

Abstract
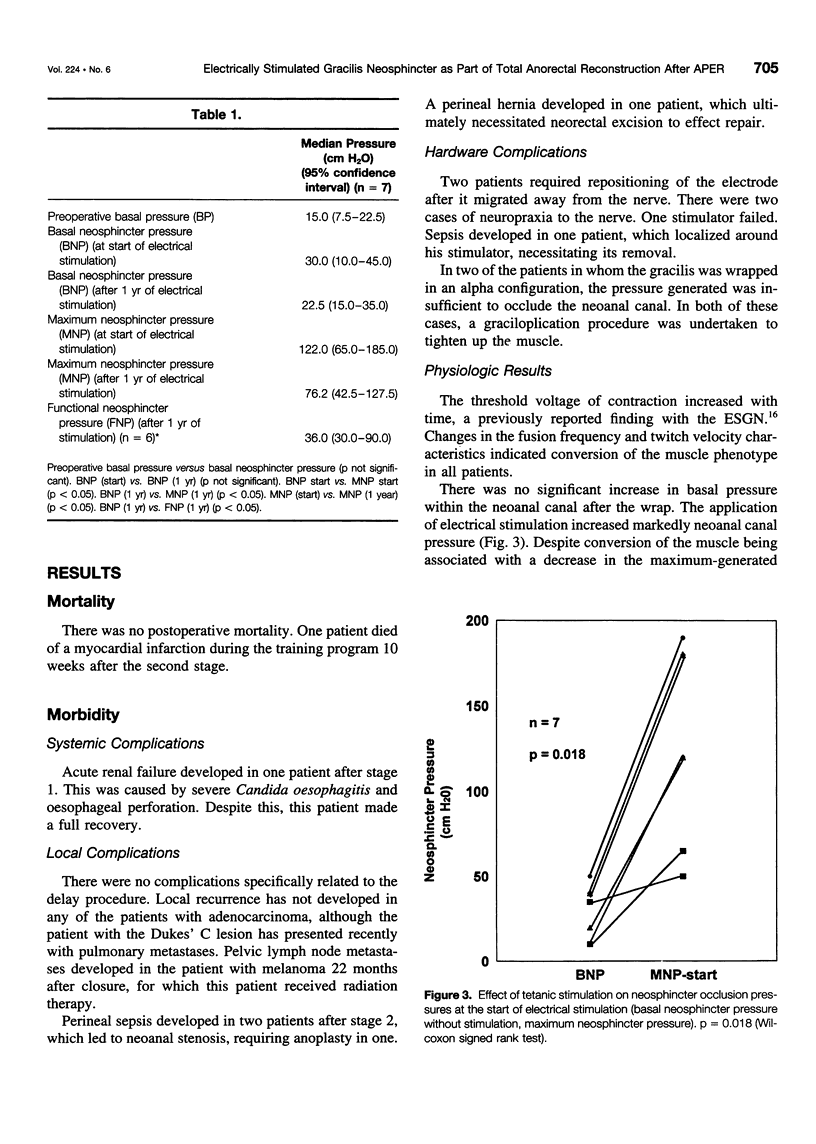
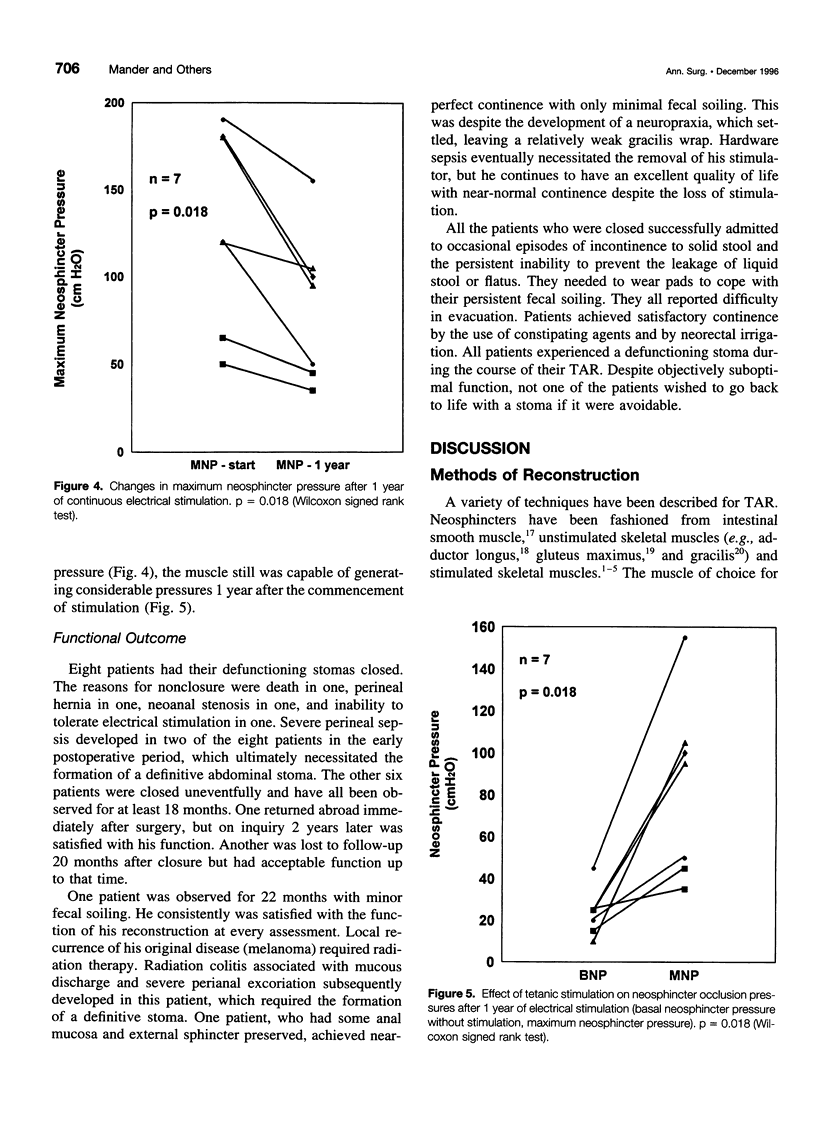
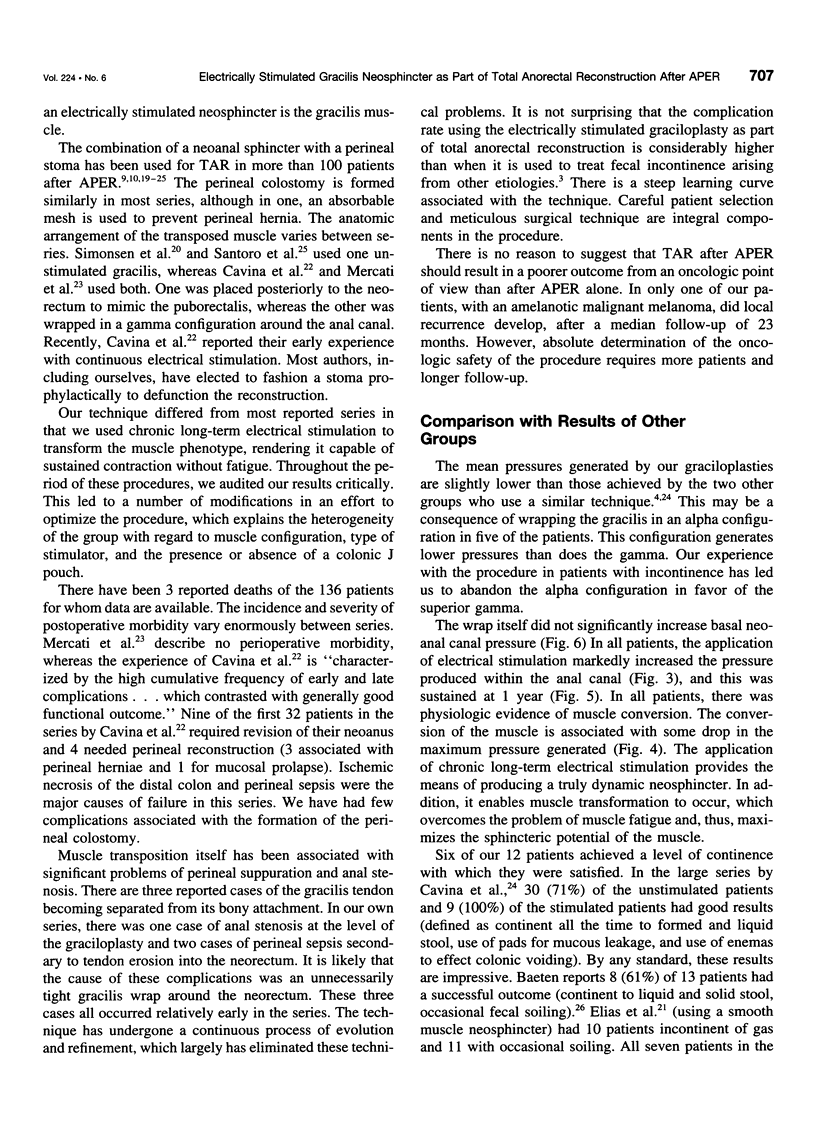
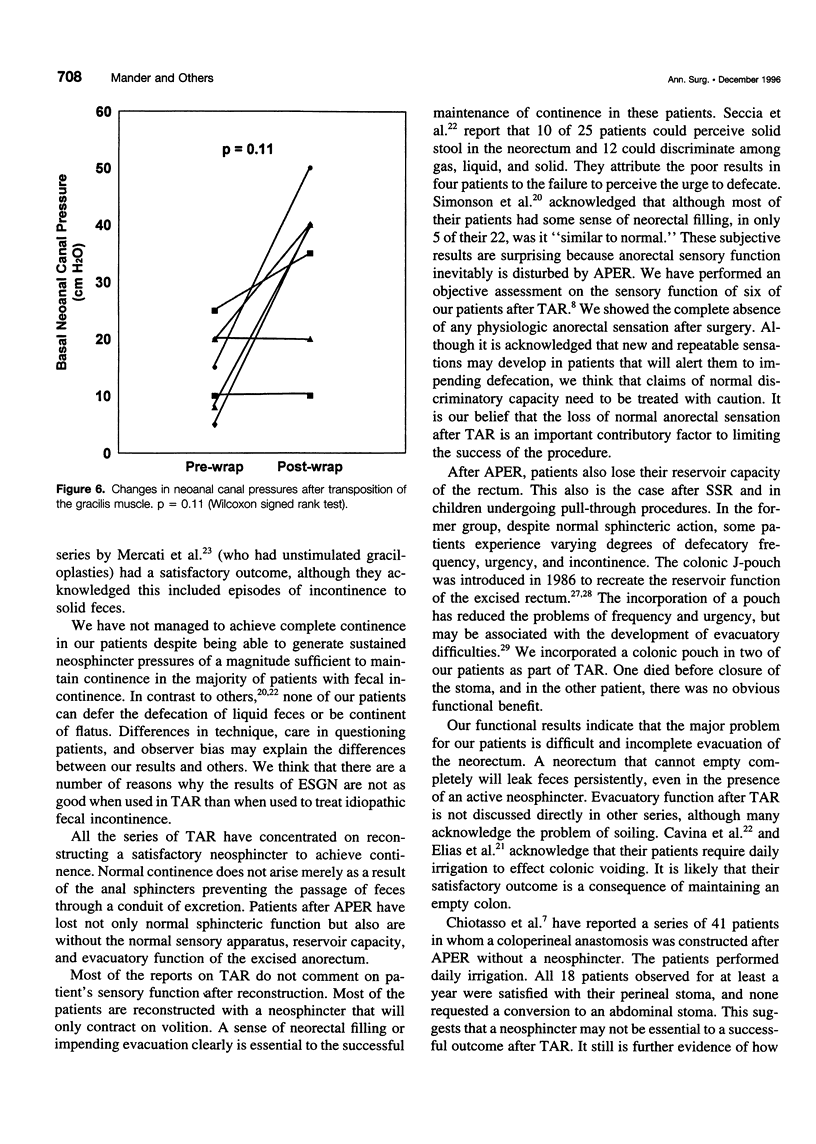
OBJECTIVE: The authors investigated the feasibility and effectiveness of combining electrically stimulated gracilis neoanal (ESGN) sphincter and a coloperineal anastomosis in selected patients after abdominoperineal excision of the rectum (APER). SUMMARY BACKGROUND DATA: The ESGN is effective in the treatment of idiopathic fecal incontinence. METHODS: Between March 1989 and September 1993, 12 patients (9 men, 3 women) with a median age of 59.25 years (range, 45-70) underwent the procedure. The underlying disease was adenocarcinoma in 10, anal malignant melanoma in 1, and a sweat gland tumor in the other. In all patients, a sphincter saving resection was contraindicated. The procedure was performed in stages. Stage 1 involved a conventional APER with the formation of a perineal stoma. Eleven patients underwent a vascular delay procedure. All patients were defunctioned. In stage 2, the gracilis was mobilized, transposed around the anal canal, and the electrodes and hardware needed for electrical stimulation were implanted. Once muscle conversion was complete, the defunctioning stoma was closed. RESULTS: Eight patients were closed successfully. In seven of the eight patients, complete physiologic measurements were taken. Median basal and maximum neosphincter pressures were 30 and 122 cm H2O, respectively, at the start of electrical stimulation and 22.5 and 76.2 cm H2O, respectively, after 1 year. Median functioning neosphincter pressure was 36 cm H2O at 1 year. All of the patients whose stomas were closed experienced episodes of incontinence to solid stool and wore pads for persistent fecal soiling. They all reported difficulty in evacuation. Despite imperfect continence, no patient wished to go back to life with a stoma. CONCLUSIONS: The incorporation of ESGN as part of total anorectal reconstruction is technically feasible. The majority of patients are satisfied with their function and pleased to avoid a permanent stoma.
Full text
PDF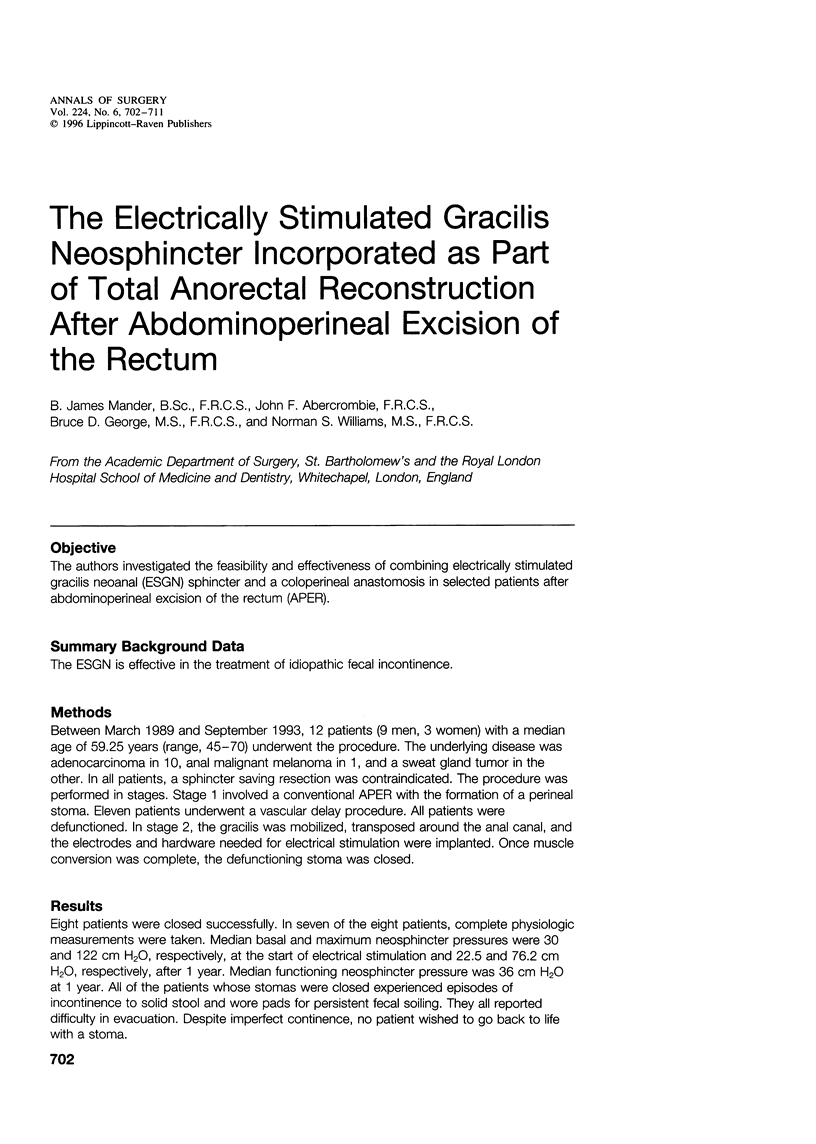
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Abercrombie J. F., Rogers J., Williams N. S. Total anorectal reconstruction results in complete anorectal sensory loss. Br J Surg. 1996 Jan;83(1):57–59. doi: 10.1002/bjs.1800830118. [DOI] [PubMed] [Google Scholar]
- Abercrombie J. F., Williams N. S. Development of an electrically-stimulated skeletal muscle neoanal sphincter. Baillieres Clin Neurol. 1995 Apr;4(1):21–34. [PubMed] [Google Scholar]
- Baeten C. G., Konsten J., Spaans F., Visser R., Habets A. M., Bourgeois I. M., Wagenmakers A. J., Soeters P. B. Dynamic graciloplasty for treatment of faecal incontinence. Lancet. 1991 Nov 9;338(8776):1163–1165. doi: 10.1016/0140-6736(91)92030-6. [DOI] [PubMed] [Google Scholar]
- Baeten C., Spaans F., Fluks A. An implanted neuromuscular stimulator for fecal continence following previously implanted gracilis muscle. Report of a case. Dis Colon Rectum. 1988 Feb;31(2):134–137. doi: 10.1007/BF02562646. [DOI] [PubMed] [Google Scholar]
- Cavina E., Seccia M., Evangelista G., Chiarugi M., Buccianti P., Chirico A., Lenzi M., Bortolotti P., Bellomini G., Arganini M. Construction of a continent perineal colostomy by using electrostimulated gracilis muscles after abdominoperineal resection: personal technique and experience with 32 cases. Ital J Surg Sci. 1987;17(4):305–314. [PubMed] [Google Scholar]
- Elias D., Lasser P., Leroux A., Rougier P., Comandella M. G., Deraco M. Colostomies périnéales pseudo-continentes après amputation rectale pour cancer. Gastroenterol Clin Biol. 1993;17(3):181–186. [PubMed] [Google Scholar]
- Federov V. D., Odaryuk T. S., Shelygin Y. A., Tsarkov P. V., Frolov S. A. Method of creation of a smooth-muscle cuff at the site of the perineal colostomy after extirpation of the rectum. Dis Colon Rectum. 1989 Jul;32(7):562–566. doi: 10.1007/BF02554174. [DOI] [PubMed] [Google Scholar]
- Fedorov V. D., Shelygin Y. A. Treatment of patients with rectal cancer. Dis Colon Rectum. 1989 Feb;32(2):138–145. doi: 10.1007/BF02553827. [DOI] [PubMed] [Google Scholar]
- Geerdes B. P., Zoetmulder F. A., Baeten C. G. Double dynamic graciloplasty and coloperineal pull-through after abdominoperineal resection. Eur J Cancer. 1995 Jul-Aug;31A(7-8):1248–1252. doi: 10.1016/0959-8049(95)00173-g. [DOI] [PubMed] [Google Scholar]
- George B. D., Williams N. S., Patel J., Swash M., Watkins E. S. Physiological and histochemical adaptation of the electrically stimulated gracilis muscle to neoanal sphincter function. Br J Surg. 1993 Oct;80(10):1342–1346. doi: 10.1002/bjs.1800801042. [DOI] [PubMed] [Google Scholar]
- Hughes S. F., Williams N. S. Continent colonic conduit for the treatment of faecal incontinence associated with disordered evacuation. Br J Surg. 1995 Oct;82(10):1318–1320. doi: 10.1002/bjs.1800821008. [DOI] [PubMed] [Google Scholar]
- Konsten J., Baeten C. G., Spaans F., Havenith M. G., Soeters P. B. Follow-up of anal dynamic graciloplasty for fecal continence. World J Surg. 1993 May-Jun;17(3):404–409. doi: 10.1007/BF01658712. [DOI] [PubMed] [Google Scholar]
- Lazorthes F., Fages P., Chiotasso P., Lemozy J., Bloom E. Resection of the rectum with construction of a colonic reservoir and colo-anal anastomosis for carcinoma of the rectum. Br J Surg. 1986 Feb;73(2):136–138. doi: 10.1002/bjs.1800730222. [DOI] [PubMed] [Google Scholar]
- Mercati U., Trancanelli V., Castagnoli G. P., Mariotti A., Ciaccarini R. Use of the gracilis muscles for sphincteric construction after abdominoperineal resection. Technique and preliminary results. Dis Colon Rectum. 1991 Dec;34(12):1085–1089. doi: 10.1007/BF02050066. [DOI] [PubMed] [Google Scholar]
- Parc R., Tiret E., Frileux P., Moszkowski E., Loygue J. Resection and colo-anal anastomosis with colonic reservoir for rectal carcinoma. Br J Surg. 1986 Feb;73(2):139–141. doi: 10.1002/bjs.1800730223. [DOI] [PubMed] [Google Scholar]
- Pélissier E. P., Blum D., Bachour A., Bosset J. F. Functional results of coloanal anastomosis with reservoir. Dis Colon Rectum. 1992 Sep;35(9):843–846. doi: 10.1007/BF02047870. [DOI] [PubMed] [Google Scholar]
- Salmons S., Vrbová G. The influence of activity on some contractile characteristics of mammalian fast and slow muscles. J Physiol. 1969 May;201(3):535–549. doi: 10.1113/jphysiol.1969.sp008771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Santoro E., Tirelli C., Scutari F., Garofalo A., Silecchia G., Scaccia M., Santoro E. Continent perineal colostomy by transposition of gracilis muscles. Technical remarks and results in 14 cases. Dis Colon Rectum. 1994 Feb;37(2 Suppl):S73–S80. doi: 10.1007/BF02048436. [DOI] [PubMed] [Google Scholar]
- Seccia M., Menconi C., Balestri R., Cavina E. Study protocols and functional results in 86 electrostimulated graciloplasties. Dis Colon Rectum. 1994 Sep;37(9):897–904. doi: 10.1007/BF02052595. [DOI] [PubMed] [Google Scholar]
- Simonsen O. S., Stolf N. A., Aun F., Raia A., Habr-Gama A. Rectal sphincter reconstruction in perineal colostomies after abdominoperineal resection for cancer. Br J Surg. 1976 May;63(5):389–391. doi: 10.1002/bjs.1800630514. [DOI] [PubMed] [Google Scholar]
- Willams N. S., Hallan R. I., Koeze T. H., Pilot M. A., Watkins E. S. Construction of a neoanal sphincter by transposition of the gracilis muscle and prolonged neuromuscular stimulation for the treatment of faecal incontinence. Ann R Coll Surg Engl. 1990 Mar;72(2):108–113. [PMC free article] [PubMed] [Google Scholar]
- Williams N. S., Hallan R. I., Koeze T. H., Watkins E. S. Construction of a neorectum and neoanal sphincter following previous proctocolectomy. Br J Surg. 1989 Nov;76(11):1191–1194. doi: 10.1002/bjs.1800761124. [DOI] [PubMed] [Google Scholar]
- Williams N. S., Hallan R. I., Koeze T. H., Watkins E. S. Restoration of gastrointestinal continuity and continence after abdominoperineal excision of the rectum using an electrically stimulated neoanal sphincter. Dis Colon Rectum. 1990 Jul;33(7):561–565. doi: 10.1007/BF02052207. [DOI] [PubMed] [Google Scholar]
- Williams N. S., Hughes S. F., Stuchfield B. Continent colonic conduit for rectal evacuation in severe constipation. Lancet. 1994 May 28;343(8909):1321–1324. doi: 10.1016/s0140-6736(94)92467-8. [DOI] [PubMed] [Google Scholar]
- Williams N. S., Patel J., George B. D., Hallan R. I., Watkins E. S. Development of an electrically stimulated neoanal sphincter. Lancet. 1991 Nov 9;338(8776):1166–1169. doi: 10.1016/0140-6736(91)92031-v. [DOI] [PubMed] [Google Scholar]