

Abstract
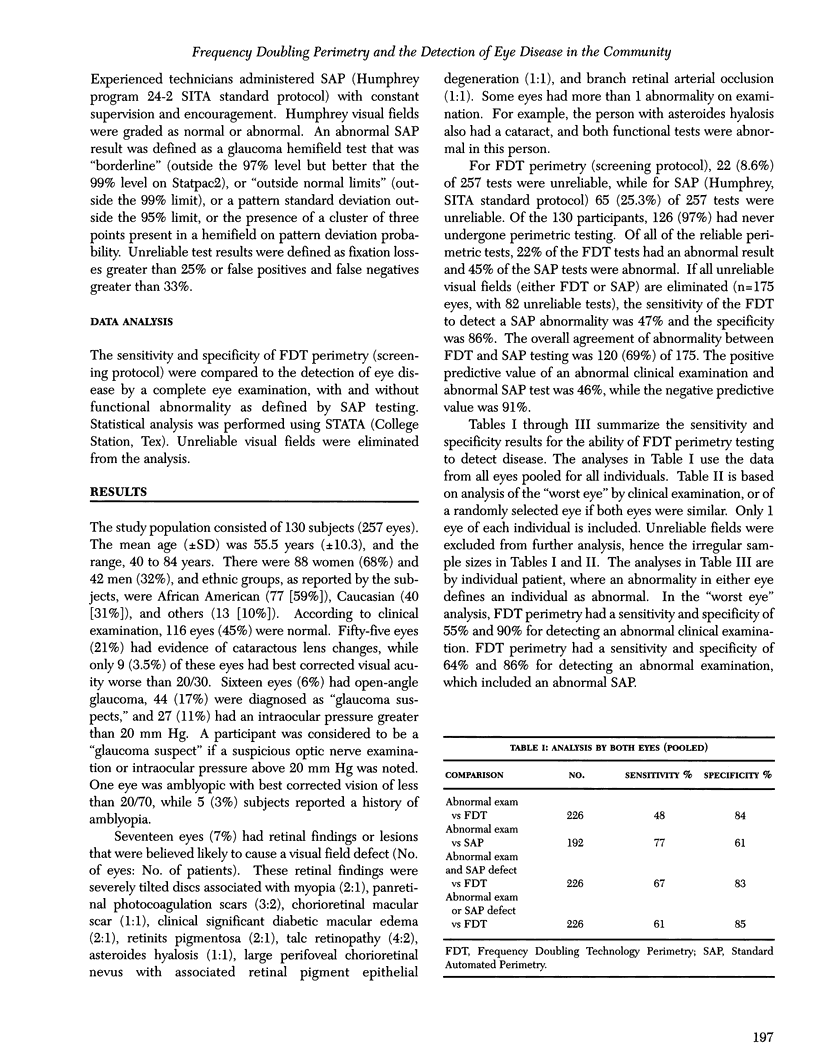
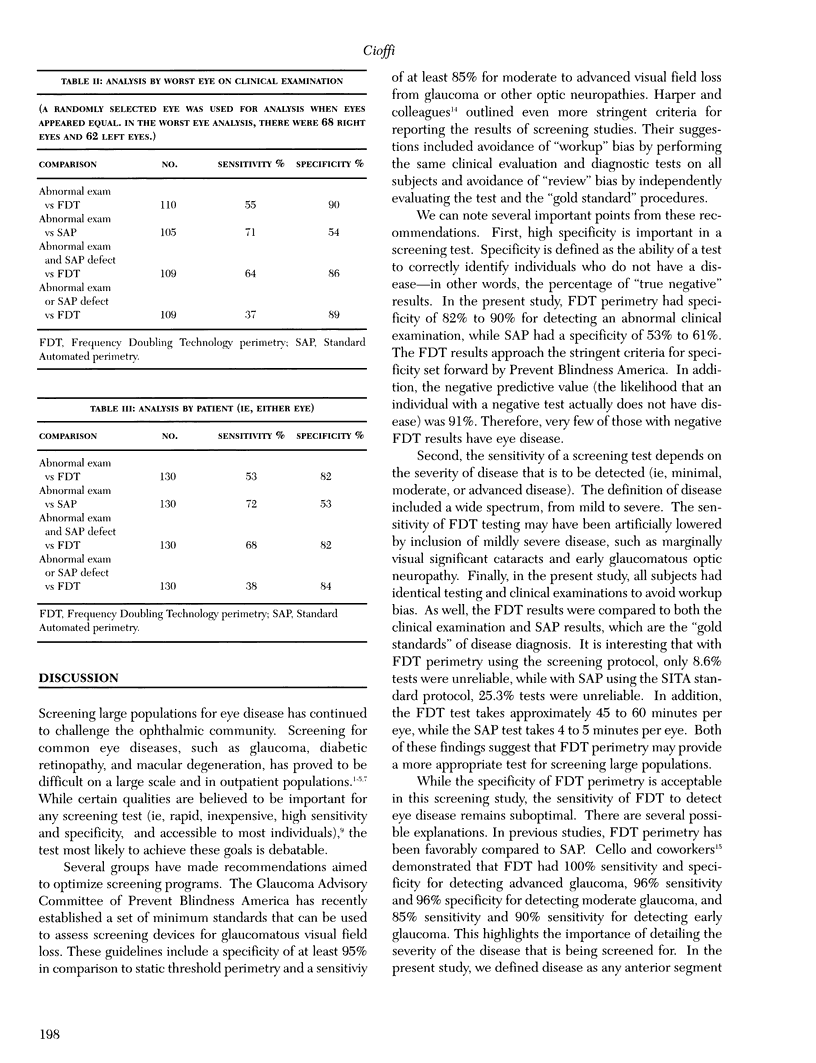
PURPOSE: Frequency Doubling Technology (FDT) perimetry is a novel perimetric test that provides rapid screening (45 to 60 seconds) and full-threshold (4 to 5 minutes) testing for detection of vision loss. The purpose of this study was to determine the specificity and sensitivity of FDT perimetry for the detection of ocular disease. METHODS: A total of 130 participants (257 eyes of 42 men and 88 women) recruited from the community completed FDT perimetry, standard achromatic automated perimetry (SAP), anterior segment biomicroscopy, tonometry, and dilated ophthalmoscopy. FDT results were considered abnormal if 1 point was abnormal (depressed below the 5% level on the screening protocol C-20-5). SAP was considered abnormal if the glaucoma hemifield test or pattern standard deviation was outside normal limits (P < .05) or a hemifield cluster of 3 depressed points on the pattern deviation probability plot (P < .05) was present. An abnormal eye examination was defined as the presence of an abnormality in the anterior segment, lens, or posterior segment that was likely to cause a visual field defect or the presence of glaucomatous or other optic neuropathy. RESULTS: The mean age (+/- SD) of participants was 55.5 years (+/- 10.3). Ethnic groups, as reported by participants, included 77 (59%) African Americans, 40 (31%) Caucasians, and 13 (10%) in other groups. On clinical examination, 116 eyes (45%) were normal, 9 eyes (3.5%) had a cataract with best corrected visual acuity worse than 20/30, 16 eyes (6%) had open-angle glaucoma, and 17 eyes (7%) had retinal findings or lesions that were likely to cause a visual field defect. For FDT perimetry, 22 (8.6%) of 257 tests were unreliable, and for SAP, 65 (25.3%) of 257 tests were unreliable. The sensitivity and specificity of FDT perimetry for detecting an abnormal clinical examination were 55% and 90% and for detecting an abnormal examination that included an abnormal SAP, 64% and 86%. CONCLUSIONS: FDP demonstrated reasonable discriminatory power for detecting eye disease.
Full text
PDF




Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Adab P. Screening for sight threatening eye disease. Cost effectiveness of screening modalities must be determined. BMJ. 1996 Feb 17;312(7028):440–441. doi: 10.1136/bmj.312.7028.440a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brusini P., Busatto P. Frequency doubling perimetry in glaucoma early diagnosis. Acta Ophthalmol Scand Suppl. 1998;(227):23–24. doi: 10.1111/j.1600-0420.1998.tb00869.x. [DOI] [PubMed] [Google Scholar]
- Cello K. E., Nelson-Quigg J. M., Johnson C. A. Frequency doubling technology perimetry for detection of glaucomatous visual field loss. Am J Ophthalmol. 2000 Mar;129(3):314–322. doi: 10.1016/s0002-9394(99)00414-6. [DOI] [PubMed] [Google Scholar]
- Grey R. H., Hart J. C. Screening for sight threatening eye disease. Stereoscopic viewing of the retina needed to identify maculopathy. BMJ. 1996 Feb 17;312(7028):440–441. doi: 10.1136/bmj.312.7028.440b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harding S. P., Broadbent D. M., Neoh C., White M. C., Vora J. Sensitivity and specificity of photography and direct ophthalmoscopy in screening for sight threatening eye disease: the Liverpool Diabetic Eye Study. BMJ. 1995 Oct 28;311(7013):1131–1135. doi: 10.1136/bmj.311.7013.1131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harper R., Reeves B. Compliance with methodological standards when evaluating ophthalmic diagnostic tests. Invest Ophthalmol Vis Sci. 1999 Jul;40(8):1650–1657. [PubMed] [Google Scholar]
- Hickey-Dwyer M., Ellerby S. Screening for sight threatening eye disease. Calculation of sensitivity is misleading. BMJ. 1996 Feb 17;312(7028):440–441. doi: 10.1136/bmj.312.7028.440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iester M., Mermoud A., Schnyder C. Frequency doubling technique in patients with ocular hypertension and glaucoma: correlation with octopus perimeter indices. Ophthalmology. 2000 Feb;107(2):288–294. doi: 10.1016/s0161-6420(99)00058-5. [DOI] [PubMed] [Google Scholar]
- Johnson C. A., Cioffi G. A., Van Buskirk E. M. Frequency doubling technology perimetry using a 24--2 stimulus presentation pattern. Optom Vis Sci. 1999 Aug;76(8):571–581. doi: 10.1097/00006324-199908000-00026. [DOI] [PubMed] [Google Scholar]
- Johnson C. A., Samuels S. J. Screening for glaucomatous visual field loss with frequency-doubling perimetry. Invest Ophthalmol Vis Sci. 1997 Feb;38(2):413–425. [PubMed] [Google Scholar]
- Katz J., Tielsch J. M., Quigley H. A., Javitt J., Witt K., Sommer A. Automated suprathreshold screening for glaucoma: the Baltimore Eye Survey. Invest Ophthalmol Vis Sci. 1993 Nov;34(12):3271–3277. [PubMed] [Google Scholar]
- Mills R. P. Glaucoma screening as a vehicle for providing continuing medical education. Acad Med. 2000 Jan;75(1):91–91. doi: 10.1097/00001888-200001000-00023. [DOI] [PubMed] [Google Scholar]
- Quigley H. A. Identification of glaucoma-related visual field abnormality with the screening protocol of frequency doubling technology. Am J Ophthalmol. 1998 Jun;125(6):819–829. doi: 10.1016/s0002-9394(98)00046-4. [DOI] [PubMed] [Google Scholar]
- Rhatigan M. C., Leese G. P., Ellis J., Ellingford A., Morris A. D., Newton R. W., Roxburgh S. T. Blindness in patients with diabetes who have been screened for eye disease. Eye (Lond) 1999 Apr;13(Pt 2):166–169. doi: 10.1038/eye.1999.44. [DOI] [PubMed] [Google Scholar]
- Sponsel W. E., Arango S., Trigo Y., Mensah J. Clinical classification of glaucomatous visual field loss by frequency doubling perimetry. Am J Ophthalmol. 1998 Jun;125(6):830–836. doi: 10.1016/s0002-9394(98)00047-6. [DOI] [PubMed] [Google Scholar]
- Tuck M. W., Crick R. P. The cost-effectiveness of various modes of screening for primary open angle glaucoma. Ophthalmic Epidemiol. 1997 Mar;4(1):3–17. doi: 10.3109/09286589709058056. [DOI] [PubMed] [Google Scholar]
- Yamada N., Chen P. P., Mills R. P., Leen M. M., Lieberman M. F., Stamper R. L., Stanford D. C. Screening for glaucoma with frequency-doubling technology and Damato campimetry. Arch Ophthalmol. 1999 Nov;117(11):1479–1484. doi: 10.1001/archopht.117.11.1479. [DOI] [PubMed] [Google Scholar]