

Abstract
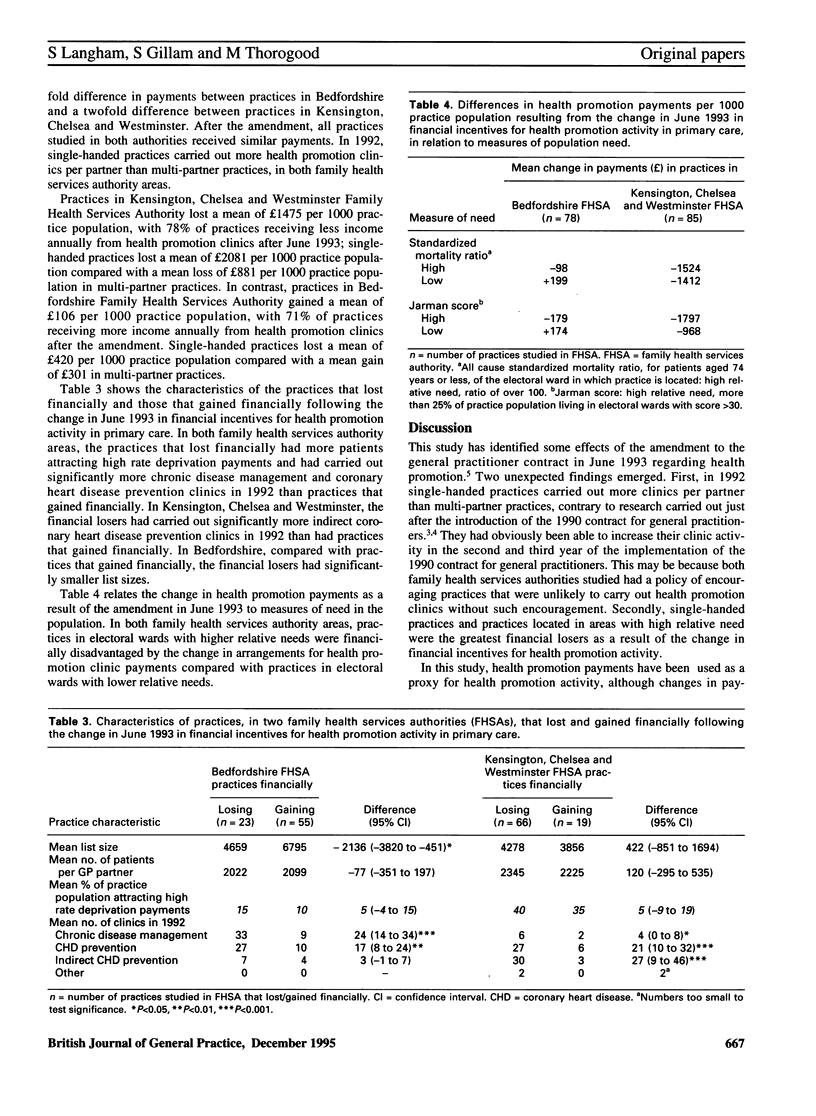
BACKGROUND: Financial incentives for increasing health promotion activity in primary care, introduced with the 1990 contract for general practitioners, were amended in 1993 and are now focused on cardiovascular disease. Payments for health promotion clinics were abolished and target payments were introduced. AIM: The study aimed to evaluate the effect of the change, in June 1993, in financial incentives for health promotion activity in primary care on the distribution of health promotion payments in two family health services authorities. METHOD: A retrospective study was undertaken in which data from two family health services authorities were used to determine the annual level of health promotion payments per 1000 practice population before and after the contractual amendment. Health promotion clinic payment data were analysed for 78 practices in Bedfordshire Family Health Services Authority and 85 practices in Kensington, Chelsea and Westminster Family Health Services Authority. Changes in health promotion payments were calculated and related to two measures of relative need: all cause standardized mortality ratios, for patients aged 74 years or less, of the electoral ward in which the practice is located; and the Jarman underprivileged area score. High relative need was defined as a standardized mortality ratio of over 100 or more than 25% of the practice population living in electoral wards with a Jarman score of over 30. RESULTS: Health promotion payments were more evenly distributed after the change in June 1993 than before between the two family health services authorities and between general practices. Single-handed practices were carrying out more clinics in 1992 than multi-partner practices and consequently were one of the greatest financial losers as a result of the change. In addition, practices located in electoral wards with high relative needs lost proportionally more than those in electoral wards with lower needs. CONCLUSION: Changes in the general practitioner health promotion contract have created new financial winners and losers. It now appears that health promotion payments are more evenly distributed but that the distribution is unrelated to need or treatment given. More evidence on the effectiveness of health promotion interventions is required before policies aimed at promoting better health through primary care can be fully evaluated.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Foy C., Hutchinson A., Smyth J. Providing census data for general practice. 2. Usefulness. J R Coll Gen Pract. 1987 Oct;37(303):451–454. [PMC free article] [PubMed] [Google Scholar]
- Gillam S. J. Provision of health promotion clinics in relation to population need: another example of the inverse care law? Br J Gen Pract. 1992 Feb;42(355):54–56. [PMC free article] [PubMed] [Google Scholar]
- Iliffe S., Munro J. General practitioners and incentives. BMJ. 1993 Nov 6;307(6913):1156–1157. doi: 10.1136/bmj.307.6913.1156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jarman B. Identification of underprivileged areas. Br Med J (Clin Res Ed) 1983 May 28;286(6379):1705–1709. doi: 10.1136/bmj.286.6379.1705. [DOI] [PMC free article] [PubMed] [Google Scholar]