

Abstract
Background
Medical conditions may adversely affect driving ability. Many North American jurisdictions provide restricted driving licences that permit people with certain medical conditions to drive under limited conditions, but the effectiveness of such programs has not yet been determined. The objectives of this study were to evaluate the rates of crashes and traffic violations among drivers with a restricted licence, compared with the rates in the general driving population, and to compare the crash and traffic violation rates before and after driving restrictions were imposed.
Methods
We retrospectively analyzed a cohort of all licensed Saskatchewan drivers registered from Jan. 1, 1992, to Apr. 19, 1999. The cohort was divided into those with a restricted licence and those with an unrestricted general licence. We used multivariate Poisson regression to calculate incidence rate ratios (IRRs) for at-fault crashes and traffic violations, adjusting for age, sex and residence (urban v. rural). We used interventional time series analysis to compare rates of crashes and traffic violations before and after the imposition of driving restrictions.
Results
Of the 703 758 drivers in the study, 23 185 (3.3%) had a restricted licence. Restricted licence holders had a higher crash rate than drivers without restrictions (adjusted IRR 1.13, 95% confidence interval [CI] 1.11–1.17). However, this rate was lower than that among male drivers (adjusted IRR 2.01, 95% CI 1.99–2.02) and urban drivers (adjusted IRR 1.38, 95% CI 1.37–1.39). Drivers with restricted licences had a lower traffic violation rate than those without restrictions (adjusted IRR 0.93, 95% CI 0.91–0.95). At-fault crash rates decreased by 12.8% (95% CI 2.4%–23.2%) and adjusted traffic violation rates decreased by 10.0% (95% CI 4.4%–15.7%) after restrictions were imposed. During the study period, licence restrictions likely averted up to 816 crashes and 751 traffic violations.
Interpretation
Province-wide population data suggest that a restricted licensing program appears to provide a significant decrease in the rates of crashes and traffic violations.
Driving motor vehicles has become almost a basic activity of daily living.1 Driving ability is often essential for independence, especially for those in smaller towns and rural areas. Visual,2,3,4 cardiac,5,6 arthritic,7,8 cognitive,9,10,11,12,13 and neurologic14,15,16,17 impairments are each associated with increased risks of motor vehicle accidents. In many jurisdictions, people with these diseases are prohibited from driving to protect both the public and the patient. Unfortunately for such patients, this often results in a large loss of independence.
Some jurisdictions provide restricted or conditional licences for people with medical impairments.18 These restricted licences allow driving under specific or limited conditions, such as only during daylight hours or within a certain radius of the person's home. However, the effectiveness of such programs is unknown.18,19 Crancer and McMurray19 studied the accident and violation rates of drivers with licence restrictions because of medical impairments in the state of Washington from 1961 to 1967. They found that drivers with diabetes mellitus, epilepsy or fainting had a significantly higher number of crashes than the control subjects. Drivers with diabetes, epilepsy and other conditions also had higher violation rates than control subjects. In a subsequent study Crancer and O'Neall6 determined that drivers in Washington with licence restrictions for heart disease had an accident rate similar to that of a control population. These studies are limited by not controlling for changes in driver licence status or driver residence. Also, the studies may be outdated since population demographic characteristics, motor vehicles and road conditions have changed considerably since the 1960s.20
More recently, the National Highway Traffic Safety Association, US Department of Transportation, evaluated drivers with medical conditions who were licensed in Utah between 1992 and 1996.21 Two groups of drivers were studied: those with licence restrictions and a comparison group with a similar demographic profile with regard to age, sex and county of residence who did not have licence restrictions. When all disease groups were combined, drivers with restricted licences had higher crash rates than unrestricted drivers (relative risk 1.74, 95% confidence interval [CI] 1.49–2.04). For some medical conditions, such as diabetes, epilepsy, and cardiovascular, psychiatric and visual problems, drivers with no restrictions had lower crash rates than those with restrictions. Although these results suggest that restricted licensing is ineffective, the study was limited because crash rates and rate differences could not be calculated. These data are essential for physicians and policy-makers to determine whether the results are clinically significant.
Since most jurisdictions in North America endorse restricted licensing to one degree or another,22 studies suggesting that drivers with licence restrictions may have higher at-fault crash rates than control subjects are of concern. Accurately determining the effectiveness of restricted licensing is important for physicians who must identify medically unfit drivers,23 government policy-makers and society at large. If restricted licensing is ineffective, many North American jurisdictions should reconsider their policies of providing restricted licences. However, if restricted licensing decreases crash and traffic violation rates to acceptable levels, jurisdictions whose only current option is an unrestricted licence might introduce restricted licensing.
Saskatchewan Government Insurance (SGI) provides insurance coverage to all drivers in the province. SGI delivers a program that issues restricted licences to people with medical impairments that may affect driving ability. Restrictions include both driving restrictions (e.g., driving during daylight hours only or driving within a certain number of kilometres from home only) and licensing restrictions (e.g., physical examination or periodic eye examinations are required for licensing). Restrictions are based on a combination of a driving ability assessment, an on-road evaluation and the expected progression of the person's medical condition. Driving and licensing restrictions may be imposed simultaneously. The SGI database contains the driving history of all drivers in the province as well as demographic information, including date of birth, sex, and urban or rural residence (as defined by postal code).
Our objectives were to compare drivers with and without licence restrictions with regard to crash rates and traffic violation rates while controlling for sex, age and residence, and to determine whether crash and violation rates change after licence restrictions are imposed.
Methods
We included all drivers who held a valid driver's licence between Jan. 1, 1992, and Apr. 19, 1999. Driving record data before Jan. 1, 1992, were incomplete. We excluded drivers with a licence higher than class 5 (general) because these drivers would be more likely to be commercial drivers and to have higher levels of experience and driver training.24 We excluded drivers born before Jan. 1, 1900, because their birth date was unreliable, and those with a restriction solely for alcohol or substance abuse since these conditions are known to be associated with higher crash and traffic violation rates.25,26 We identified the date that all driving or licensing restrictions were imposed. The dates of all crashes that resulted in an insurance claim and all traffic violations were recorded, as were crash fault status and violation type. In the event of a crash, a driver was classified as being “at fault” if he or she was considered, by the insurance adjuster, to be at least 50% responsible for the crash. Throughout this paper, involvement in a crash is used interchangeably with at-fault crash. All moving violations resulting in noncriminal or criminal convictions were classified as violations in this study. Criminal and noncriminal traffic violations were combined. The dates of licence suspension or cancellation, which we considered in calculating crash and traffic violation rates, were also recorded. Since Saskatchewan drivers must renew their licence annually, we considered unrenewed licences as inactive and did not include them in calculating person-years of driving time.
We classified drivers as having a restricted or unrestricted licence. For the base analysis, drivers with a driving restriction and those with a licensing restriction were grouped together. For drivers with restrictions, their driving records before the restriction was imposed were included in the cohort of drivers without restrictions, after a sensitivity analysis demonstrated no difference in the rates for the unrestricted cohort when these records were censored.
We used Poisson regression analysis to determine crash and traffic violation rates among drivers with and without licence restrictions after adjusting for age, sex and residence (urban v. rural). We examined the effect of a licence restriction on driving performance by calculating crude incidence rates of crashes and traffic violation rates among drivers with restrictions before and after the restrictions were imposed. We then used interventional autoregressive, integrated, moving average (ARIMA) time series modelling to determine whether the rates before and after the restrictions were imposed differed significantly.27 We used time series analysis because data with a temporal sequence are often autocorrelated (i.e., the value at time x is affected by the value at time x – 1). Therefore, the error terms of these observations are not independent, which makes simple regression and standard inferential testing inappropriate. Time series analysis models autocorrelation in temporally sequenced data, thereby permitting traditional regression and inferential testing. In each model, licence restriction was represented by a dummy series (0 representing before restriction, and 1 representing after restriction) that was cross-correlated with the crash or violation series. We reviewed the autocorrelation plots and the partial autocorrelation plots to determine the presence of moving average and autoregressive processes respectively. If the t ratio for the intervention parameter in the best-fitting model28 had a 2-sided p value less than 0.05, restricted licensing was considered to be associated with a significant change in the crash or traffic violation rates.
The study was approved by the Research Ethics Committee of The Rehabilitation Centre, Ottawa.
Results
There were 1 176 486 drivers registered in the SGI database at some time during the study period. A total of 472 728 drivers were excluded: 82 183 because they were born before 1900, 120 808 because they had an elevated licence class, and 269 737 because they did not hold a driver's licence during the study period. Of the remaining 703 758 drivers, 23 185 had a licence restriction at some point: 20 074 had a licensing restriction only, 2010 had both a driving and a licensing restriction, and 1101 had a driving restriction only. Restricted licence holders accounted for 72 410 of the 3 792 479 person-years of driving.
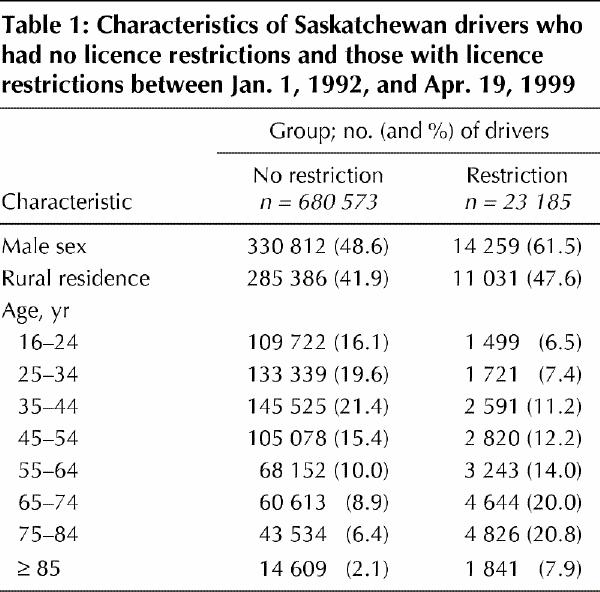
Compared with unrestricted licence holders, drivers with restricted licences were older and were more likely to be male and to live in a rural location (Table 1). Overall, 537 749 drivers (76%) had had no crashes, 115 808 (16%) had had 1 crash, 34 702 (5%) had had 2 crashes, and 15 499 (2%) had had 3 or more crashes. Restricted licence holders were significantly less likely than drivers with unrestricted licences to have been involved in crashes (19 236/23 185 [83%] v. 537 749/703 758 [76%]; p < 0.001). Overall, 438 331 drivers (62%) had had no traffic violations, 134 463 (19%) had had 1 violation, 56 582 (8%) had had 2 violations, and 74 382 (11%) had had 3 or more violations. Drivers with licence restrictions had fewer traffic violations than unrestricted licence holders (19 124/23 185 [82%] v. 438 331/703 758 [62%]; p < 0.001).
Table 1
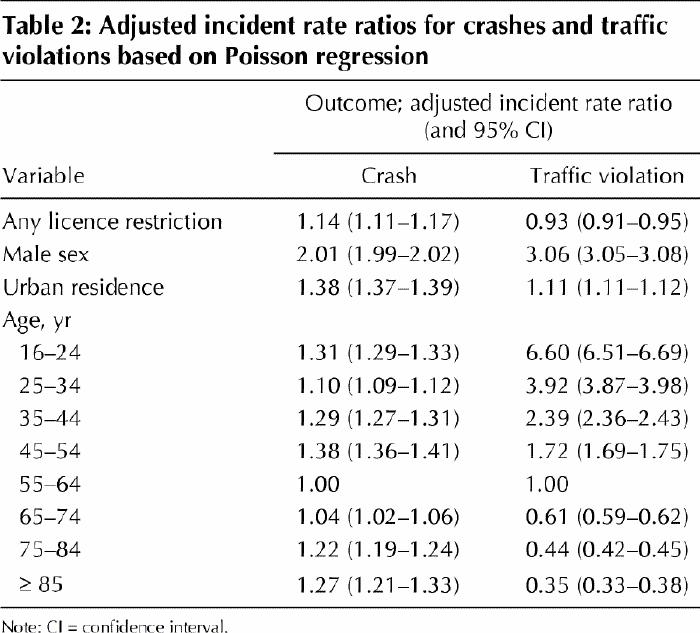
On multivariate Poisson regression, driver age, sex and residence were all significantly associated with crash and traffic violation rates (Table 2). After adjustment for these factors, drivers with any restriction (incidence rate ratio [IRR] 1.14, 95% CI 1.11–1.17), those with driving restrictions (IRR 1.18, 95% CI 1.10–1.27) and those with licensing restrictions (IRR 1.15, 95% CI 1.12–1.18) had significantly higher crash rates than drivers without restrictions. However, the increases were significantly lower than those associated with being male (adjusted IRR 2.01, 95% CI 1.99–2.02) or living in an urban area (adjusted IRR 1.38, 95% CI 1.37–1.39). In contrast, restricted licence holders had significantly lower traffic violation rates than drivers without restrictions (adjusted IRR 0.93, 95% CI 0.91–0.95). All models fit the data well.
Table 2
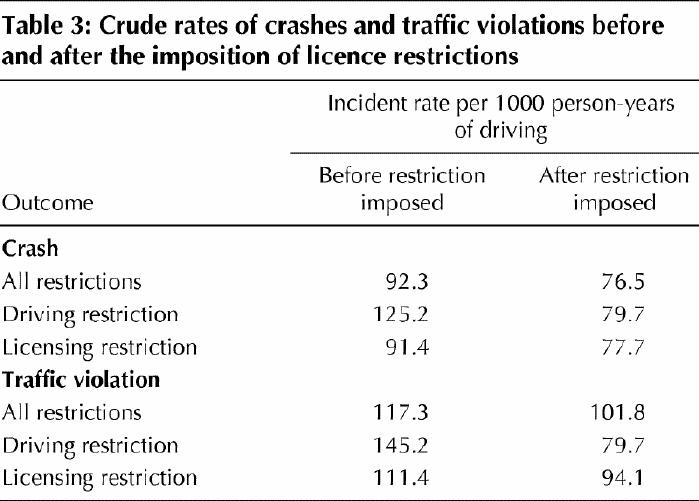
The crude rates of crashes and traffic violations before and after driving restrictions were imposed are presented in Table 3. The rates decreased following imposition of restrictions in all instances.
Table 3
The weekly crash rates during the 4 years before and the 4 years after the imposition of licence restrictions are presented in Fig. 1. With both driving and licensing restrictions combined, we observed a significant decrease of 0.2 (95% CI 0.04–0.39) crashes per 1000 drivers per week after the restrictions were imposed (p < 0.001). This translated into a relative rate reduction of 12.8% (95% CI 2.4%–23.2%). Similar results were obtained when the series were fit for driving and licensing restrictions separately. Driving restrictions alone were associated with a significant decrease of 0.7 (95% CI 0.38–1.04) crashes per 1000 drivers per week (p < 0.001) (relative rate reduction 31.8% [95% CI 17.1%–46.5%]). Licensing restrictions were associated with a smaller but still significant decrease (0.2 [95% CI 0.02–0.3] crashes per 1000 drivers per week) (p = 0.03).

Fig. 1: Time series plot of outcome rates during the 4 years before and the 4 years after the imposition of driving and licensing restrictions combined. Restrictions were imposed at year 0. Top: At-fault crash rates. Bottom: Traffic violation rates.
The weekly traffic violation rates during the 4 years before and the 4 years after the imposition of licence restrictions are shown in Fig. 1. With both types of restriction combined, there was a significant decrease of 0.2 (95% CI 0.09–0.31) traffic violations per 1000 drivers per week after the restrictions were imposed (p < 0.001) (relative rate reduction 10.0% [95% CI 4.4%–15.7%]). Driving restrictions alone did not change the rates significantly (decrease of 0.03 violations per 1000 drivers per week) (relative rate reduction 0.2% [95% CI -0.1% to 0.5%]). However, licensing restrictions were associated with a significant reduction of 0.2 (95% CI 0.08–0.31) violations per 1000 drivers per week (p < 0.001) (relative rate reduction 10.7% [95% CI 4.6%–16.9%]).
During the study period, restricted licence holders accounted for 72 410 person-years of driving. Assuming that the rates of at-fault crashes and traffic violations among these drivers would have remained stable without the restriction, we estimate that licence restrictions averted 816 crashes and 751 traffic violations during the study period.
Interpretation
Compared with the general driving population, drivers with restricted licences had a lower adjusted risk of traffic violations but a higher adjusted risk of at-fault crashes. However, the increased risk of crashes attributable to restricted licences is significantly smaller than that attributable to male sex or urban residence. Imposition of a licence restriction was associated with significantly decreased rates of crashes and traffic violations.
Our study demonstrates a statistically and clinically significant decrease in rates of crashes and traffic violations following the imposition of licence restrictions. Like Crancer and McMurray,19 we found a higher crash rate among restricted licence holders after controlling for age and sex, but we also found a lower traffic violation rate among these drivers. A report of the US National Highway and Traffic Safety Association showed an increased risk of crashes for drivers with licence restrictions.21 Our findings reflect a similar trend, but to a much smaller extent.
Despite the differences between our results and those from the United States,21 we are confident that our findings are valid, for several reasons. First, we used a cohort design, which is susceptible to fewer biases than a case–control study. Second, ours was a population-based study, which averts problems with incorrect or biased sampling. Finally, our findings were very coherent in showing that licence restrictions were associated with decreased traffic violation rates. Traffic violations are a marker of driving behaviour associated with increased risk of crashes.29,30,31
Licence restrictions may decrease crash and traffic violation rates for drivers with medical impairments in several ways. Driving restrictions may limit a driver to an environment for which he or she has the skills required for safe driving, thereby reducing exposure to more complex or higher-risk traffic situations. Driving restrictions may also change driving behaviour by highlighting limitations to the restricted driver or his or her family. Restricted licence holders may self-restrict their driving and drive less frequently or under less demanding conditions, thus decreasing their risk for traffic violations or crashes.
The primary weakness of our study was the inability to control for driving exposure, which is likely to be less for drivers with restrictions. We were also unable to measure driver compliance with restrictions. Since residence was determined as of the date the data sets were created, some driving time may have been misallocated if the driver moved during the study period. Information on crash severity was unavailable. Had these data been available, they may have influenced our interpretation of the results, since severity of the crash is the greatest concern for society. Finally, we did not explore the influence of specific driving and licensing restrictions or specific medical diagnoses on crashes.
Further prospective study is needed to determine what specific factors lead to decreased rates of crashes and traffic violations. A prospective study would also assess driving exposure, providing a true, time-based estimate of crash and violation risk. Specific driving and licensing restrictions each need to be evaluated, as do specific medical diagnoses or impairments and their different effects on rates of crashes and traffic violations. Also, further study of the appropriate timing and methods of identifying who would benefit from a restricted licence is required.
In conclusion, restricted licensing programs such as those used in Saskatchewan appear to be effective, but further study is needed to determine the most effective restrictions and the most appropriate method of implementing restrictions.
β See related articles pages 761 and 769
Acknowledgments
This research was conducted while Dr. Marshall was a postgraduate student in the Department of Epidemiology and Community Medicine, University of Ottawa. Dr. van Walraven is an Ontario Ministry of Health Career Scientist.
Footnotes
This article has been peer reviewed.
Contributors: Dr. Marshall was the principal author and was responsible for the conception and design of the study, drafting of the manuscript and data analysis. Dr. Spasoff was responsible for the conception and design of the study and data interpretation, and edited the manuscript significantly. Dr. Nair assisted in the study design and analysis and interpretation of the data. Dr. van Walraven was responsible for the study design, and analysis and interpretation of the data, and provided significant input into the drafting of the manuscript.
Competing interests: None declared.
Correspondence to: Dr. Shawn C. Marshall, The Rehabilitation Centre, 505 Smyth Rd., Ottawa ON K1H 8M2; smarshall@ottawahospital.on.ca
References
- 1.Van Zomeren AH, Brouwer WH, Minderhoud JM. Acquired brain damage and driving: a review. Arch Phys Med Rehabil 1987;68:697-705. [PubMed]
- 2.Owsley C, Ball K, McGwin G, Sloane ME, Roenker DL, White MF, et al. Visual processing impairment and risk of motor vehicle crash among older adults. JAMA 1998;279:1083-8. [DOI] [PubMed]
- 3.Kline DW, Kline TJB, Fozard JL, Kosnik W, Schieber F, Sekuler R. Vision, aging, and driving: the problems of older drivers. J Gerontol 1992;47:27-34. [DOI] [PubMed]
- 4.Wood JM, Troutbeck AJ. Effect of age and visual impairment on driving and vision performance. Transport Res Rec 2000;1438:84-90.
- 5.Waller JA. Driving patterns before and after hospitalization for heart disease. Accid Anal Prev 1987;19:105-14. [DOI] [PubMed]
- 6.Crancer AJ, O'Neall PA. A record analysis of Washington drivers with license restrictions for heart disease. Northwest Med 1970;69:409-16. [PubMed]
- 7.Cornwell M. The assessment of people with arthritis who wish to drive a car. Int Disabil Stud 1987;9:174-7. [DOI] [PubMed]
- 8.Jones JG, McCann J, Lassere MN. Driving and arthritis. Br J Rheumatol 1991; 30:361-4. [DOI] [PubMed]
- 9.Carr DB, LaBarge E, Dunnigan K, Storandt M. Differentiating drivers with dementia of the Alzheimer type from healthy older persons with a Traffic Sign Naming test. J Gerontol A Biol Sci Med Sci 1998;53:M135-9. [DOI] [PubMed]
- 10.Reuben DB, St George P. Driving and dementia: California's approach to a medical and policy dilemma. West J Med 1996;164:111-21. [PMC free article] [PubMed]
- 11.Drachman DA, Swearer JM. Driving and Alzheimer's disease: the risk of crashes. Neurology 1993;43:2448-56. [DOI] [PubMed]
- 12.O'Neill D, Neubauer K, Boyle M, Gerrard J, Surmon D, Wilcock GK. Dementia and driving. J R Soc Med 1992;85:199-202. [DOI] [PMC free article] [PubMed]
- 13.Nicholson JM, Hogan DB. Dementia and driving: a survey of Canadian geriatricians. Ann R Coll Physicians Surg Can 2000;33:157-63.
- 14.Galski T, Bruno RL, Ehle HT. Driving after cerebral damage: a model with implications for evaluation. Am J Occup Ther 1992;46:324-32. [DOI] [PubMed]
- 15.Mazer BL, Korner-Bitensky NA, Sofer S. Predicting ability to drive after stroke. Arch Phys Med Rehabil 1998;79:743-50. [DOI] [PubMed]
- 16.Kumar R, Powell B, Tani N, Naliboff B, Metter EJ. Perceptual dysfunction in hemiplegia and automobile driving. Gerontologist 1991;31:807-10. [DOI] [PubMed]
- 17.Sundet K, Goffeng L, Hofft E. To drive or not to drive: neuropsychological assessment for driver's license among stroke patients. Scand J Psychol 1995; 36: 47-58. [DOI] [PubMed]
- 18.Graduated driver licensing: creating mobility choices. Washington: American Association of Retired Persons; 1993. p. 4-8.
- 19.Crancer AJ, McMurray L. Accident and violation rates of Washington's medically restricted drivers. JAMA 1968;205:74-8.5694871
- 20.Stutts JC, Martell C. Older driver population and crash involvement trends, 1974–1988. Accid Anal Prev 1992;24:317-27. [DOI] [PubMed]
- 21.Diller E, Cook L, Leonard D, Reading J, Deon JM, Vernon D. Evaluating drivers licensed with medical conditions in Utah, 1992–1996. Springfield (VA): US Dept of Transportation; 1999. DOT HS 809 023. p. 1-43.
- 22.Petrucelli E, Malinowski M. Status of medical review in driver licensing: policies, programs and standards. Springfield (VA): National Highway Traffic Safety Administration, US Dept of Transportation; 1992. DOT HS 807 892. p. 98-222.
- 23.Marshall S, Gilbert N. Saskatchewan physicians' knowledge and attitudes regarding assessment of medical fitness to drive. CMAJ 1999;160:1701-4. [PMC free article] [PubMed]
- 24.Medgyesi M, Koch D. Medical impairments to driving. Regina: Saskatchewan Government Insurance; 1994. p. 50-2.
- 25.Miller TR, Lestina DC, Spicer RS. Highway crash costs in the United States by driver age, blood alcohol level, victim age, and restraint use. Accid Anal Prev 1998;30:137-50. [DOI] [PubMed]
- 26.Voas RB, Tippetts AS, Lange JE. Evaluation of a method for reducing unlicensed driving: the Washington and Oregon license plate sticker laws. Accid Anal Prev 1997;29:627-34. [DOI] [PubMed]
- 27.Van Walraven C, Goel V, Chan B. Effect of population-based interventions on laboratory utilization: a time series analysis. JAMA 1998;280:2028-33. [DOI] [PubMed]
- 28.Introduction to ARIMA: nonseasonal models. Available: www.geocities.com/Colosseum/5585/mprev.html (accessed 2002 Aug 23).
- 29.Panek PWE. Hand test personality variables related to automotive moving violations in female drivers. J Pers Assess 1986;50:208-11. [DOI] [PubMed]
- 30.Lourens PF, Vissers JA, Jessurun M. Annual mileage, driving violations, and accident involvement in relation to drivers' sex, age, and level of education. Accid Anal Prev 1901;31:593-7. [DOI] [PubMed]
- 31.West R, Elander J, French D. Mild social deviance, Type-A behaviour pattern and decision-making style as predictors of self-reported driving style and traffic accident risk. Br J Psychol 1993;84(pt 2):207-19. [DOI] [PubMed]