

Abstract
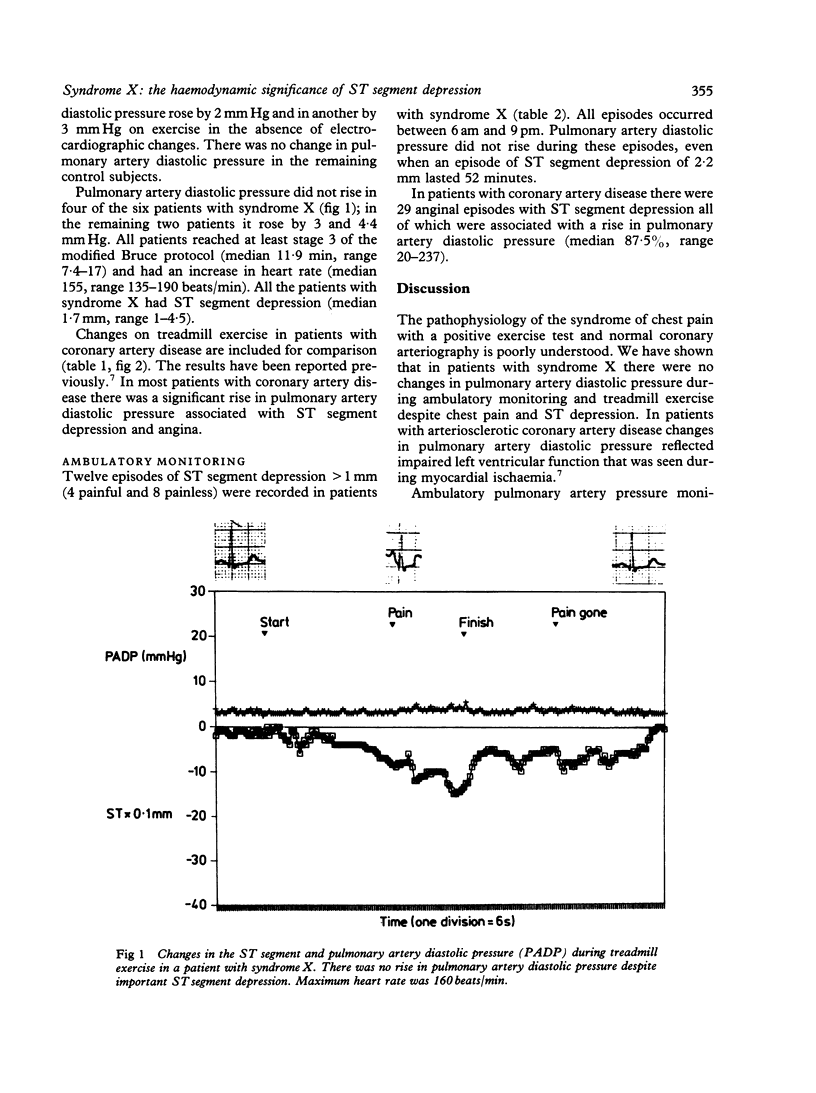
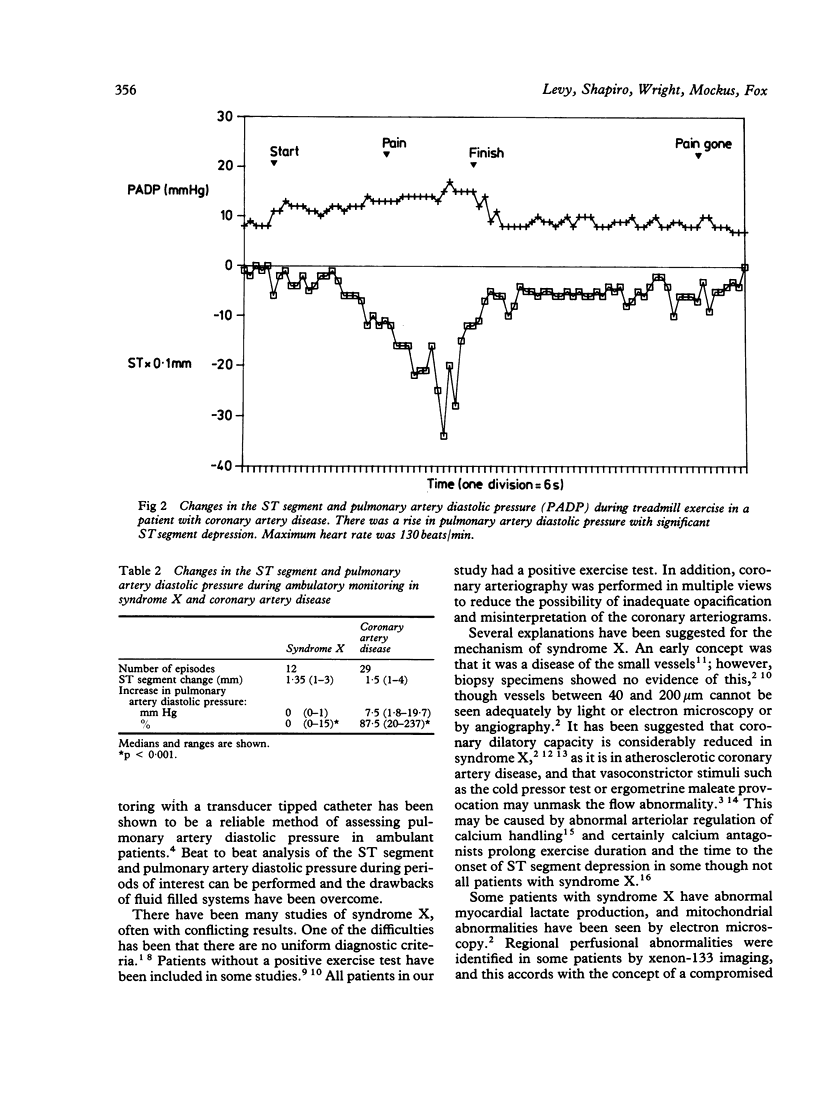
The relation between chest pain, ST segment depression, and changes in left ventricular function was assessed in six patients with angina, a positive exercise test, and normal coronary arteries as assessed by arteriography (syndrome X). In the six patients with syndrome X and in six controls there was no significant rise in pulmonary artery diastolic pressure during treadmill exercise, although there was ST segment depression (range 1-4.5 mm) in the patients with syndrome X. In 19 patients with coronary artery disease, however, the pulmonary artery diastolic pressure increased by a median 5 mm Hg (range 0-13.6 mm Hg) on treadmill exercise. In only one patient with coronary artery disease, who showed 1 mm ST segment depression, was there no rise in pulmonary artery diastolic pressure. During ambulatory monitoring in patients with syndrome X there were 12 episodes of ST segment depression (greater than 1 mm) (4 painful, 8 painless) in which there was no change in pulmonary artery diastolic pressure. In the patients with coronary artery disease there were 29 episodes of angina during ambulatory monitoring and during all of them pulmonary artery diastolic pressure rose by a median 7.5 mm Hg (range 1.8-19.7 mm Hg). Unlike the haemodynamic changes that usually occur during myocardial ischaemia in coronary artery disease, chest pain and ST segment changes in patients with syndrome X are not associated with impaired left ventricular function as assessed by ambulatory pulmonary artery pressure monitoring.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BRUCE R. A., BLACKMON J. R., JONES J. W., STRAIT G. EXERCISING TESTING IN ADULT NORMAL SUBJECTS AND CARDIAC PATIENTS. Pediatrics. 1963 Oct;32:SUPPL–756. [PubMed] [Google Scholar]
- Bemiller C. R., Pepine C. J., Rogers A. K. Long-term observations in patients with angina and normal coronary arteriograms. Circulation. 1973 Jan;47(1):36–43. doi: 10.1161/01.cir.47.1.36. [DOI] [PubMed] [Google Scholar]
- Cannon R. O., 3rd, Bonow R. O., Bacharach S. L., Green M. V., Rosing D. R., Leon M. B., Watson R. M., Epstein S. E. Left ventricular dysfunction in patients with angina pectoris, normal epicardial coronary arteries, and abnormal vasodilator reserve. Circulation. 1985 Feb;71(2):218–226. doi: 10.1161/01.cir.71.2.218. [DOI] [PubMed] [Google Scholar]
- Cannon R. O., 3rd, Watson R. M., Rosing D. R., Epstein S. E. Efficacy of calcium channel blocker therapy for angina pectoris resulting from small-vessel coronary artery disease and abnormal vasodilator reserve. Am J Cardiol. 1985 Aug 1;56(4):242–246. doi: 10.1016/0002-9149(85)90842-2. [DOI] [PubMed] [Google Scholar]
- Dwyer E. M., Jr, Wiener L., Cox J. W. Angina pectoris in patients with normal and abnormal coronary arteriograms. Am J Cardiol. 1969 May;23(5):639–646. doi: 10.1016/0002-9149(69)90024-1. [DOI] [PubMed] [Google Scholar]
- James T. N. Pathology of small coronary arteries. Am J Cardiol. 1967 Nov;20(5):679–691. doi: 10.1016/0002-9149(67)90012-4. [DOI] [PubMed] [Google Scholar]
- Kaltman A. J., Herbert W. H., Conroy R. J., Kossmann C. E. The gradient in pressure across the pulmonary vascular bed during diastole. Circulation. 1966 Sep;34(3):377–384. doi: 10.1161/01.cir.34.3.377. [DOI] [PubMed] [Google Scholar]
- Kemp H. G., Jr Left ventricular function in patients with the anginal syndrome and normal coronary arteriograms. Am J Cardiol. 1973 Sep 7;32(3):375–376. doi: 10.1016/s0002-9149(73)80150-x. [DOI] [PubMed] [Google Scholar]
- Korhola O., Valle M., Frick M. H., Wiljasalo M., Riihimäki E. Regional myocardial perfusion abnormalities on xenon-133 imaging in patients with angina pectoris and normal coronary arteries. Am J Cardiol. 1977 Mar;39(3):355–359. doi: 10.1016/s0002-9149(77)80088-x. [DOI] [PubMed] [Google Scholar]
- Levy R. D., Cunningham D., Shapiro L. M., Wright C., Mockus L., Fox K. M. Continuous ambulatory pulmonary artery pressure monitoring. A new method using a transducer tipped catheter and a simple recording system. Br Heart J. 1986 Apr;55(4):336–343. doi: 10.1136/hrt.55.4.336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levy R. D., Shapiro L. M., Wright C., Mockus L., Fox K. M. Haemodynamic response to myocardial ischaemia during unrestricted activity, exercise testing, and atrial pacing assessed by ambulatory pulmonary artery pressure monitoring. Br Heart J. 1986 Jul;56(1):12–18. doi: 10.1136/hrt.56.1.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mammohansingh P., Parker J. O. Angina pectoris with normal coronary arteriograms: hemodynamic and metabolic response to atrial pacing. Am Heart J. 1975 Nov;90(5):555–561. doi: 10.1016/0002-8703(75)90217-3. [DOI] [PubMed] [Google Scholar]
- Opherk D., Zebe H., Weihe E., Mall G., Dürr C., Gravert B., Mehmel H. C., Schwarz F., Kübler W. Reduced coronary dilatory capacity and ultrastructural changes of the myocardium in patients with angina pectoris but normal coronary arteriograms. Circulation. 1981 Apr;63(4):817–825. doi: 10.1161/01.cir.63.4.817. [DOI] [PubMed] [Google Scholar]
- Richardson P. J., Livesley B., Oram S., Olsen E. G., Armstrong P. Angina pectoris with normal coronary arteries. Transvenous myocardial biopsy in diagnosis. Lancet. 1974 Sep 21;2(7882):677–680. doi: 10.1016/s0140-6736(74)93260-7. [DOI] [PubMed] [Google Scholar]