

Abstract
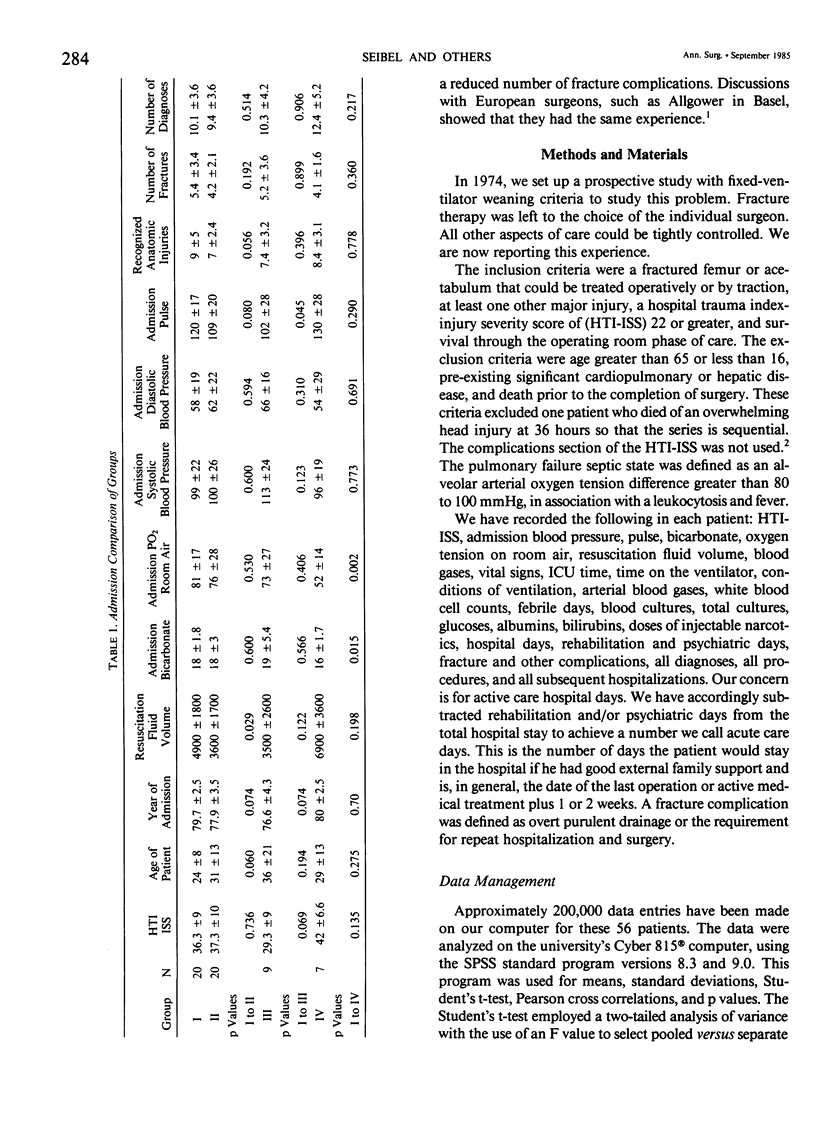
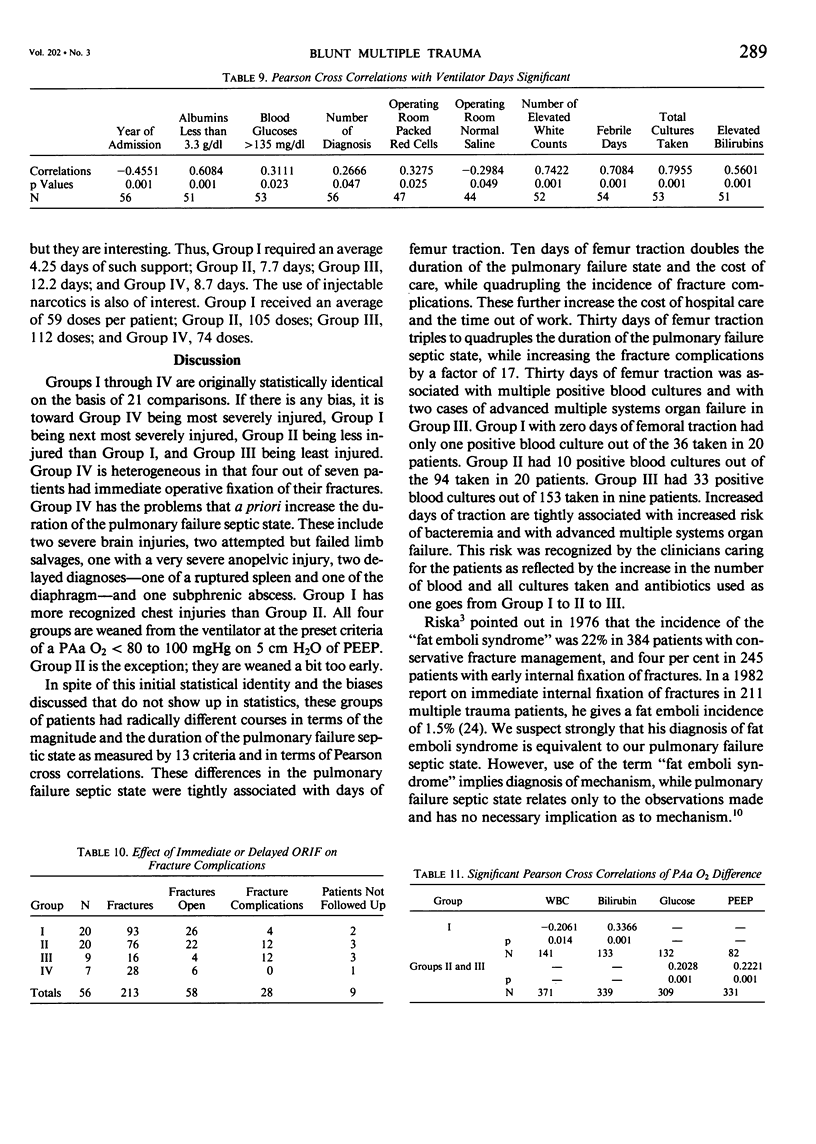
Fifty-six blunt multiple trauma patients (HTI-ISS 22-57) were studied for the effects of immediate versus delayed internal fixation of a femur or acetabular fracture on the pulmonary failure septic state. The pulmonary failure septic state may be defined as an alveolar arterial oxygen tension difference greater than 100, plus fever and leukocytosis. These patients were divided into four groups. Group I (N = 20) had immediate internal fixation, postoperative ventilatory support, and was sitting up at 30 hours. Group II (N = 20) had 10 days of femur traction and postoperative ventilatory support. Group III (N = 9) was immediately extubated after surgery and had 30 days of femur traction. Group IV (N = 7) had special circumstances that should increase the duration of the pulmonary failure septic state. These four groups of patients were statistically identical by 20 different criteria on admission except that Group I had more recognized chest injuries than Group II (12 vs. 9). Group I required 3.4 +/- 2.6 days of ventilator support and 7.5 +/- 3.8 intensive care unit (ICU) days; they had 12 +/- 8.8 elevated white counts, 3.8 +/- 4 febrile days, 0.05 positive blood cultures per patient, four fracture complications out of 93 fractures, 59 injections of narcotics, and 23 +/- 8.6 acute care days. Ten days of femur traction doubled the duration of the pulmonary failure septic state relative to Group I at a statistically significant level for nine out of 10 criteria, while increasing the number of positive blood cultures by a factor of 10, the number of fracture complications by a factor of 3.5, and the use of injectable narcotics by a factor of 2. Thirty days of femur traction increased the duration of the pulmonary failure septic state relative to Group I by a factor of 3 to 5 for all criteria at a statistically significant level, while increasing fracture complications by a factor of 17, positive blood cultures by a factor of 74, and the use of narcotics by a factor of 2. Group IV, which had four out of seven immediate internal fixations, behaved similarly to Group II. Femoral shaft traction should be avoided in the blunt multiple trauma patients because it greatly increases the cost of care and the risk of multiple systems organ failure.(ABSTRACT TRUNCATED AT 400 WORDS)
Full text
PDF







Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Baker S. P., O'Neill B., Haddon W., Jr, Long W. B. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974 Mar;14(3):187–196. [PubMed] [Google Scholar]
- Border J. R., Hopkinson B. R., Schenk W. G., Jr Mechanisms of pulmonary trauma. An experimental study. J Trauma. 1968 Jan;8(1):47–62. doi: 10.1097/00005373-196801000-00006. [DOI] [PubMed] [Google Scholar]
- Clowes G. H., Jr, George B. C., Villee C. A., Jr, Saravis C. A. Muscle proteolysis induced by a circulating peptide in patients with sepsis or trauma. N Engl J Med. 1983 Mar 10;308(10):545–552. doi: 10.1056/NEJM198303103081001. [DOI] [PubMed] [Google Scholar]
- Gelfand J. A. How do complement components and fragments affect cellular immunological function? J Trauma. 1984 Sep;24(9 Suppl):S118–S124. [PubMed] [Google Scholar]
- Goris R. J., Gimbrère J. S., van Niekerk J. L., Schoots F. J., Booy L. H. Early osteosynthesis and prophylactic mechanical ventilation in the multitrauma patient. J Trauma. 1982 Nov;22(11):895–903. doi: 10.1097/00005373-198211000-00002. [DOI] [PubMed] [Google Scholar]
- Hechtman H. B., Lonergan E. A., Shepro D. Platelet and leukocyte lung interactions in patients with respiratory failure. Surgery. 1978 Feb;83(2):155–163. [PubMed] [Google Scholar]
- Heideman M., Hugli T. E. Anaphylatoxin generation in multisystem organ failure. J Trauma. 1984 Dec;24(12):1038–1043. doi: 10.1097/00005373-198412000-00006. [DOI] [PubMed] [Google Scholar]
- LaDuca J. N., Bone L. L., Seibel R. W., Border J. R. Primary open reduction and internal fixation of open fractures. J Trauma. 1980 Jul;20(7):580–586. doi: 10.1097/00005373-198007000-00006. [DOI] [PubMed] [Google Scholar]
- Lewis F. R., Jr, Blaisdell F. W., Schlobohm R. M. Incidence and outcome of posttraumatic respiratory failure. Arch Surg. 1977 Apr;112(4):436–443. doi: 10.1001/archsurg.1977.01370040088014. [DOI] [PubMed] [Google Scholar]
- Malangoni M. A., Dillon L. D., Klamer T. W., Condon R. E. Factors influencing the risk of early and late serious infection in adults after splenectomy for trauma. Surgery. 1984 Oct;96(4):775–783. [PubMed] [Google Scholar]
- PELTIER L. F. An appraisal of the problem of fat embolism. Surg Gynecol Obstet. 1957 Apr;104(4):313–324. [PubMed] [Google Scholar]
- Powanda M. C., Beisel W. R. Hypothesis: leukocyte endogenous mediator/endogenous pyrogen/lymphocyte-activating factor modulates the development of nonspecific and specific immunity and affects nutritional status. Am J Clin Nutr. 1982 Apr;35(4):762–768. doi: 10.1093/ajcn/35.4.762. [DOI] [PubMed] [Google Scholar]
- Riska E. B., von Bonsdorff H., Hakkinen S., Jaroma H., Kiviluoto O., Paavilainen T. Primary operative fixation of long bone fractures in patients with multiple injuries. J Trauma. 1977 Feb;17(2):111–121. doi: 10.1097/00005373-197702000-00005. [DOI] [PubMed] [Google Scholar]
- Semmlow J. L., Cone R. Utility of the injury severity score: a confirmation. Health Serv Res. 1976 Spring;11(1):45–52. [PMC free article] [PubMed] [Google Scholar]
- Till G. O., Beauchamp C., Menapace D., Tourtellotte W., Jr, Kunkel R., Johnson K. J., Ward P. A. Oxygen radical dependent lung damage following thermal injury of rat skin. J Trauma. 1983 Apr;23(4):269–277. doi: 10.1097/00005373-198304000-00001. [DOI] [PubMed] [Google Scholar]
- Wolff G., Dittmann M., Rüedi T., Buchmann B., Allgöwer M. Koordination von Chirurgie und Intensivmedizin zur Vermeidung der posttraumatischen respiratorischen Insuffizienz. Unfallheilkunde. 1978 Jun;81(6):425–442. [PubMed] [Google Scholar]