

Abstract
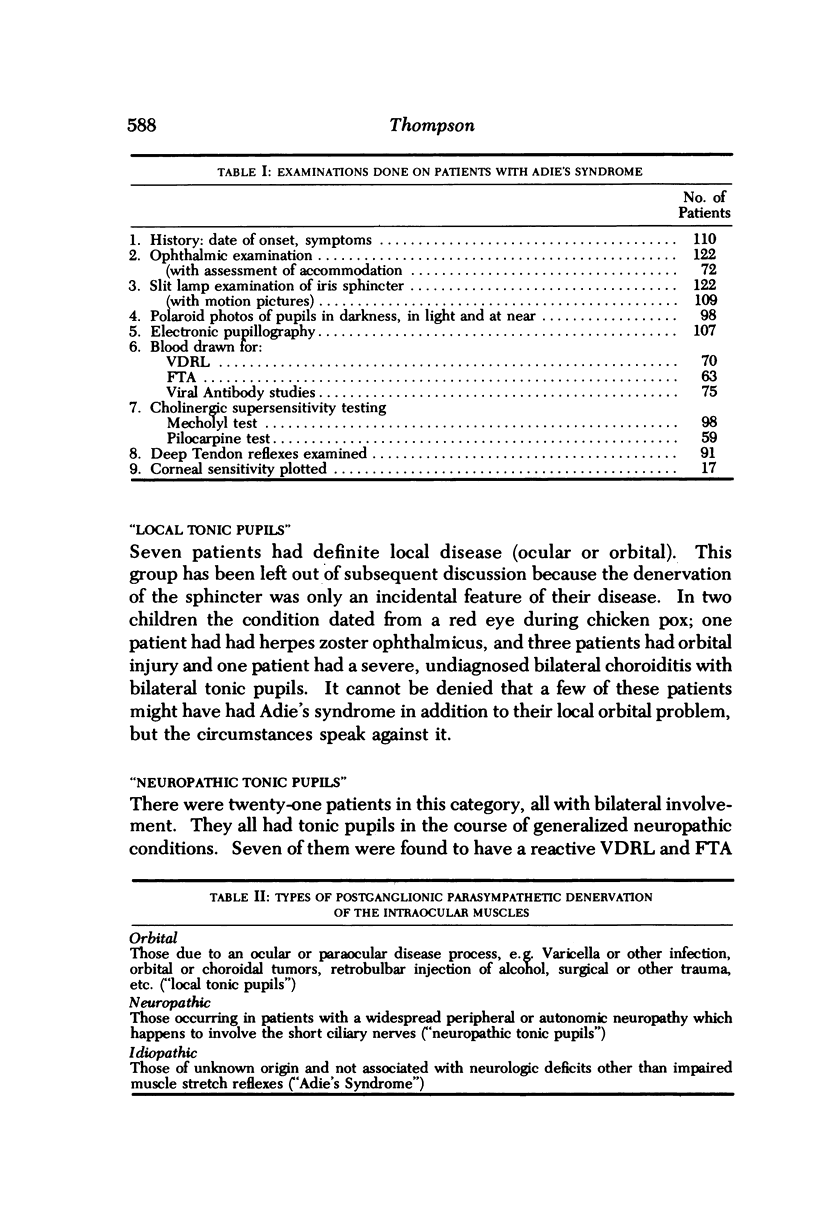
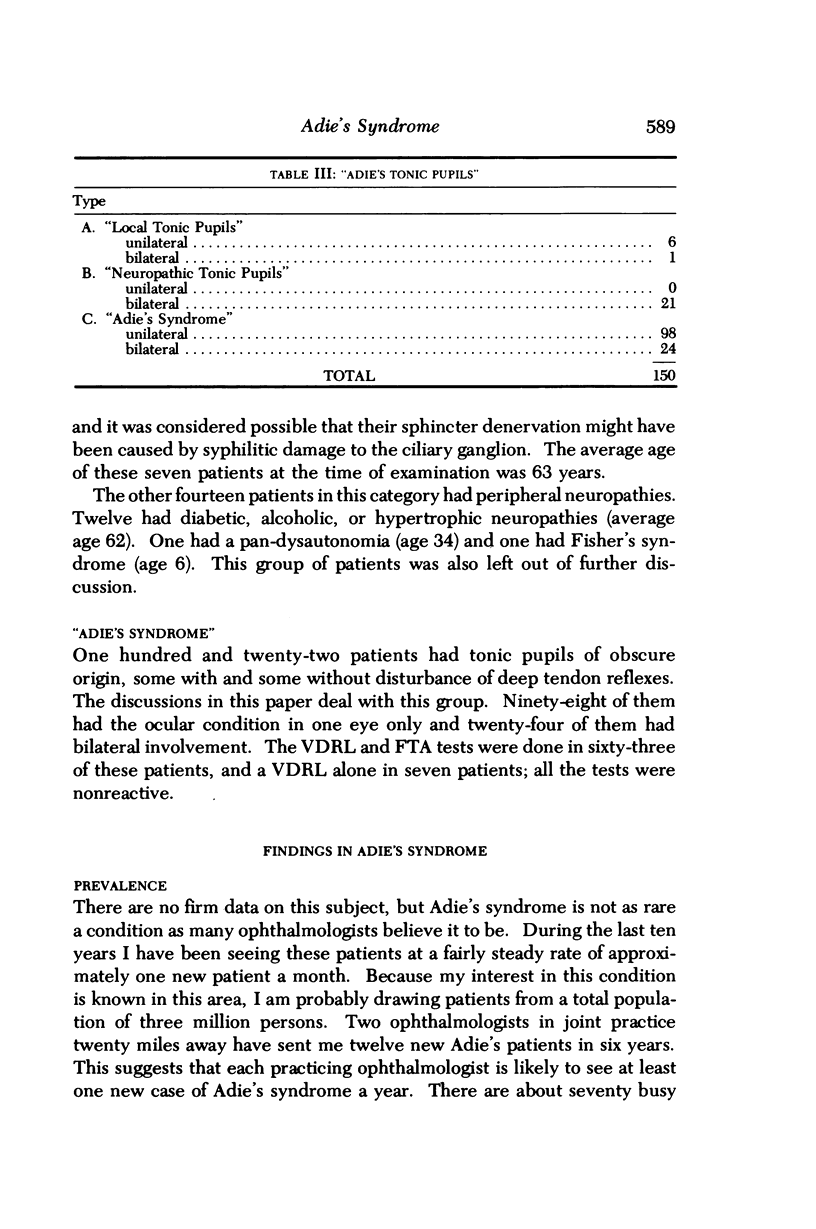
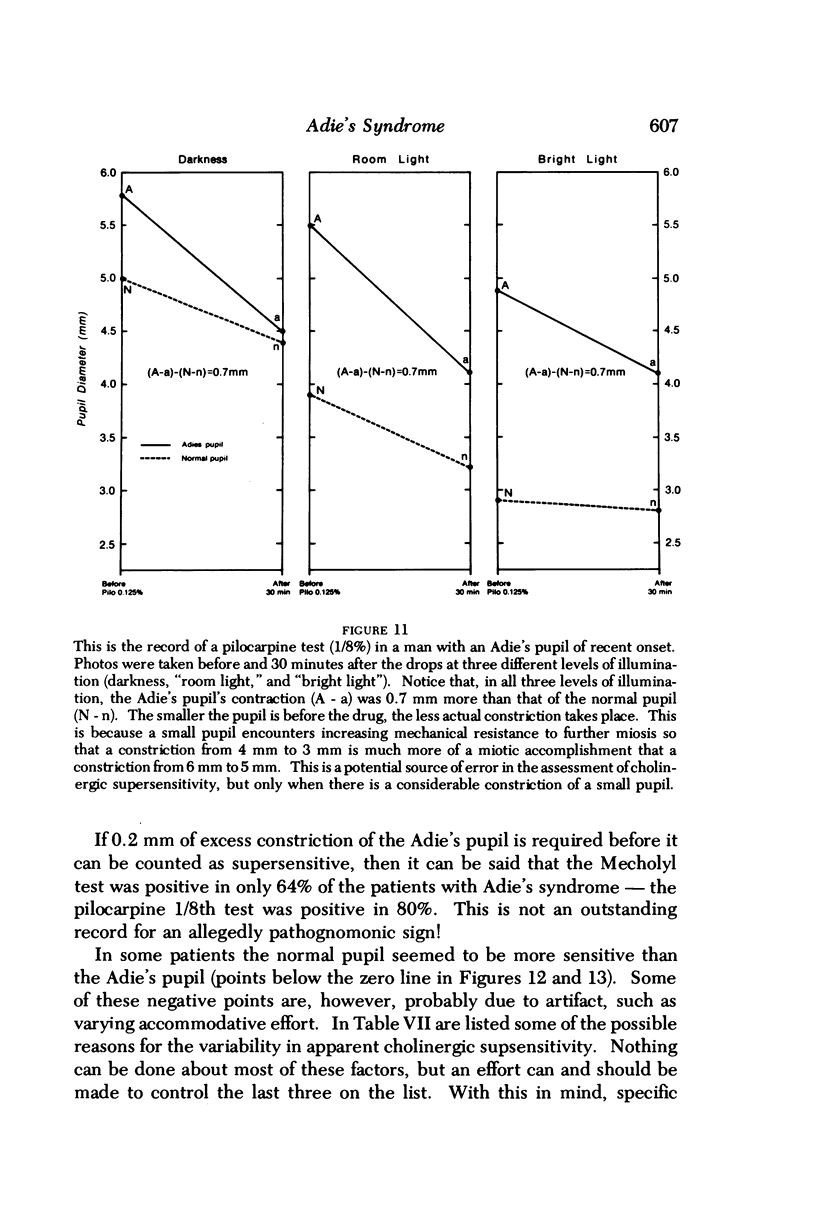
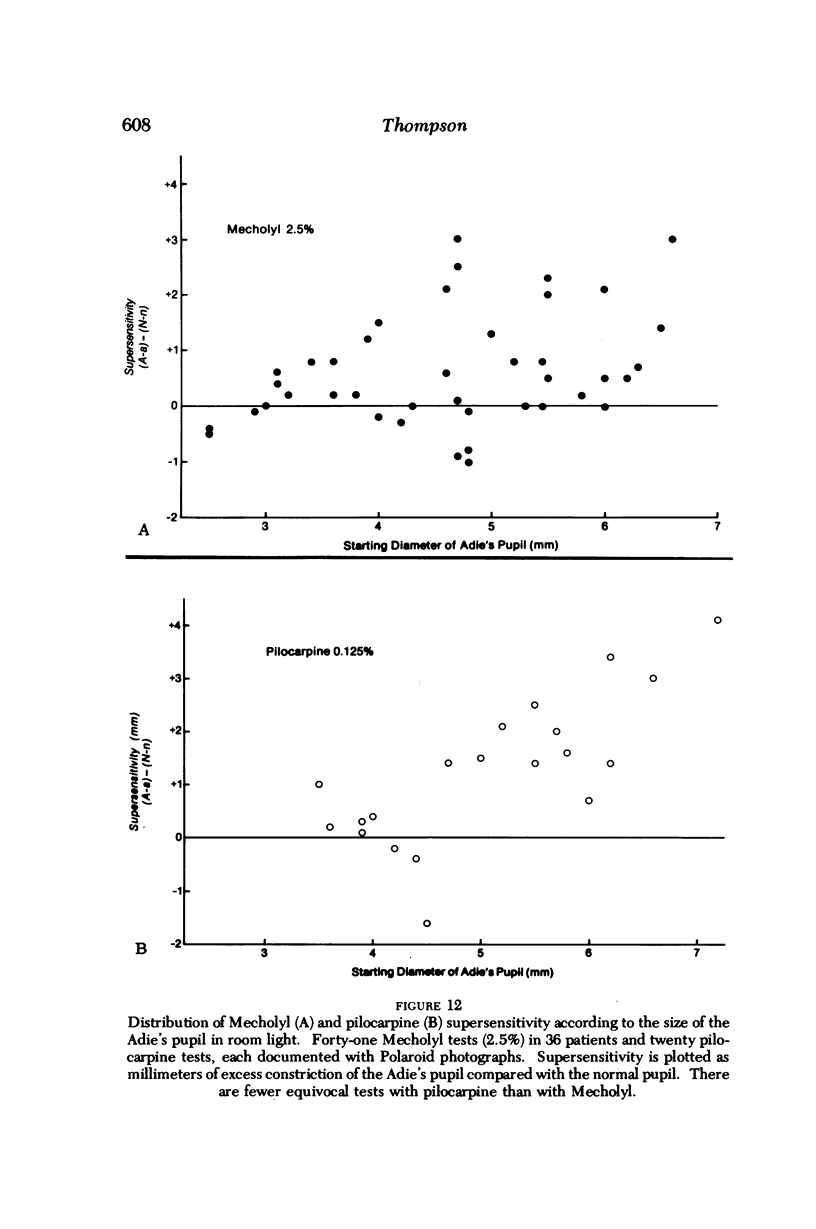
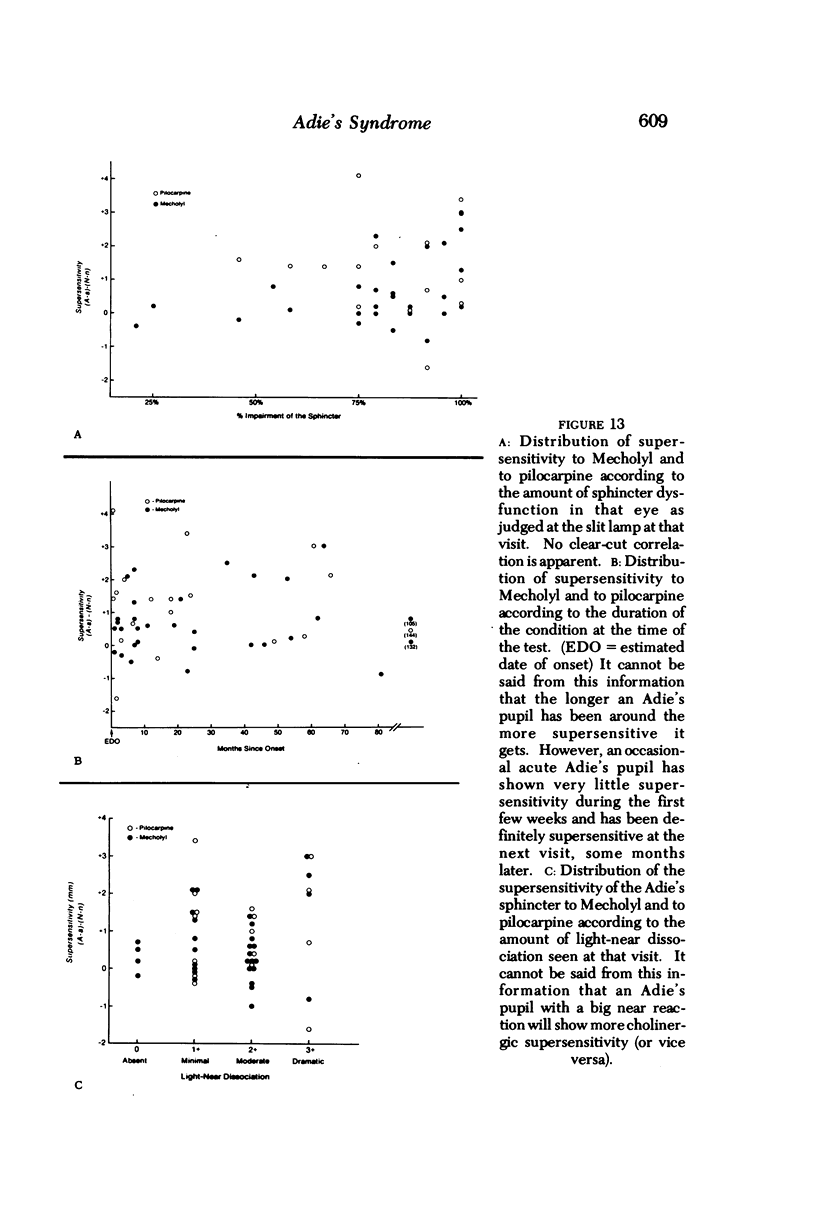
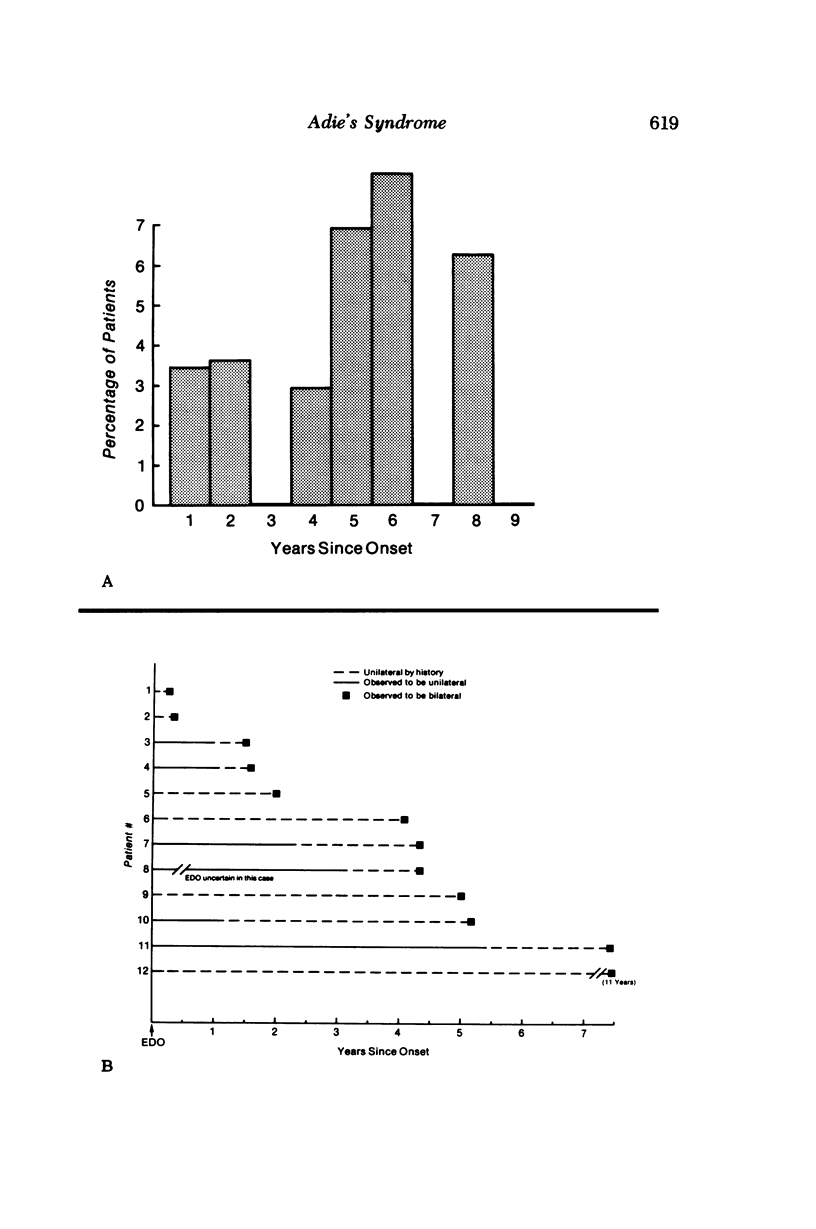
Adie's syndrome is a disease of unknown etiology. We known where the damage is, and which nerves are involved. We even know something of how the nerves react after the damage is done, but we don't known what causes the primary injury. The first step in working a jigsaw puzzle is to getall of the pieces right side up and take a good look at them. Some of the jigsaw pieces handled in this paper are listed below. Some of them are new observations; many of them are old concepts, partly modified and partly made secure by new facts. 1. Not all "tonic pupils" are due to "Adie's syndrome"; some are due to local injury and some to a generalized peripheral neuropathy (Table II). 2. All patients should have serologic tests for shyphilis. In this series one in six had positive serology. 3. The incidence of Adie's syndrome in Iowa in the early 1970's was approximately 4.7 per 100,000 population per year. 4. The prevalence of Adie's syndrome, therefore, was approximately 2 per 1000. 5. The mean age of onset of Adie's syndrome was about 32.2 years (Figure 1A). 6. The sex ratio was 2.6 females to each male. 7. Right eyes and left eyes were involved at approximately the same rate (Figure 2). 8. The incidence of second eye involvement in unilateral cases was about 4% per year during the first decade of the disease (Figure 18). 9. If this rate of second eye involvement (4% per year) persists during subsequent decades, then most Adie's pupils will eventually become bilateral. 10. The incidence of Adie's syndrome in a largely caucasian patient group is independent of iris color (Figure 4). 11. Only 10% of patients with Adie's syndrome had completely normal muscle stretch reflexes. 12. The muscle stretch reflexes in the arms were just as frequently imparied as those in th elegs, but the degree of impariment tended to be more severe in the ankles and triceps. 13. When there was any light reaction remaining in an Adie's pupil, a segmental paralysis of the sphincter muscle could be seen. 14. The near reaction of the pupil was often segmental and frequently involved segments which did not respond to light. 15. The segmental paralysis to light was randomly distributed around the sphincter (Figure 6B). 16. There was some tendency for the sphincter palsy to gradually become worse. This progression was also random (Figure 8). 17. Almost all patients with Adie's syndrome had an accommodative paresis at the time of onset. 18. Reading glasses given to a patient with a fresh Adie's pupil were soon discarded as accommodation recovered (Figure 9). 19. Accomodative effort induced an astigmatism in about half of the eyes with Adie's--presumably the result of a segmental palsy of the ciliary muscle. 20. Tonicity of accommodation was present in about 1/2 of the eyes with Adie's, making it difficut for the patient to maintain a steady level of ciliary muscle tone. 21. An occasional patient complained of brow ache from ciliary spasm with near work. 22. In most patients with Adie's syndrome the ciliary muscle was supersensitive to pilocarpine 0...
Full text
PDF
Selected References
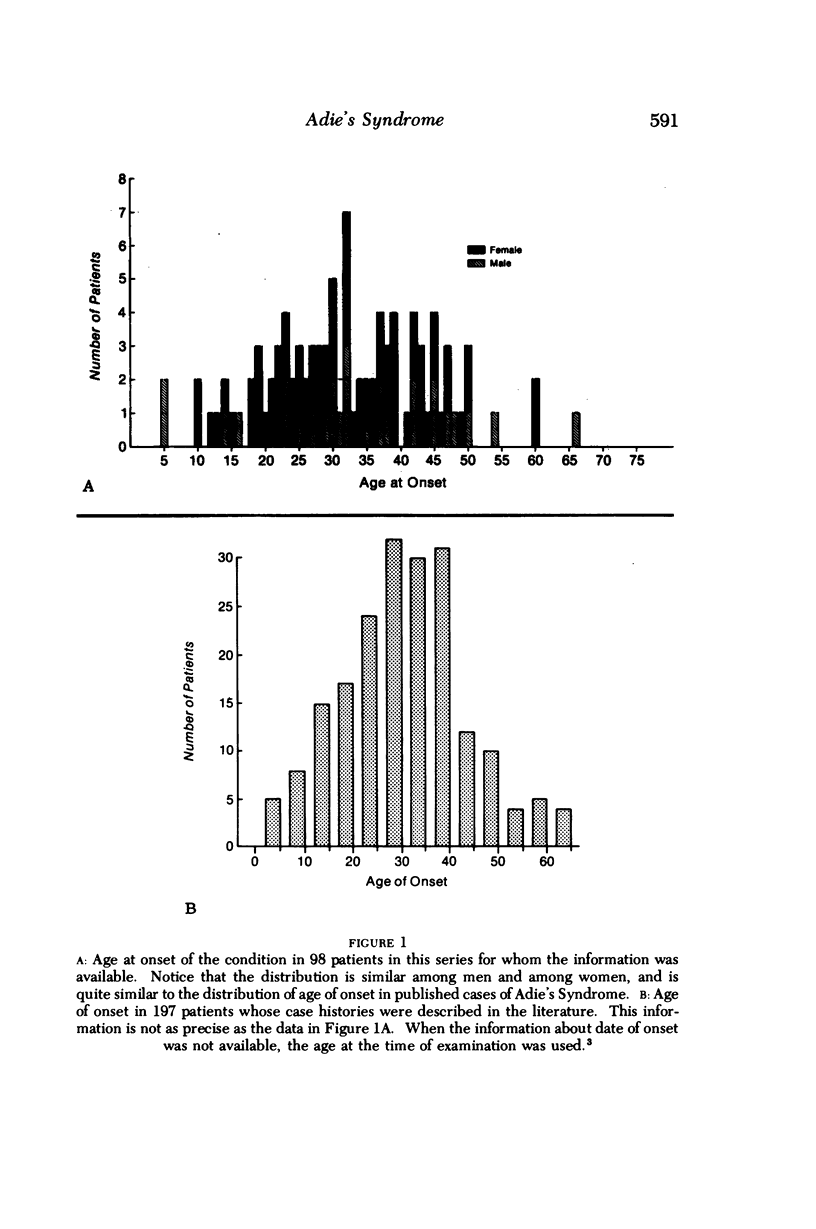
These references are in PubMed. This may not be the complete list of references from this article.
- Adie W. J. COMPLETE AND INCOMPLETE FORMS OF THE BENIGN DISORDER CHARACTERISED BY TONIC PUPILS AND ABSENT TENDON REFLEXES. Br J Ophthalmol. 1932 Aug;16(8):449–461. doi: 10.1136/bjo.16.8.449. [DOI] [PMC free article] [PubMed] [Google Scholar]
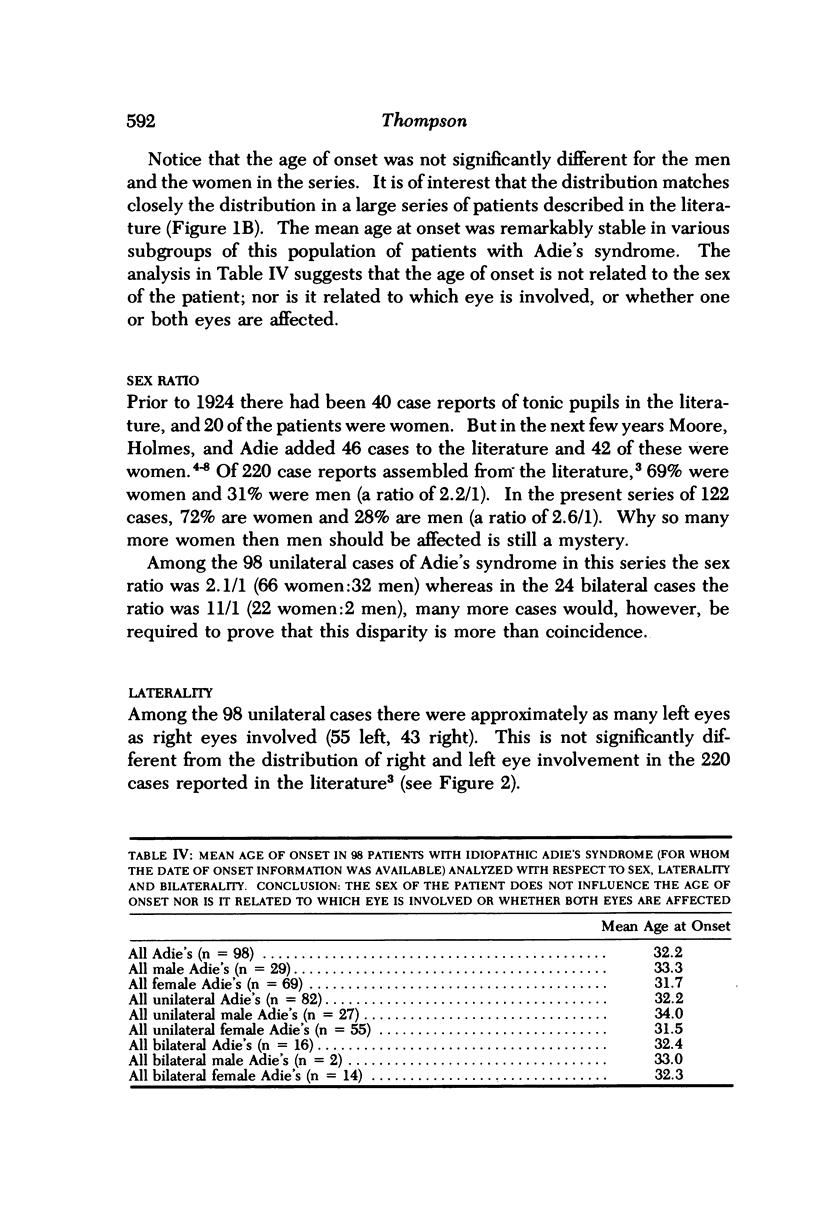
- Anderson H. K. The paralysis of involuntary muscle: Part II. On paralysis of the sphincter of the pupil with special reference to paradoxical constriction and the functions of the ciliary ganglion. J Physiol. 1905 Nov 9;33(2):156–174. doi: 10.1113/jphysiol.1905.sp001117. [DOI] [PMC free article] [PubMed] [Google Scholar]
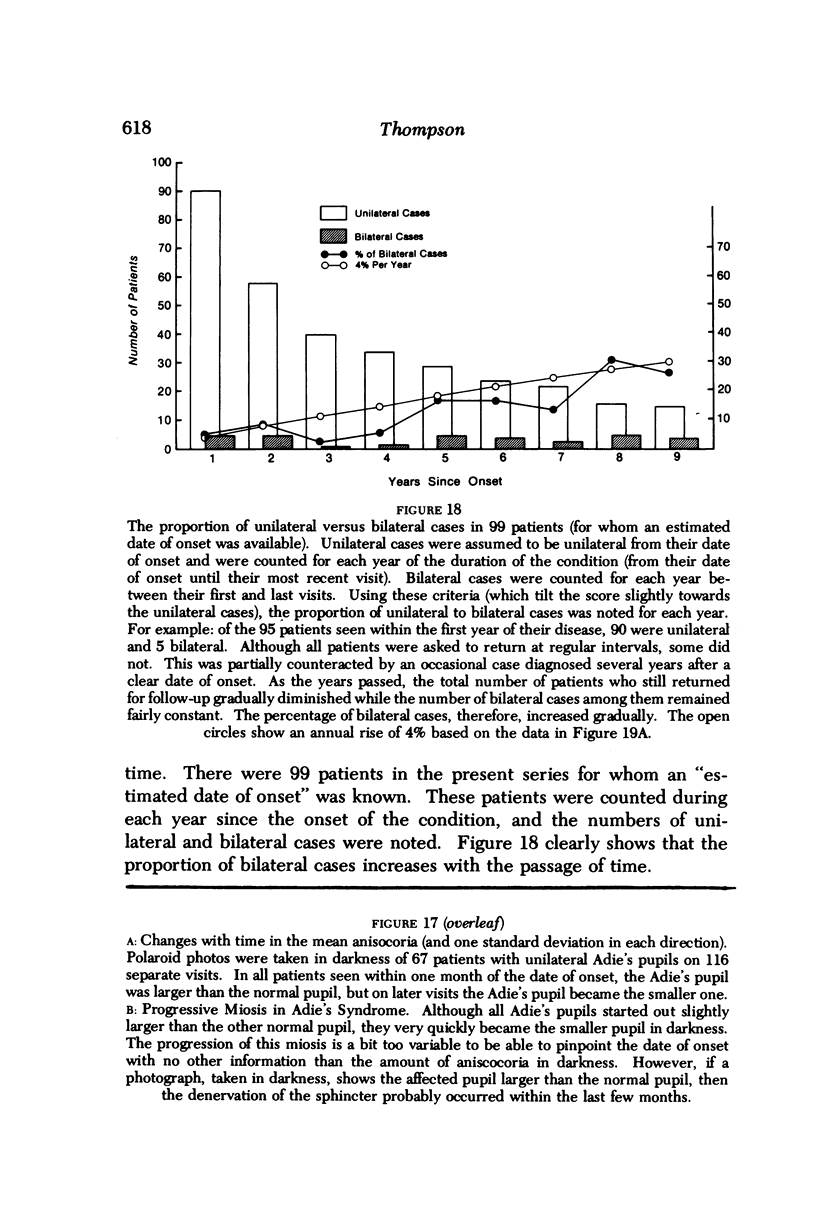
- Anderson H. K. The paralysis of involuntary muscle: Part III. On the action of pilocarpine, physostigmine, and atropine upon the paralysed iris. J Physiol. 1905 Dec 30;33(4-5):414–438. doi: 10.1113/jphysiol.1905.sp001129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen D. N., Zakov Z. N. The diagnosis of Adie's pupil using 0.0625% pilocarpine solution. Am J Ophthalmol. 1975 May;79(5):883–885. doi: 10.1016/0002-9394(75)90753-9. [DOI] [PubMed] [Google Scholar]
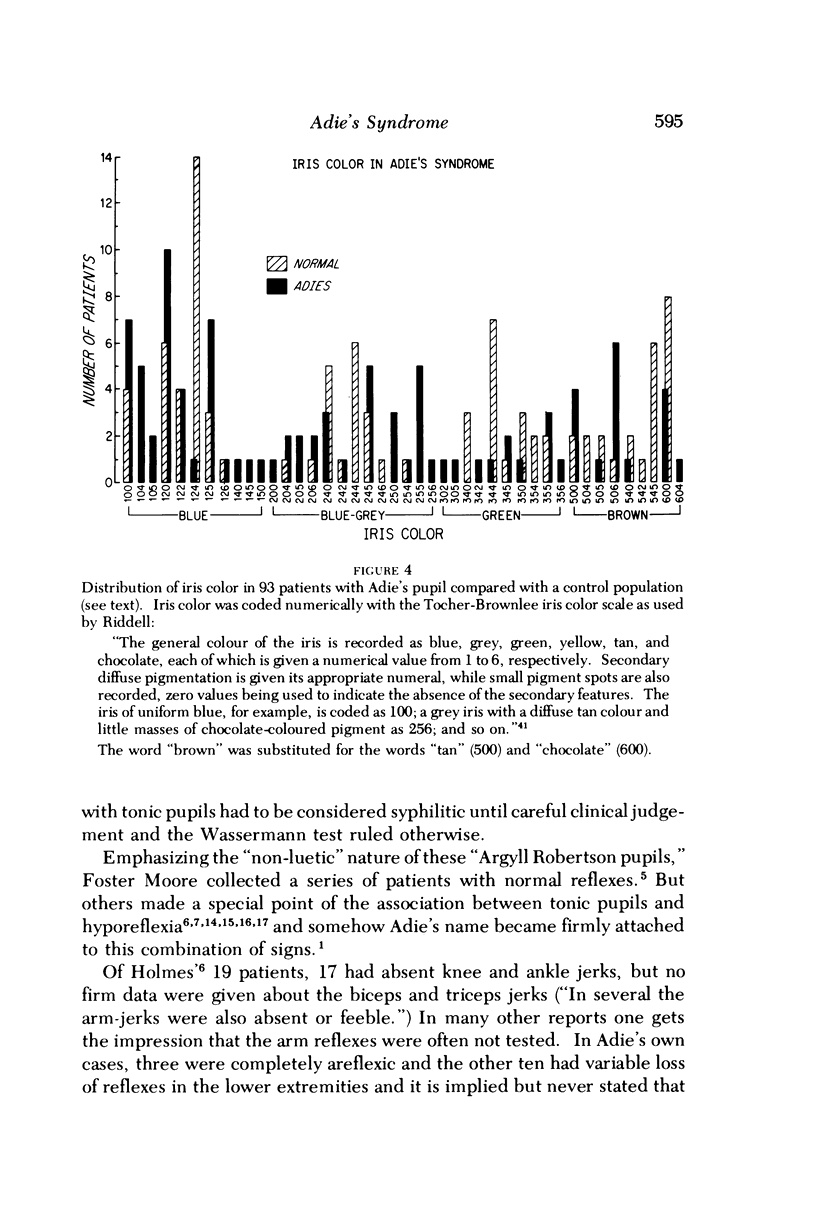
- Harriman D. G., Garland H. The pathology of Adie's syndrome. Brain. 1968 Sep;91(3):401–418. doi: 10.1093/brain/91.3.401. [DOI] [PubMed] [Google Scholar]
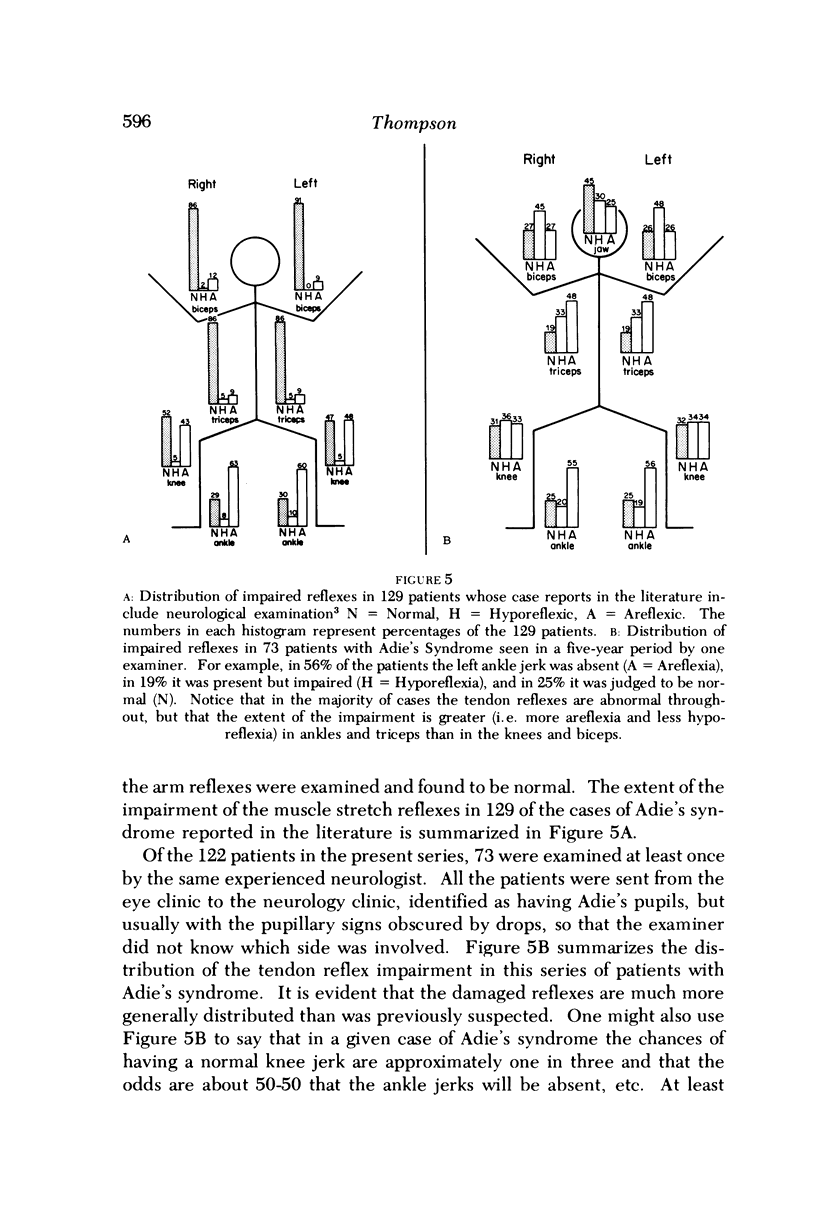
- Harriman D. G. Pathological aspects of Adie's syndrome. Adv Ophthalmol. 1970;23:55–73. [PubMed] [Google Scholar]
- LOWENSTEIN O., LOEWENFELD I. E. PUPILLOTONIC PSEUDOTABES (SYNDROME OF MARKUS-WEILL AND REYS-HOLMES-AIDE). A CRITICAL REVIEW OF THE LITERATURE. Surv Ophthalmol. 1965 Apr;10:129–185. [PubMed] [Google Scholar]
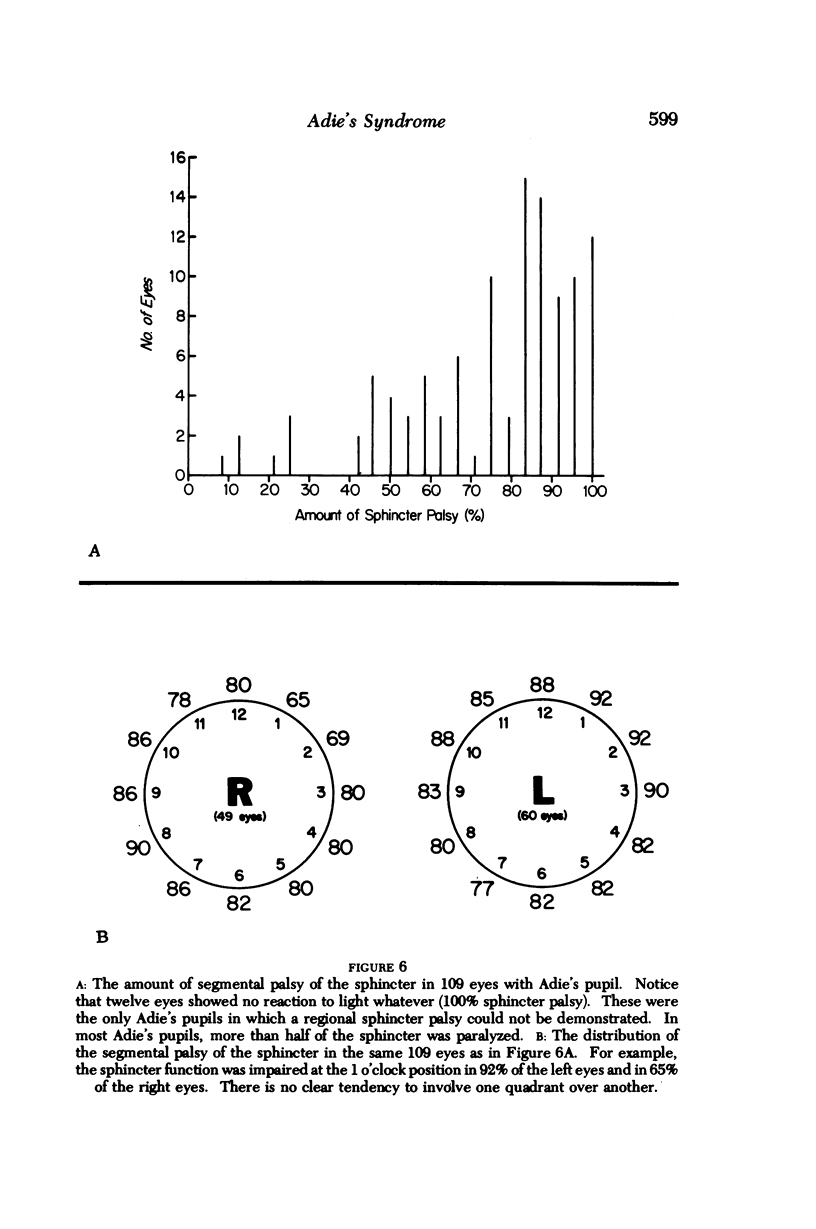
- Laties A. M., Scheie H. G. Adie's syndrome: duration of methacholine sensitivity. Arch Ophthalmol. 1965 Oct;74(4):458–459. doi: 10.1001/archopht.1965.00970040460004. [DOI] [PubMed] [Google Scholar]
- Loewenfeld I. E., Oono S. The iris as pharmacologic indicator. The supposed instability of mecholyl. Eye Ear Nose Throat Mon. 1966 Oct;45(10):69–passim. [PubMed] [Google Scholar]
- Loewenfeld I. E., Thompson H. S. The tonic pupil: a re-evaluation. Am J Ophthalmol. 1967 Jan;63(1):46–87. doi: 10.1016/0002-9394(67)90579-x. [DOI] [PubMed] [Google Scholar]
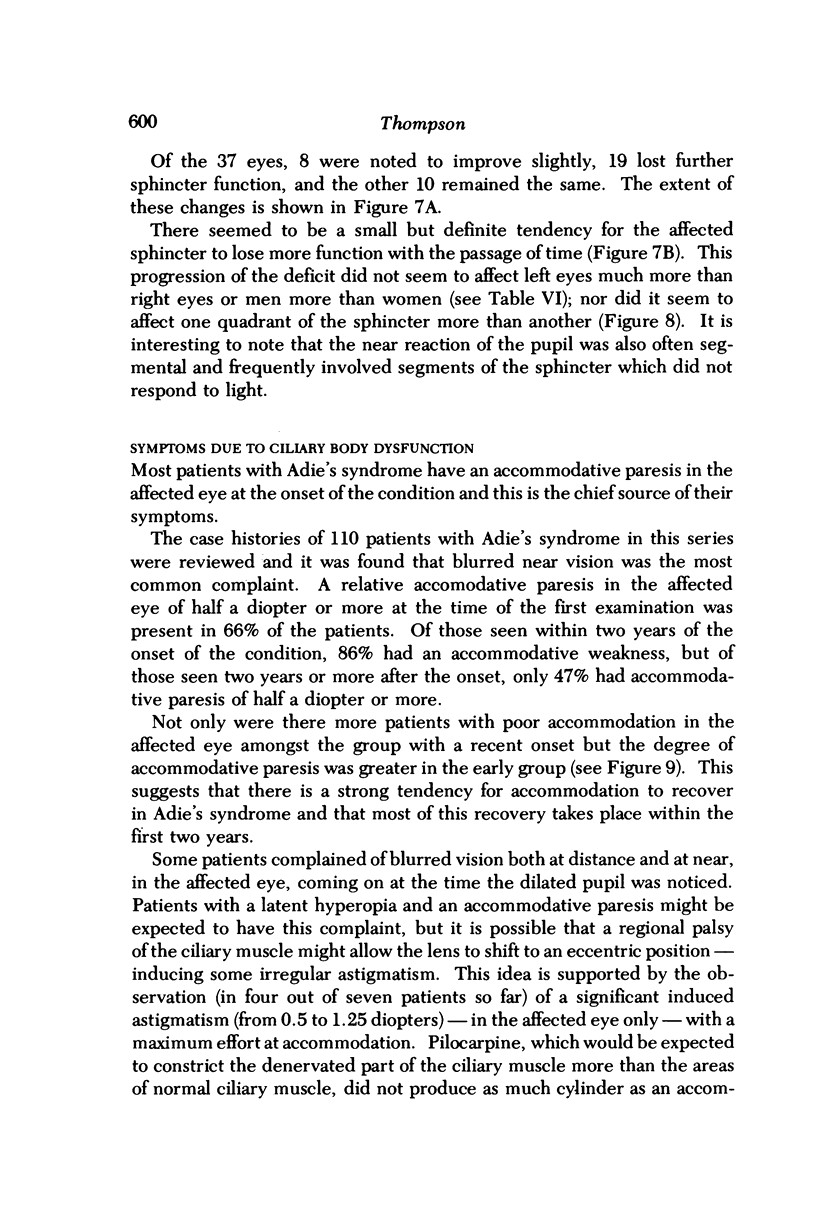
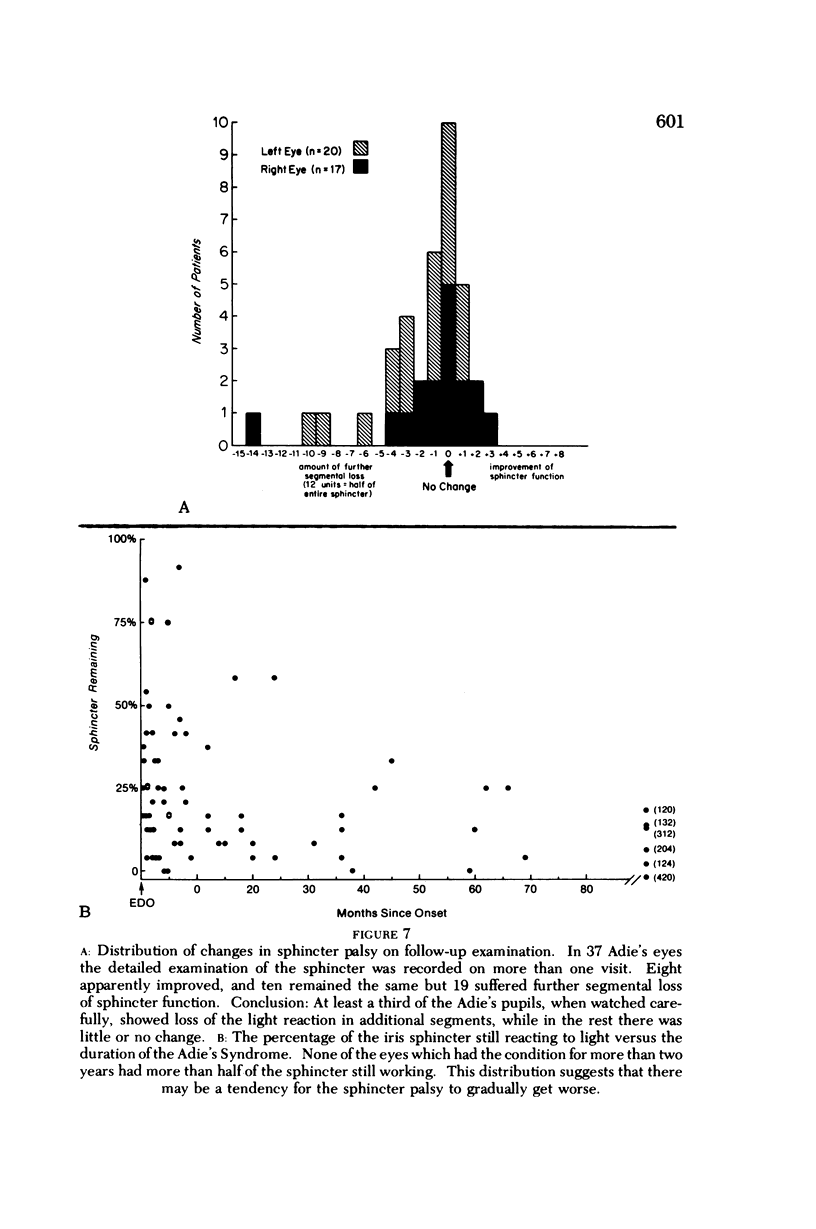
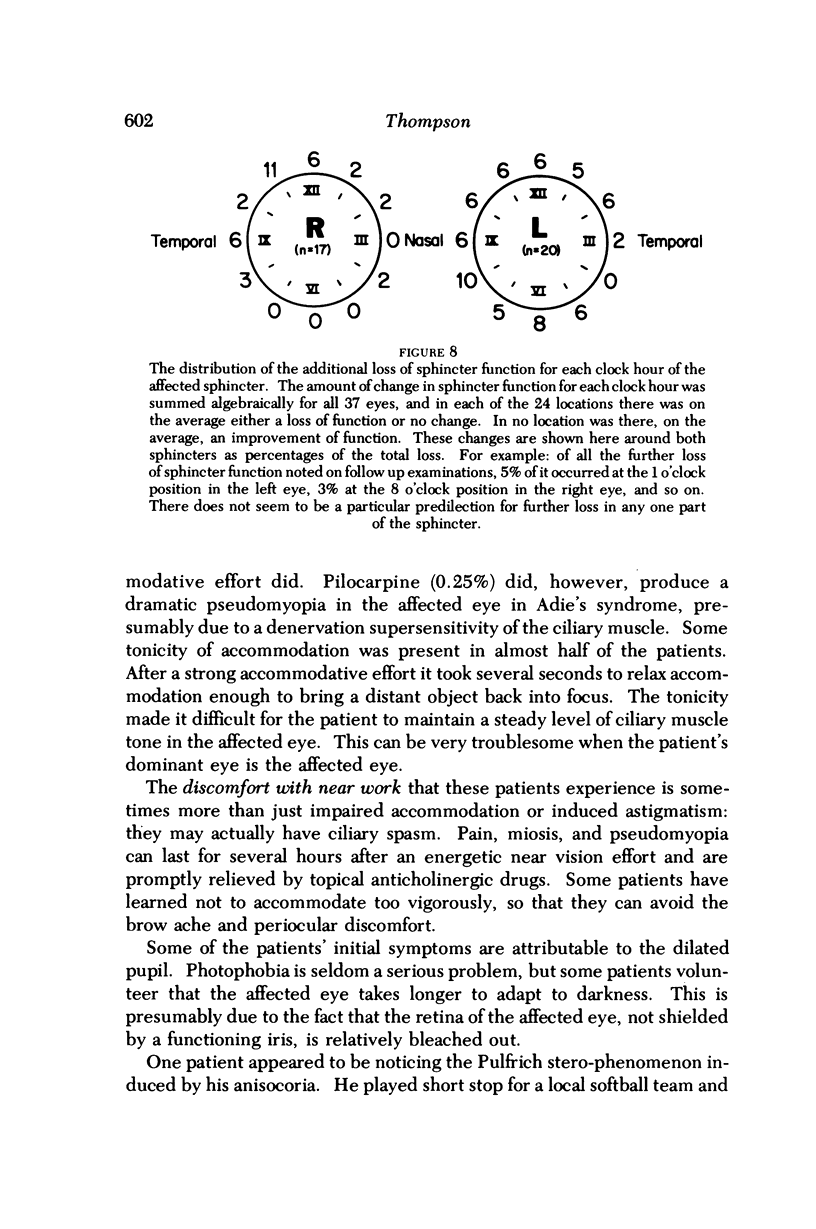
- McGregor I. S. Segmental Movement of the Pupil. Br Med J. 1945 May 5;1(4400):629–630. doi: 10.1136/bmj.1.4400.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wellings P. C. A new ocular syndrome. Br J Ophthalmol. 1968 Jul;52(7):555–559. doi: 10.1136/bjo.52.7.555. [DOI] [PMC free article] [PubMed] [Google Scholar]
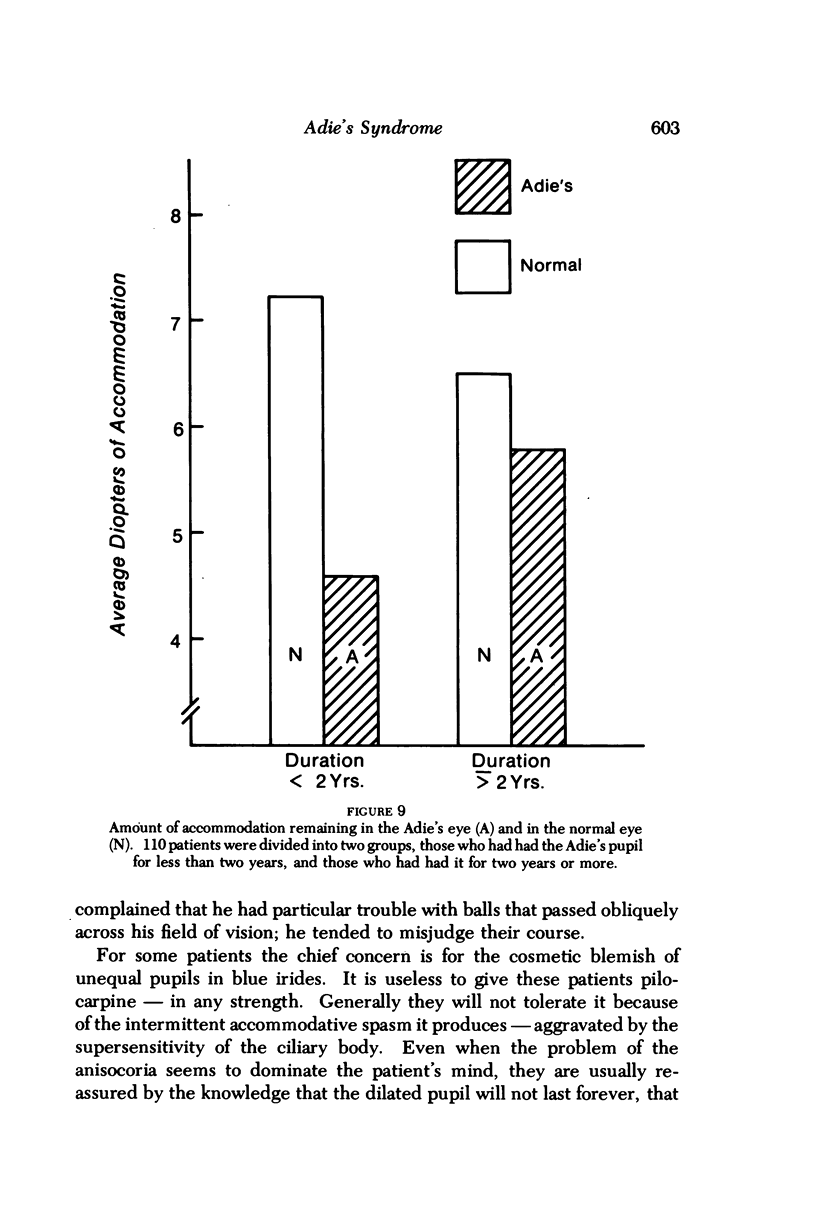
- Younge B. R., Buski Z. J. Tonic pupil: a simple screening test. Can J Ophthalmol. 1976 Oct;11(4):295–299. [PubMed] [Google Scholar]