

Abstract
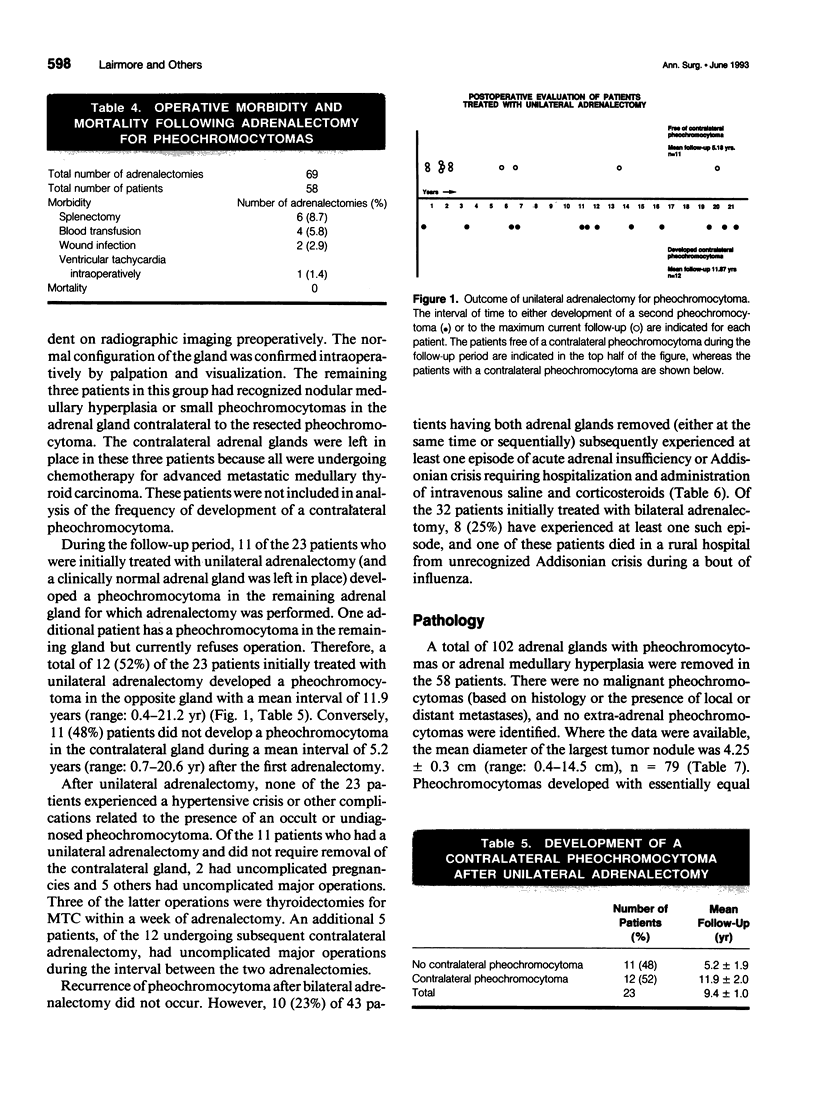
OBJECTIVE: The authors sought to determine the optimal surgical management of pheochromocytomas that develop in patients with multiple endocrine neoplasia (MEN) type 2 syndromes. SUMMARY BACKGROUND DATA: The performance of empirical bilateral adrenalectomy in patients with MEN 2A or MEN 2B, whether or not they have bilateral pheochromocytomas, is controversial. METHODS: The results of unilateral or bilateral adrenalectomy were studied in 58 patients (49 with MEN 2A and 9 with MEN 2B). Recurrence of disease was evaluated by measuring 24-hour urinary excretion rates of catecholamines and metabolites and by computed tomography (CT) scanning. RESULTS: The mean postoperative follow-up was 9.40 years. There was no operative mortality and malignant or extra-adrenal pheochromocytomas were not present. Twenty-three patients with a unilateral pheochromocytoma and a macroscopically normal contralateral gland underwent unilateral adrenalectomy. A pheochromocytoma developed in the remaining gland a mean of 11.87 years after the primary adrenalectomy in 12 (52%) patients. Conversely, 11 (48%) patients did not develop pheochromocytoma during a mean interval of 5.18 years. In the interval after unilateral adrenalectomy, no patient experienced hypertensive crises or other complications related to an undiagnosed pheochromocytoma. Ten (23%) of 43 patients having both adrenal glands removed (either at a single operation or sequentially) experienced at least one episode of acute adrenal insufficiency or Addisonian crisis, including one patient who died during a bout of influenza. CONCLUSIONS: Based on these data, the treatment of choice for patients with MEN 2A or MEN 2B and a unilateral pheochromocytoma is resection of only the involved gland. Substantial morbidity and significant mortality are associated with the Addisonian state after bilateral adrenalectomy.
Full text
PDF



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Carney J. A., Sizemore G. W., Sheps S. G. Adrenal medullary disease in multiple endocrine neoplasia, type 2: pheochromocytoma and its precursors. Am J Clin Pathol. 1976 Aug;66(2):279–290. doi: 10.1093/ajcp/66.2.279. [DOI] [PubMed] [Google Scholar]
- Carney J. A., Sizemore G. W., Tyce G. M. Bilateral adrenal medullary hyperplasia in multiple endocrine neoplasia, type 2: the precursor of bilateral pheochromocytoma. Mayo Clin Proc. 1975 Jan;50(1):3–10. [PubMed] [Google Scholar]
- Freier D. T., Thompson N. W., Sisson J. C., Nishiyama R. H., Freitas J. E. Dilemmas in the early diagnosis and treatment of multiple endocrine adenomatosis, type II. Surgery. 1977 Sep;82(3):407–413. [PubMed] [Google Scholar]
- Jansson S., Tisell L. E., Fjälling M., Lindberg S., Jacobsson L., Zachrisson B. F. Early diagnosis of and surgical strategy for adrenal medullary disease in MEN II gene carriers. Surgery. 1988 Jan;103(1):11–18. [PubMed] [Google Scholar]
- Lips K. J., Van der Sluys Veer J., Struyvenberg A., Alleman A., Leo J. R., Wittebol P., Minder W. H., Kooiker C. J., Geerdink R. A., Van Waes P. F. Bilateral occurrence of pheochromocytoma in patients with the multiple endocrine neoplasia syndrome type 2A (Sipple's syndrome). Am J Med. 1981 May;70(5):1051–1060. doi: 10.1016/0002-9343(81)90866-4. [DOI] [PubMed] [Google Scholar]
- Tibblin S., Dymling J. F., Ingemansson S., Telenius-Berg M. Unilateral versus bilateral adrenalectomy in multiple endocrine neoplasia IIA. World J Surg. 1983 Mar;7(2):201–208. doi: 10.1007/BF01656143. [DOI] [PubMed] [Google Scholar]
- Valk T. W., Frager M. S., Gross M. D., Sisson J. C., Wieland D. M., Swanson D. P., Mangner T. J., Beierwaltes W. H. Spectrum of pheochromocytoma in multiple endocrine neoplasia. A scintigraphic portrayal using 131I-metaiodobenzylguanidine. Ann Intern Med. 1981 Jun;94(6):762–767. doi: 10.7326/0003-4819-94-6-762. [DOI] [PubMed] [Google Scholar]
- van Heerden J. A., Sizemore G. W., Carney J. A., Grant C. S., ReMine W. H., Sheps S. G. Surgical management of the adrenal glands in the multiple endocrine neoplasia type II syndrome. World J Surg. 1984 Aug;8(4):612–621. doi: 10.1007/BF01654950. [DOI] [PubMed] [Google Scholar]