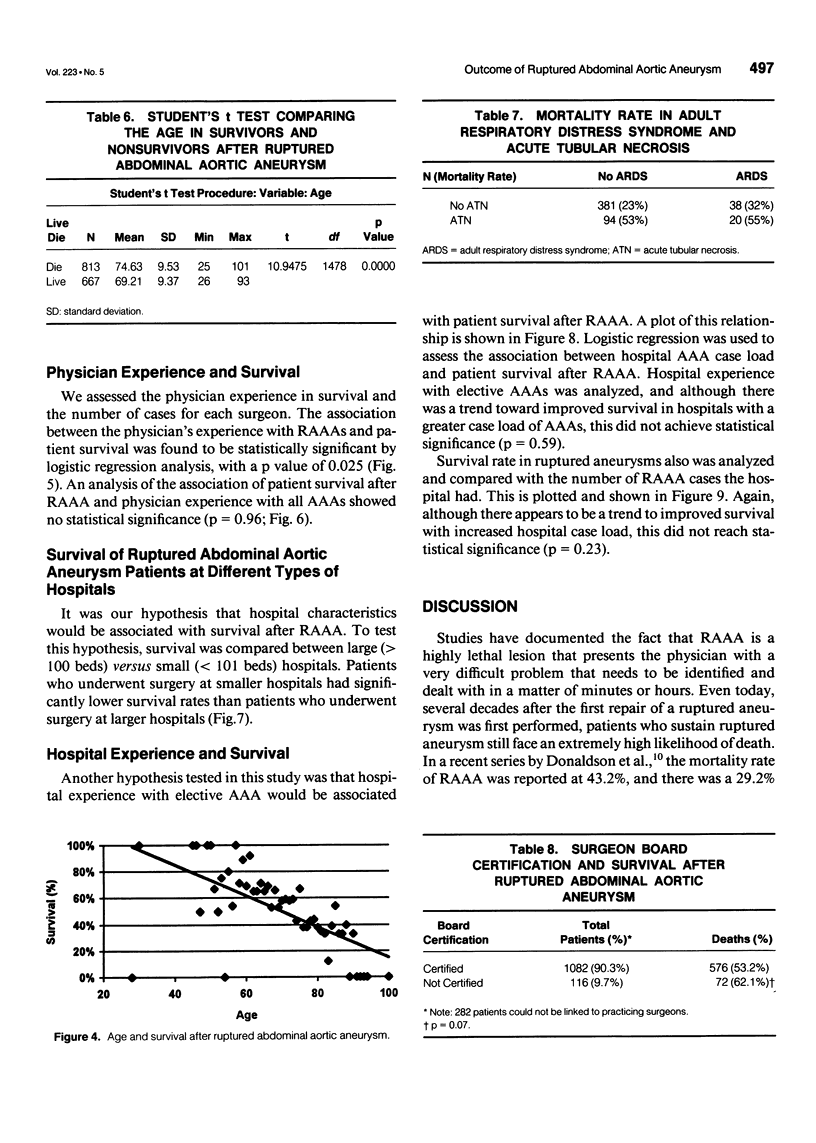
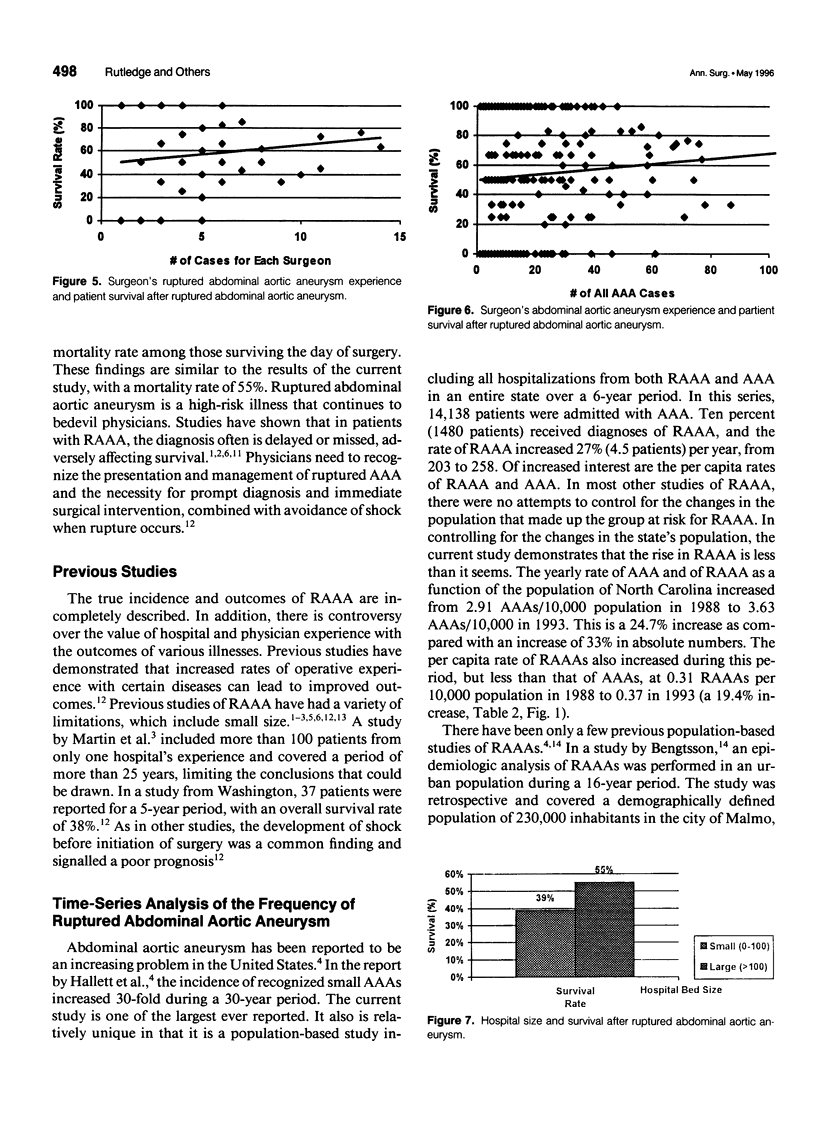
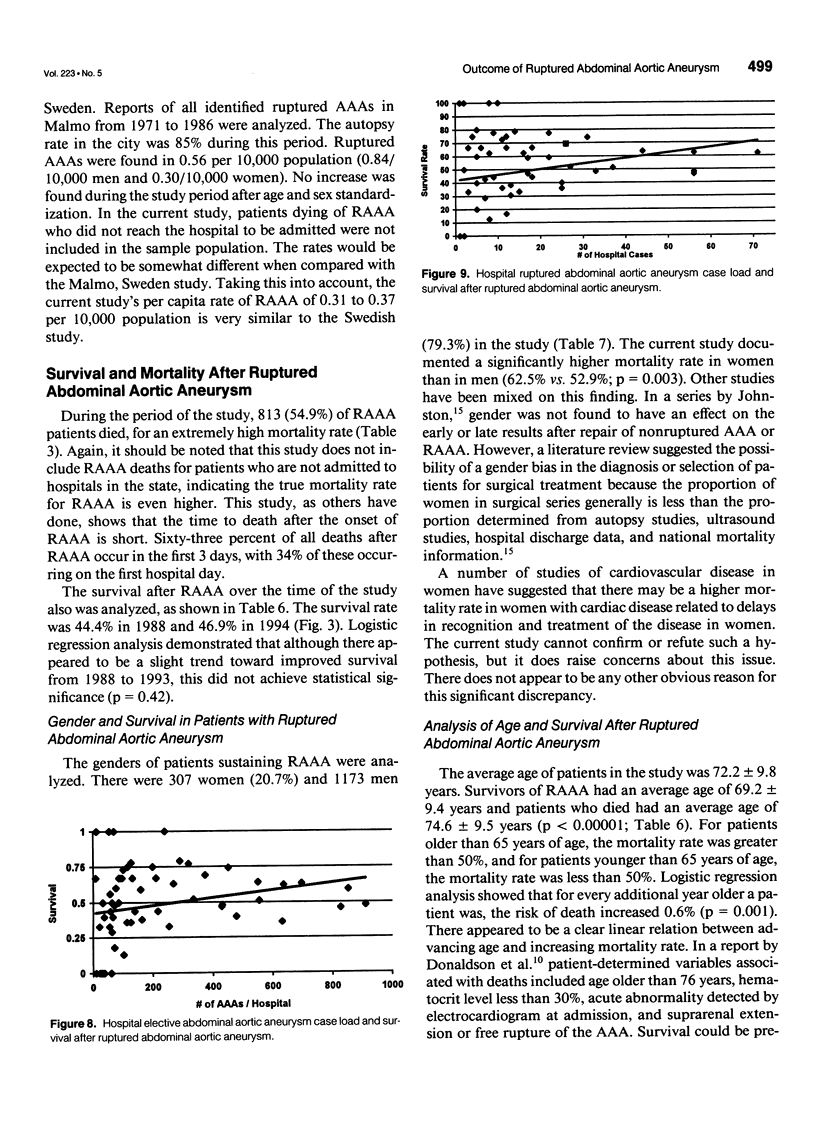
OBJECTIVES: The purpose of this study was to perform the first statewide, population-based, time-series analysis of the frequency of ruptured abdominal aortic aneurysm (RAAA), to determine the outcomes of RAAA, and to assess the association of patient, physician, and hospital factors with survival after RAAA. The hypotheses of the study were as follows: 1) the rate of RAAA would increase over time and 2) patient, surgeon, and hospital factors would be associated with survival. BACKGROUND: Ruptured abdominal aortic aneurysm is a life-threatening emergency that presents the surgeon with a technically demanding challenge that must be met and surmounted in a short time if the patient is to survive. METHODS: Data were obtained from the following four separate data sources: 1) the North Carolina Hospital Discharge database, 2) the North Carolina American Hospital Association database, 3) the North Carolina State Medical Examiner's database, and 4) the Area Resource File. All patients with the diagnosis of an abdominal aortic aneurysm (AAA) were selected for initial assessment. Patients were grouped into those with and those without rupture of the abdominal aneurysm. RESULTS: During the 6 years of the study, 14,138 patients were admitted with a diagnosis of AAA. Of these, 1480 (10%) had an RAAA. The yearly number of patients with elective AAAs increased 33% from 1889 in 1988 to 2518 in 1993. The yearly number of RAAAs increased 27% from 203 to 258. The mortality rate for AAA was 5%, as compared with 54% in RAAA patients. The patient's age was found to be the most powerful predictor of survival. Univariate logistic regression analyses demonstrated an association of the surgeon's experience with RAAA and patient survival after RAAA. Analysis of the survival rates of board-certified and nonboard-certified surgeons demonstrated that patients with RAAAs who were treated by board-certified surgeons had significantly better survival. When the survival was compared in small (less than 100 beds) and large (more than 100 beds) hospitals, survival was significantly better in the larger hospitals. CONCLUSIONS: Ruptured abdominal aortic aneurysm remains a highly lethal lesion, even in the best of hands. Despite the many improvements in the care of seriously ill patients, there was no significant improvement in the survival of RAAA during this study. This suggests that early diagnosis is the best hope of survival in these patients. The study demonstrated that survival after RAAA was related most strongly to patient age at the time of the RAAA. The physician's and the hospital's experience with RAAA, the physician's background as measured by board certification, and the type of hospital at which the operation was performed (small vs. large) also may be associated with survival. These findings may have important implications for the regionalization of care and the education and credentialling of physicians. Given the lack of recent progress of improving the outcome of RAAA, aggressive efforts to treat patients before rupture are appropriate.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bengtsson H., Bergqvist D. Ruptured abdominal aortic aneurysm: a population-based study. J Vasc Surg. 1993 Jul;18(1):74–80. doi: 10.1067/mva.1993.42107. [DOI] [PubMed] [Google Scholar]
- Bodily K. C., Buttorff J. D. Ruptured abdominal aortic aneurysm. The Tacoma experience. Am J Surg. 1985 May;149(5):580–582. doi: 10.1016/s0002-9610(85)80129-x. [DOI] [PubMed] [Google Scholar]
- Bradbury A. W., Bachoo P., Milne A. A., Duncan J. L. Platelet count and the outcome of operation for ruptured abdominal aortic aneurysm. J Vasc Surg. 1995 Mar;21(3):484–491. doi: 10.1016/s0741-5214(95)70291-1. [DOI] [PubMed] [Google Scholar]
- Donaldson M. C., Rosenberg J. M., Bucknam C. A. Factors affecting survival after ruptured abdominal aortic aneurysm. J Vasc Surg. 1985 Jul;2(4):564–570. [PubMed] [Google Scholar]
- Hallett J. W., Jr, Naessens J. M., Ballard D. J. Early and late outcome of surgical repair for small abdominal aortic aneurysms: a population-based analysis. J Vasc Surg. 1993 Oct;18(4):684–691. [PubMed] [Google Scholar]
- Hiatt J. C., Barker W. F., Machleder H. I., Baker J. D., Busuttil R. W., Moore W. S. Determinants of failure in the treatment of ruptured abdominal aortic aneurysm. Arch Surg. 1984 Nov;119(11):1264–1268. doi: 10.1001/archsurg.1984.01390230036008. [DOI] [PubMed] [Google Scholar]
- Johansen K., Kohler T. R., Nicholls S. C., Zierler R. E., Clowes A. W., Kazmers A. Ruptured abdominal aortic aneurysm: the Harborview experience. J Vasc Surg. 1991 Feb;13(2):240–247. [PubMed] [Google Scholar]
- Johnston K. W. Influence of sex on the results of abdominal aortic aneurysm repair. Canadian Society for Vascular Surgery Aneurysm Study Group. J Vasc Surg. 1994 Dec;20(6):914–926. doi: 10.1016/0741-5214(94)90228-3. [DOI] [PubMed] [Google Scholar]
- Lederle F. A., Parenti C. M., Chute E. P. Ruptured abdominal aortic aneurysm: the internist as diagnostician. Am J Med. 1994 Feb;96(2):163–167. doi: 10.1016/0002-9343(94)90137-6. [DOI] [PubMed] [Google Scholar]
- Martin R. S., 3rd, Edwards W. H., Jr, Jenkins J. M., Edwards W. H., Sr, Mulherin J. L. Ruptured abdominal aortic aneurysm: a 25-year experience and analysis of recent cases. Am Surg. 1988 Sep;54(9):539–543. [PubMed] [Google Scholar]
- Maupin G. E., Rimar S. D., Villalba M. Ischemic colitis following abdominal aortic reconstruction for ruptured aneurysm. A 10-year experience. Am Surg. 1989 Jun;55(6):378–380. [PubMed] [Google Scholar]
- Munoz E., Kassan M. A., Chang J. B. Surgonomics: the costs of ruptured abdominal aortic aneurysm. Angiology. 1988 Sep;39(9):830–837. doi: 10.1177/000331978803900907. [DOI] [PubMed] [Google Scholar]
- Patsey T., Messick J., Rutledge R., Meyer A., Butts J. M., Baker C. A population-based, multivariate analysis of the association between 911 access and per-capita county trauma death rates. Ann Emerg Med. 1992 Oct;21(10):1173–1178. doi: 10.1016/s0196-0644(05)81741-x. [DOI] [PubMed] [Google Scholar]
- Previti F. W., Onopchenko A., Glick B. The ruptured abdominal aortic aneurysm in a community hospital. A 5-year study. Am Surg. 1992 Aug;58(8):499–501. [PubMed] [Google Scholar]
- Rutledge R., Fakhry S. M., Meyer A., Sheldon G. F., Baker C. C. An analysis of the association of trauma centers with per capita hospitalizations and death rates from injury. Ann Surg. 1993 Oct;218(4):512–524. doi: 10.1097/00000658-199310000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rutledge R., Hunt J. P., Lentz C. W., Fakhry S. M., Meyer A. A., Baker C. C., Sheldon G. F. A statewide, population-based time-series analysis of the increasing frequency of nonoperative management of abdominal solid organ injury. Ann Surg. 1995 Sep;222(3):311–326. doi: 10.1097/00000658-199509000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scott R. A., Wilson N. M., Ashton H. A., Kay D. N. Influence of screening on the incidence of ruptured abdominal aortic aneurysm: 5-year results of a randomized controlled study. Br J Surg. 1995 Aug;82(8):1066–1070. doi: 10.1002/bjs.1800820821. [DOI] [PubMed] [Google Scholar]
- Seiwert A. J., Elmore J. R., Youkey J. R., Franklin D. P. Peter B. Samuels Award. Ruptured abdominal aortic aneurysm repair: the financial analysis. Am J Surg. 1995 Aug;170(2):91–96. doi: 10.1016/s0002-9610(99)80262-1. [DOI] [PubMed] [Google Scholar]
- Shackleton C. R., Schechter M. T., Bianco R., Hildebrand H. D. Preoperative predictors of mortality risk in ruptured abdominal aortic aneurysm. J Vasc Surg. 1987 Dec;6(6):583–589. doi: 10.1067/mva.1987.avs0060583. [DOI] [PubMed] [Google Scholar]
- Siegel C. L., Cohan R. H., Korobkin M., Alpern M. B., Courneya D. L., Leder R. A. Abdominal aortic aneurysm morphology: CT features in patients with ruptured and nonruptured aneurysms. AJR Am J Roentgenol. 1994 Nov;163(5):1123–1129. doi: 10.2214/ajr.163.5.7976888. [DOI] [PubMed] [Google Scholar]