

Abstract
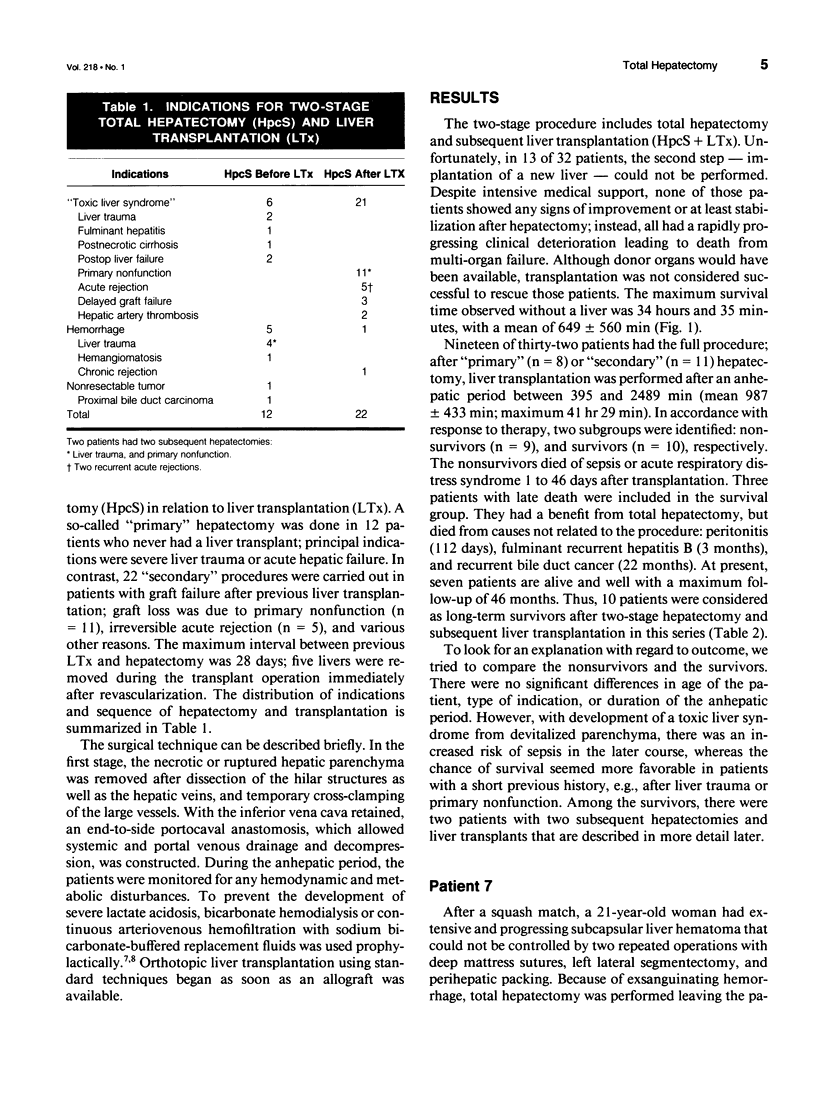
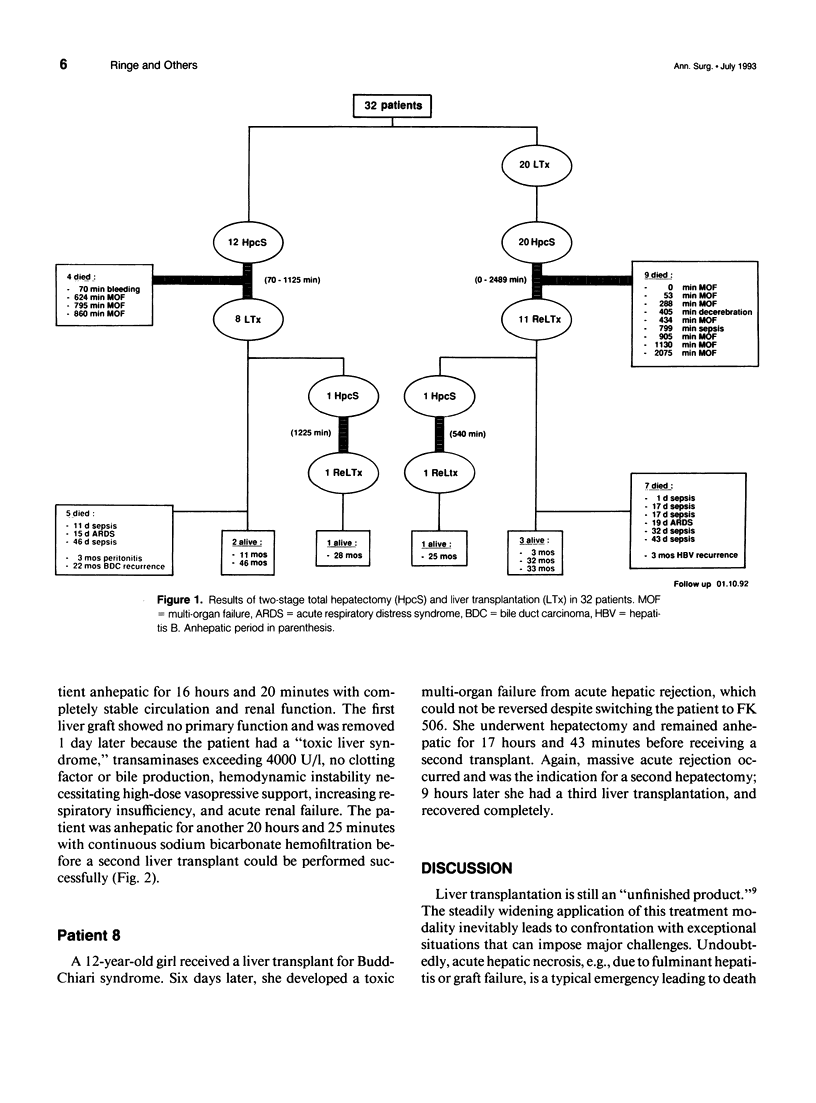
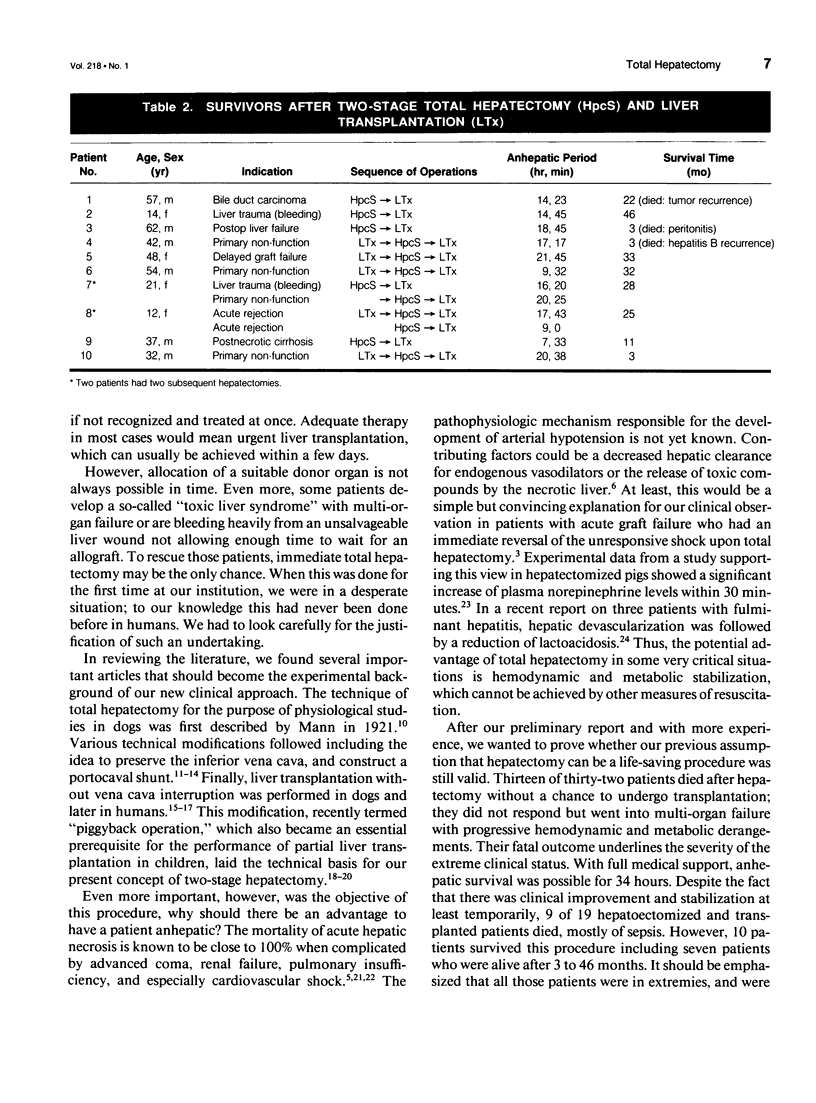
OBJECTIVE: This article describes the experience with a bridging procedure for a prolonged anhepatic period during clinical liver transplantation in case of special emergency situations. SUMMARY BACKGROUND DATA: Hepatic necrosis due to fulminant hepatitis or acute graft failure, as well as severe liver trauma are well-known and accepted indications for urgent liver transplantation. Prerequisite is the allocation of a suitable donor organ. If no allograft is available in time, patients with "toxic liver syndrome" or exsanguinating hemorrhage have been shown to benefit from advanced total hepatectomy. METHODS: As a modification of the standard one-stage procedure, recipient hepatectomy and subsequent liver transplantation are performed in two separate operations. To bridge the prolonged anhepatic period and to allow decompression and return of venous blood, an end-to-side portocaval shunt is constructed temporarily. RESULTS: Thirteen of thirty-two patients underwent hepatectomy but not transplantation subsequently, and died within 34 hours after progressive deterioration. In 19 of 32 patients, transplantation was realized 6-41 hours after hepatectomy; 9 of 19 patients died, mostly from sepsis. Ten of nineteen liver recipients survived the procedure including three unrelated late deaths; presently, seven patients are alive with a follow-up of 3 to 46 months. CONCLUSIONS: Two-stage total hepatectomy with temporary portocaval shunt, and subsequent liver transplantation can be a life-saving approach in patients most likely to die of the sequelae of advanced liver or graft necrosis or exsanguination that cannot be controlled by conventional treatment or immediate liver transplantation.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bihari D. J., Gimson A. E., Williams R. Cardiovascular, pulmonary and renal complications of fulminant hepatic failure. Semin Liver Dis. 1986 May;6(2):119–128. doi: 10.1055/s-2008-1040595. [DOI] [PubMed] [Google Scholar]
- Calne R. Y., Williams R. Liver transplantation in man. I. Observations on technique and organization in five cases. Br Med J. 1968 Nov 30;4(5630):535–540. doi: 10.1136/bmj.4.5630.535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davenport A., Will E. J., Davison A. M. Paradoxical increase in arterial hydrogen ion concentration in patients with hepatorenal failure given lactate-based fluids. Nephrol Dial Transplant. 1990;5(5):342–346. doi: 10.1093/ndt/5.5.342. [DOI] [PubMed] [Google Scholar]
- FRANK H. A., JACOB S. W. One-stage hepatectomy in the dog; preserving the inferior vena cava. Am J Physiol. 1952 Jan;168(1):156–158. doi: 10.1152/ajplegacy.1951.168.1.156. [DOI] [PubMed] [Google Scholar]
- Husberg B. S., Goldstein R. M., Klintmalm G. B., Gonwa T., Ramsay M., Cofer J., Solomon H., Watemberg I. A totally failing liver may be more harmful than no liver at all: three cases of total hepatic devascularization in preparation for emergency liver transplantation. Transplant Proc. 1991 Feb;23(1 Pt 2):1533–1535. [PubMed] [Google Scholar]
- Lempinen M., Soyer T., Eiseman B. A new technique for preparing totally hepatectomized pigs. Surgery. 1973 Mar;73(3):463–467. [PubMed] [Google Scholar]
- Olbricht C. J., Huxmann-Nägeli D., Bischoff H. Bikarbonat- statt laktatgepufferter Substitutionslösung zur kontinuierlichen Hämofiltration im Intensivbereich. Anasth Intensivther Notfallmed. 1990 Apr;25(2):164–167. [PubMed] [Google Scholar]
- Pichlmayr R., Ringe B., Lauchart W., Wonigeit K. Liver transplantation. Transplant Proc. 1987 Feb;19(1 Pt 1):103–112. [PubMed] [Google Scholar]
- Rigler B., Zalaudek G., Hermann W., Stenzl W., Tscheliessnigg K. H., Tilz G., Höfer G., Rehak P. Klinische Erfahrung mit einer atypischen Hohlvenenanastomose bei einem Fall von orthotoper Lebertransplantation. Langenbecks Arch Chir. 1981;354(1):31–38. doi: 10.1007/BF01834014. [DOI] [PubMed] [Google Scholar]
- Ringe B., Pichlmayr R., Burdelski M. A new technique of hepatic vein reconstruction in partial liver transplantation. Transpl Int. 1988 Apr;1(1):30–35. doi: 10.1007/BF00337846. [DOI] [PubMed] [Google Scholar]
- Ringe B., Pichlmayr R., Lübbe N., Bornscheuer A., Kuse E. Total hepatectomy as temporary approach to acute hepatic or primary graft failure. Transplant Proc. 1988 Feb;20(1 Suppl 1):552–557. [PubMed] [Google Scholar]
- Ringe B., Pichlmayr R., Ziegler H., Grosse H., Kuse E., Oldhafer K., Bornscheuer A., Gubernatis G. Management of severe hepatic trauma by two-stage total hepatectomy and subsequent liver transplantation. Surgery. 1991 Jun;109(6):792–795. [PubMed] [Google Scholar]
- Ritt D. J., Whelan G., Werner D. J., Eigenbrodt E. H., Schenker S., Combes B. Acute hepatic necrosis with stupor or coma. An analysis of thirty-one patients. Medicine (Baltimore) 1969 Mar;48(2):151–172. doi: 10.1097/00005792-196903000-00003. [DOI] [PubMed] [Google Scholar]
- STARZL T. E., BERNHARD V. M., BENVENUTO R., CORTES N. A new method for one-stage hepatectomy for dogs. Surgery. 1959 Nov;46:880–886. [PMC free article] [PubMed] [Google Scholar]
- Starzl T. E., Todo S., Tzakis A. G., Gordon R. D., Makowka L., Stieber A., Podesta L., Yanaga K., Concepcion W., Iwatsuki S. Liver transplantation: an unfinished product. Transplant Proc. 1989 Feb;21(1 Pt 2):2197–2200. [PMC free article] [PubMed] [Google Scholar]
- Strong R., Ong T. H., Pillay P., Wall D., Balderson G., Lynch S. A new method of segmental orthotopic liver transplantation in children. Surgery. 1988 Jul;104(1):104–107. [PubMed] [Google Scholar]
- Trewby P. N., Williams R. Pathophysiology of hypotension in patients with fulminant hepatic failure. Gut. 1977 Dec;18(12):1021–1026. doi: 10.1136/gut.18.12.1021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tzakis A., Todo S., Starzl T. E. Orthotopic liver transplantation with preservation of the inferior vena cava. Ann Surg. 1989 Nov;210(5):649–652. doi: 10.1097/00000658-198911000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]