

Abstract
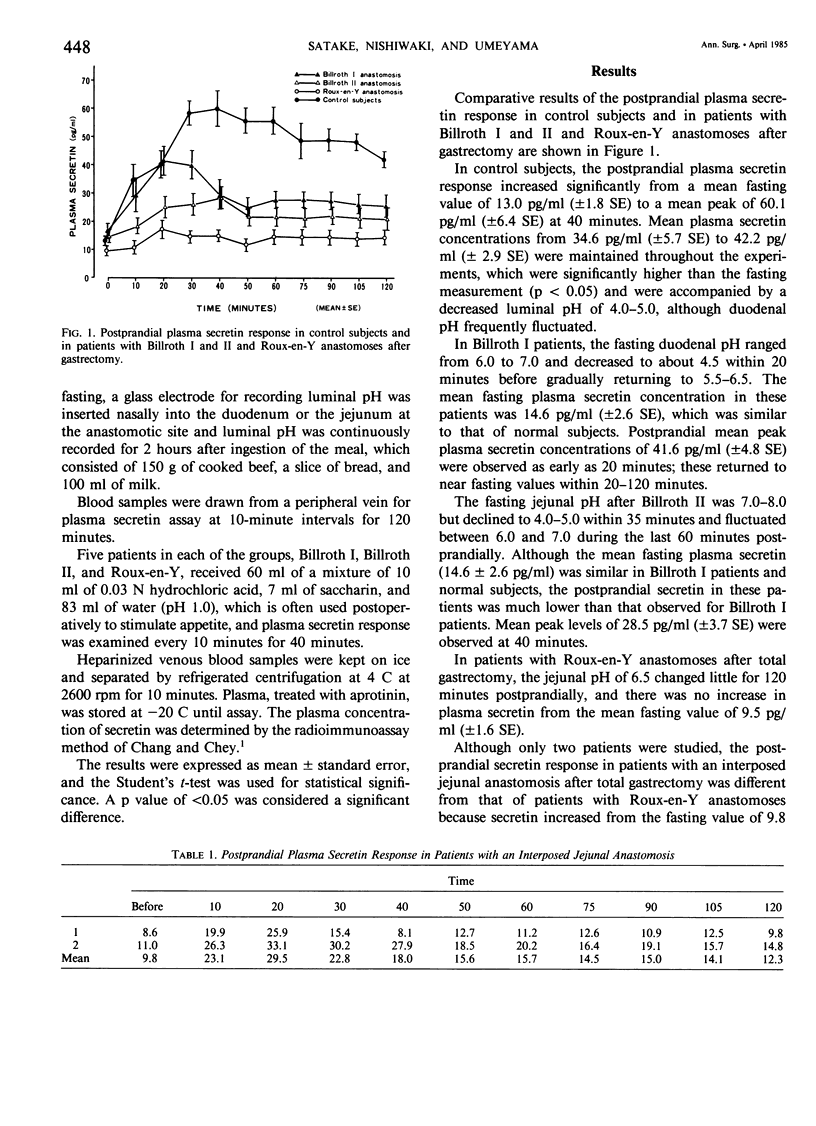
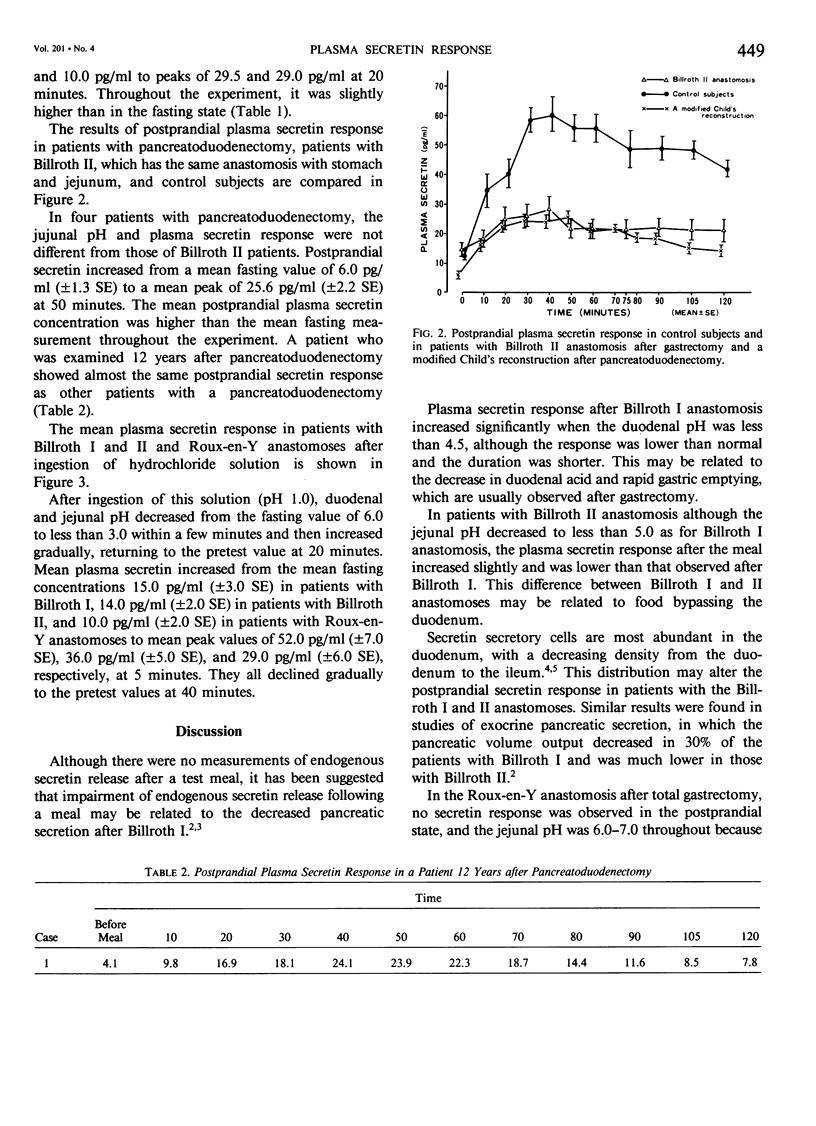
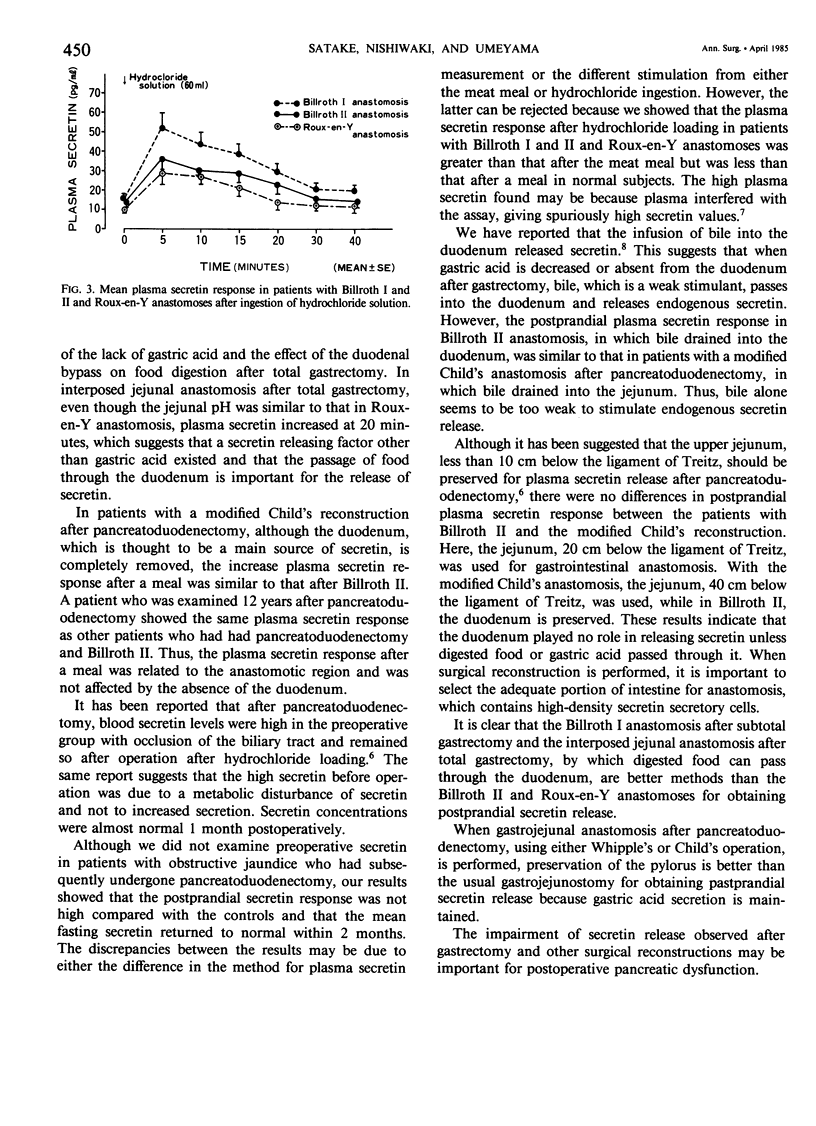
The postprandial plasma secretin response was examined in ten normal persons, seven patients with a Billroth I and seven with a Billroth II anastomosis after subtotal gastrectomy, seven with a Roux-en-Y anastomosis, two with an interposed jejunal anastomosis, and five with a modified Child's anastomosis after pancreatoduodenectomy. The postprandial plasma secretin response in patients with Billroth I anastomosis was better than that in patients with a Billroth II anastomosis but was less than that of normal subjects. Although no postprandial secretin response was noted in Roux-en-Y anastomosis after total gastrectomy, a response was seen in patients with the interposed jejunal anastomosis because the digested food passed through the duodenum, but it was less than that for Billroth I and II patients and normal controls. After a modified Child's reconstruction, the postprandial secretin response was similar to that of patients with the Billroth II, which preserved the duodenum. A patient with a modified Child's reconstruction was examined 12 years after surgery and had the same response as other patients with the modified Child's reconstruction and those with a Billroth II anastomosis within 2 months after surgery. After ingestion of hydrochloride solution, the plasma secretin release in patients with a Billroth I and II anastomosis after subtotal gastrectomy and Roux-en-Y anastomosis after total gastrectomy had a better response than after a meal, but this was less than in normal subjects. The authors suggest that careful selection of intestine for the gastrointestinal anastomosis, which contains many secretin secretory cells, is important to obtain endogenous secretin release. For gastrojejunostomy after pancreatoduodenectomy, a method preserving the pylorus is better than the usual gastrojejunostomy because it maintains gastric acid. The ingestion of secretin stimulants, such as hydrochloride, may help to prevent pancreatic dysfunction after gastrectomy and other surgical reconstructions.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BUTLER T. J. The effect of gastrectomy on pancreatic secretion in man. Ann R Coll Surg Engl. 1961 Nov;29:300–327. [PMC free article] [PubMed] [Google Scholar]
- Burhol P. G. On plasma/serum interferences on radioimmunoassay of regulatory peptides. Scand J Gastroenterol. 1984 Mar;19(2):129–130. [PubMed] [Google Scholar]
- Chang T. M., Chey W. Y. Radioimmunoassay of secretin. A critical review and current status. Dig Dis Sci. 1980 Jul;25(7):529–552. doi: 10.1007/BF01315215. [DOI] [PubMed] [Google Scholar]
- Chey W. Y., Escoffery R. Secretion cells in the gastrointestinal tract. Endocrinology. 1976 Jun;98(6):1390–1395. doi: 10.1210/endo-98-6-1390. [DOI] [PubMed] [Google Scholar]
- Faichney A., Chey W. Y., Kim Y. C., Lee K. Y., Kim M. S., Chang T. M. Effect of sodium oleate on plasma secretin concentration and pancreatic secretion in dog. Gastroenterology. 1981 Sep;81(3):458–462. [PubMed] [Google Scholar]
- MACLEAN L. D., PERRY J. F., KELLY W. D., MOSSER D. G., MANNICK A., WANGENSTEEN O. H. Nutrition following subtotal gastrectomy of four types (Billroth I and II, segmental, and tubular resections). Surgery. 1954 May;35(5):705–718. [PubMed] [Google Scholar]
- Nishiwaki H., Satake K., Umeyama K., Chey W. Y. [The effect of bile on endogenous secretin release]. Nihon Shokakibyo Gakkai Zasshi. 1982 Aug;79(8):1619–1625. [PubMed] [Google Scholar]
- Polak J. M., Bloom S., Coulling I., Pearse A. G. Immunofluorescent localization of secretin in the canine duodenum. Gut. 1971 Aug;12(8):605–610. doi: 10.1136/gut.12.8.605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sudo T., Ishiyama K., Kawamura M., Tsubakimoto R., Shobu R., Takemoto M., Shono K., Umemura H., Shiraha S., Kuyama T. Changes in plasma gastrin and secretin levels after pancreaticoduodenectomy. Surg Gynecol Obstet. 1984 Feb;158(2):133–136. [PubMed] [Google Scholar]