

Abstract
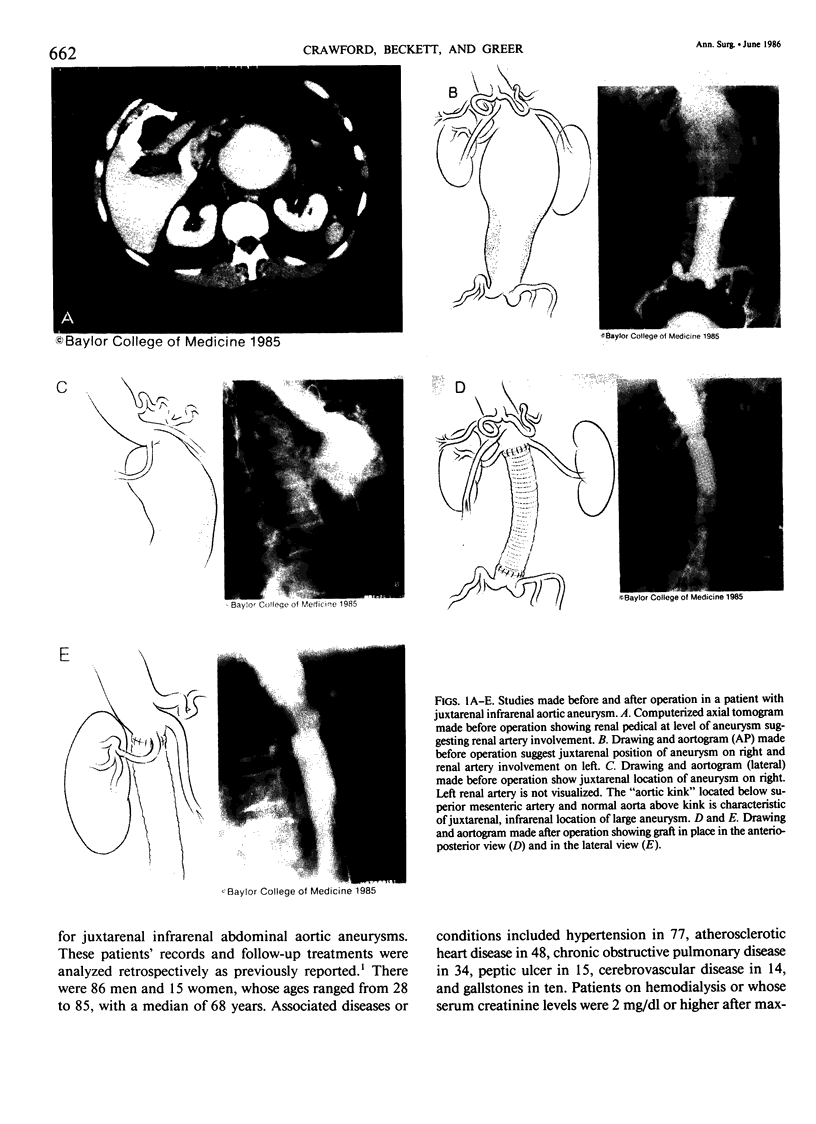
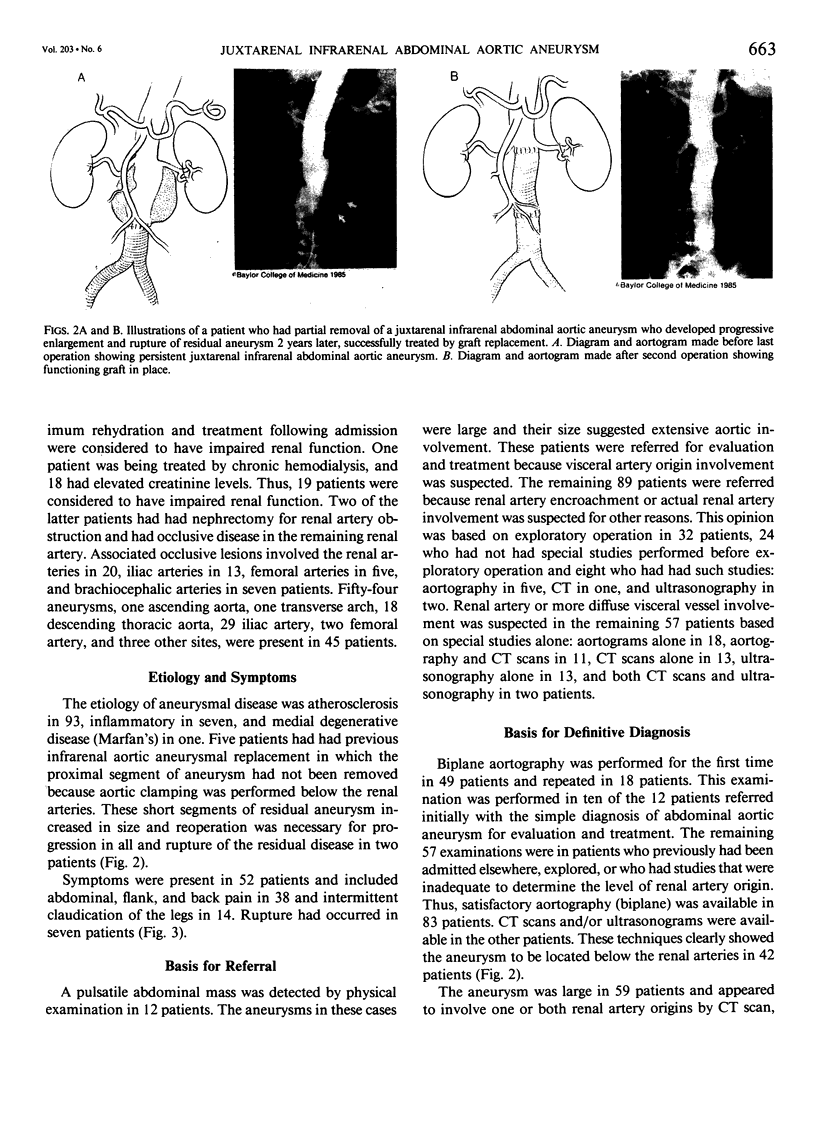
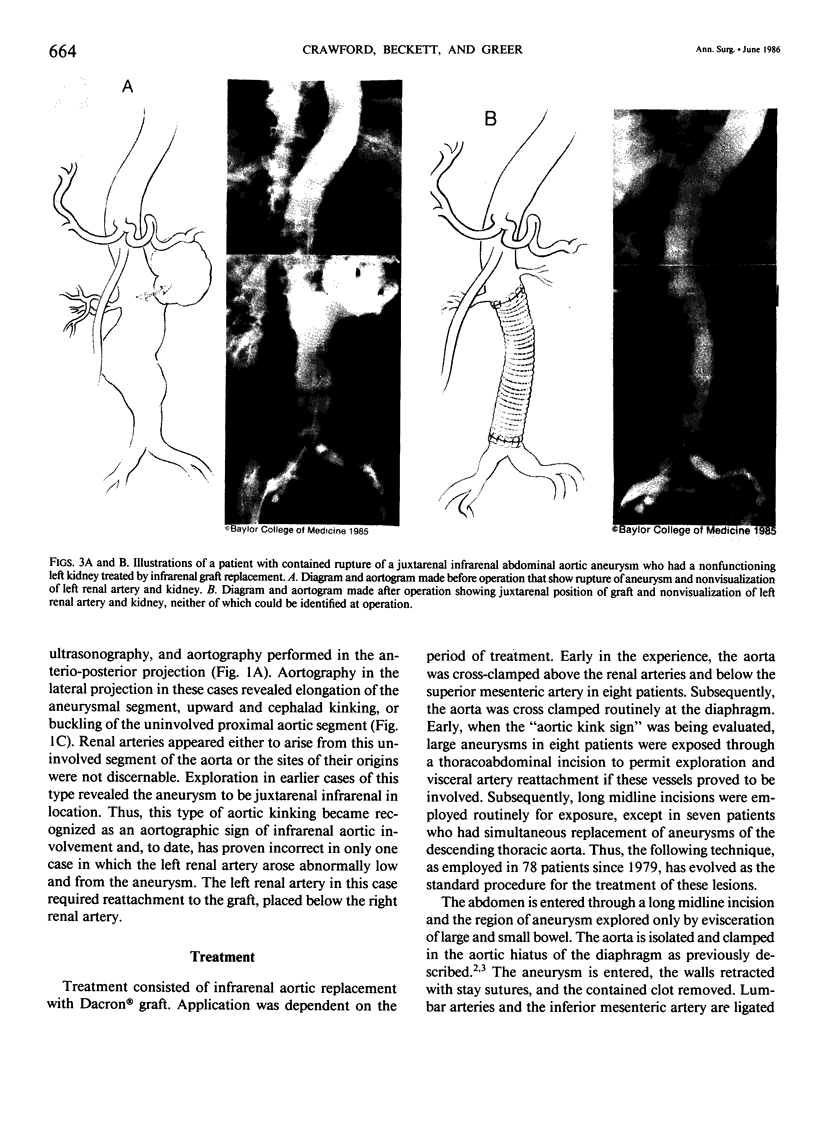
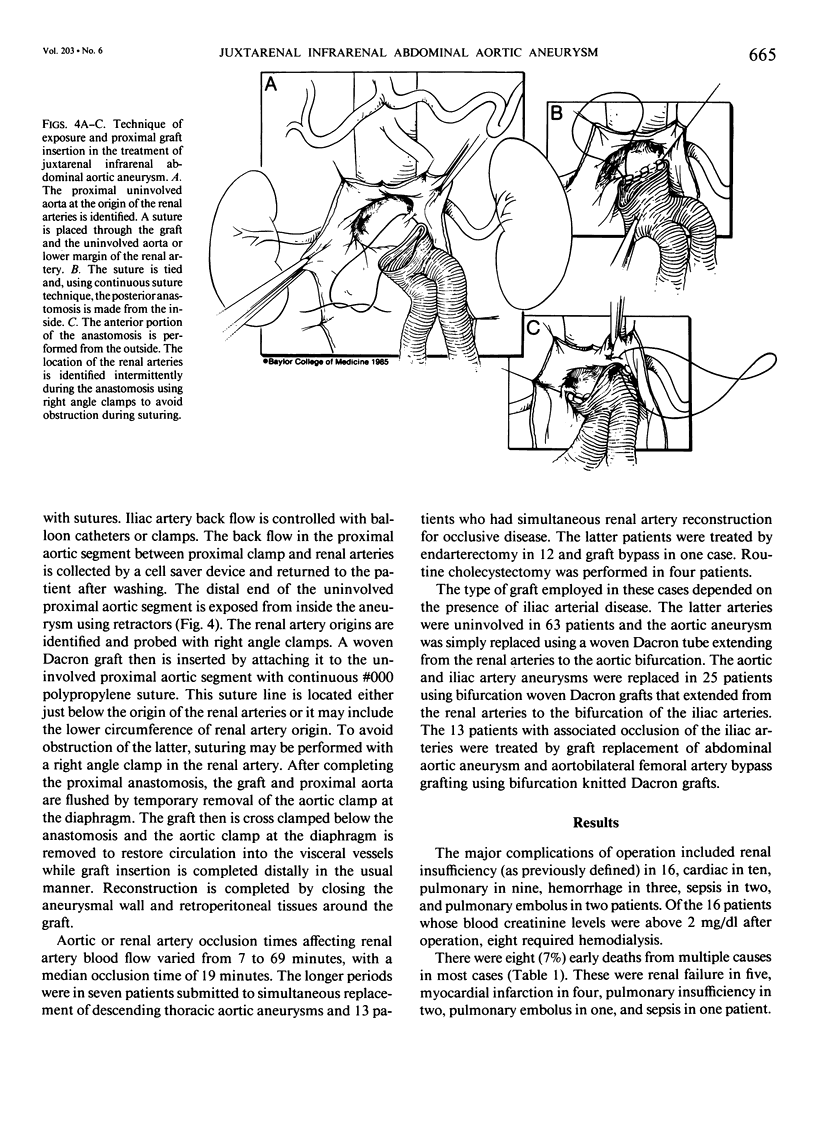
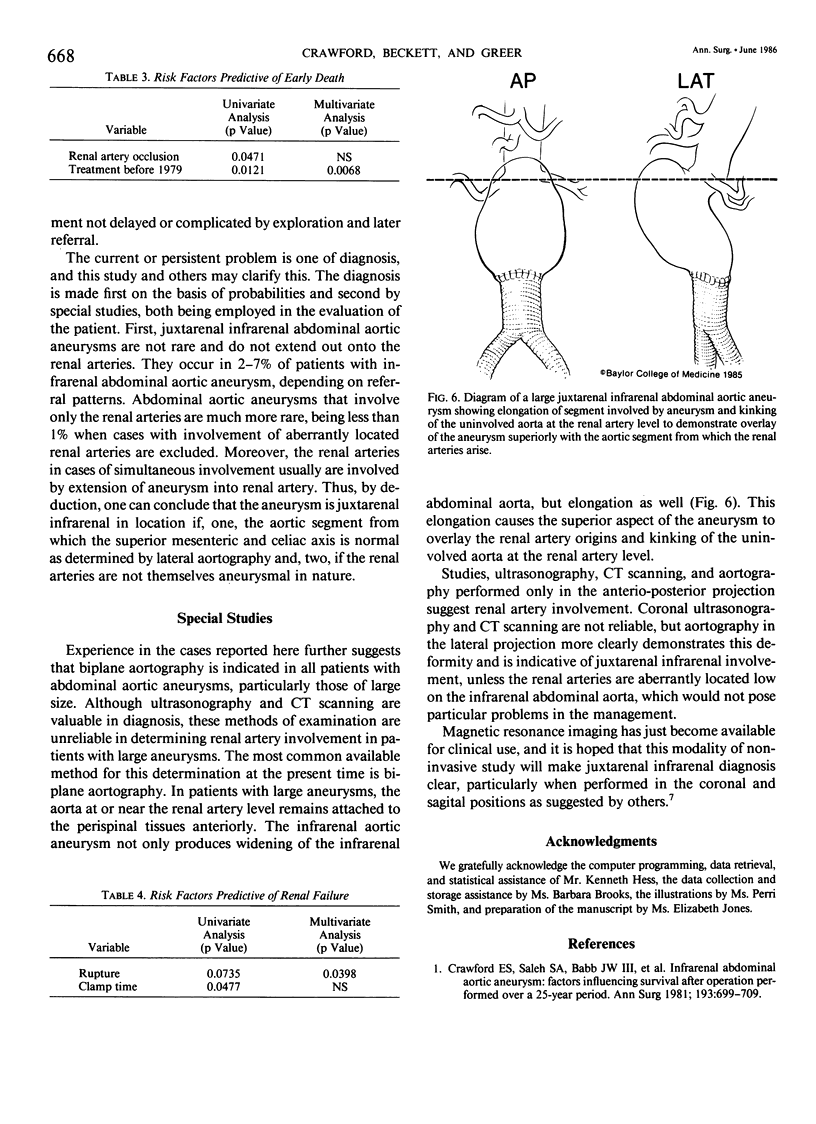
Juxtarenal infrarenal abdominal aortic aneurysms are defined as those aneurysms that involve the infrarenal abdominal aorta adjacent to or including the lower margin of renal artery origins. The misinterpretation of findings at exploratory operation or special studies may suggest renal artery involvement and result in abandonment of operation and/or referral to distant centers, thus delaying treatment. This report is concerned with 101 patients with a median age of 68 who had such aneurysms, all referred with a diagnosis of renal or visceral arterial involvement either after exploratory operation (32), because of aneurysmal size (12), or due to misinterpretation of special studies (57). Computed tomographic (CT) scans, ultrasounds, and aortograms in the anterio-posterior projection frequently suggested renal artery involvement due to the fact that the upper end of aneurysm frequently lay over the renal artery origins due to infrarenal aortic elongation and buckling of the aorta at the renal artery level. The true nature of the lesion was best demonstrated by aortography performed in the lateral position. The operation producing the best results was one performed through a midline abdominal incision. The aorta is cross-clamped at the diaphragm and the proximal anastomosis is performed from inside the aneurysm at the renal artery level. The graft then is clamped and the other clamp removed to restore flow in the visceral vessels while the distal anastomosis is completed. Early survival occurred in 93% of patients employing the operation, despite the fact that other conditions frequently were present: renal insufficiency in 19, rupture in seven, renal artery occlusive disease in 20, chronic obstructive pulmonary disease in 34, and hypertension in 77.
Full text
PDF

Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Amparo E. G., Hoddick W. K., Hricak H., Sollitto R., Justich E., Filly R. A., Higgins C. B. Comparison of magnetic resonance imaging and ultrasonography in the evaluation of abdominal aortic aneurysms. Radiology. 1985 Feb;154(2):451–456. doi: 10.1148/radiology.154.2.3880912. [DOI] [PubMed] [Google Scholar]
- Crawford E. S., Saleh S. A., Babb J. W., 3rd, Glaeser D. H., Vaccaro P. S., Silvers A. Infrarenal abdominal aortic aneurysm: factors influencing survival after operation performed over a 25-year period. Ann Surg. 1981 Jun;193(6):699–709. doi: 10.1097/00000658-198106000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perry M. O., Silane M. F. Management of renovascular problems during aortic operations. Arch Surg. 1984 Jun;119(6):681–685. doi: 10.1001/archsurg.1984.01390180047008. [DOI] [PubMed] [Google Scholar]
- Robbs J. V., Human R. R., Rajaruthnam P. Management of abdominal aortic aneurysms extending above the renal arteries. S Afr J Surg. 1983 Dec;21(4):234–242. [PubMed] [Google Scholar]
- Stoney R. J., Skiöldebrand C. G., Qvarfordt P. G., Reilly L. M., Ehrenfeld W. K. Juxtarenal aortic atherosclerosis. Surgical experience and functional result. Ann Surg. 1984 Sep;200(3):345–354. doi: 10.1097/00000658-198409000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]