

Abstract
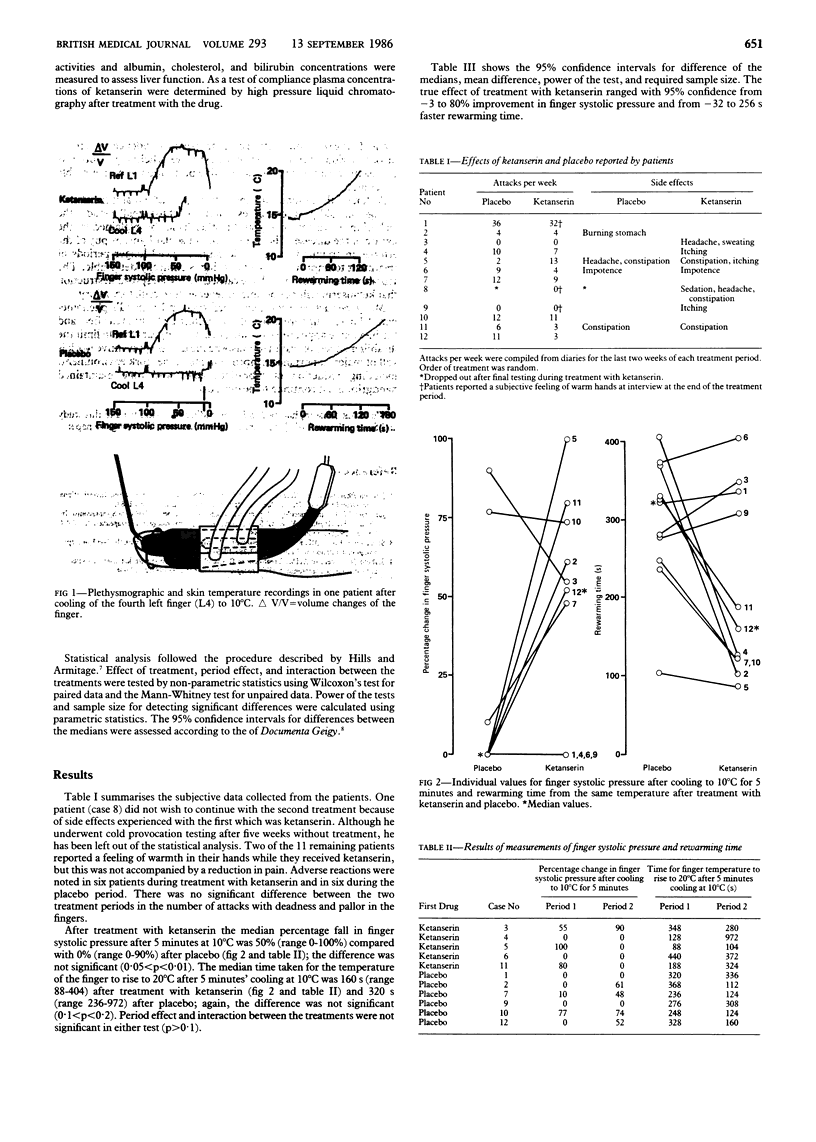
The specific serotonin receptor blocker ketanserin was given orally to 12 patients with traumatic vasospastic disease in a double blind crossover study. The effect of treatment was assessed by measuring finger systolic pressure and rewarming time after cold provocation and by medical interview and diaries. Median (range) percentage change in finger systolic pressure after cooling was 50 (0-100)% after treatment with ketanserin compared with 0 (0-90)% after placebo. Median (range) rewarming time after cooling decreased from 320 (236-972)s with placebo to 160 (88-404)s after treatment with ketanserin. These changes were not significant. Ninety five percent confidence intervals for difference between the treatments, however, showed that finger systolic pressure may be 80% better and rewarming time 256 seconds faster after treatment with ketanserin than after placebo. The number of attacks did not differ significantly between the two treatments. Two patients had a feeling of warmth in their hands during treatment with ketanserin. The results suggest that orally administered ketanserin may improve digital circulation in patients with traumatic vasospastic disease, but larger numbers of patients are required to assess the true effect of treatment with ketanserin in this disease.
Full text
PDF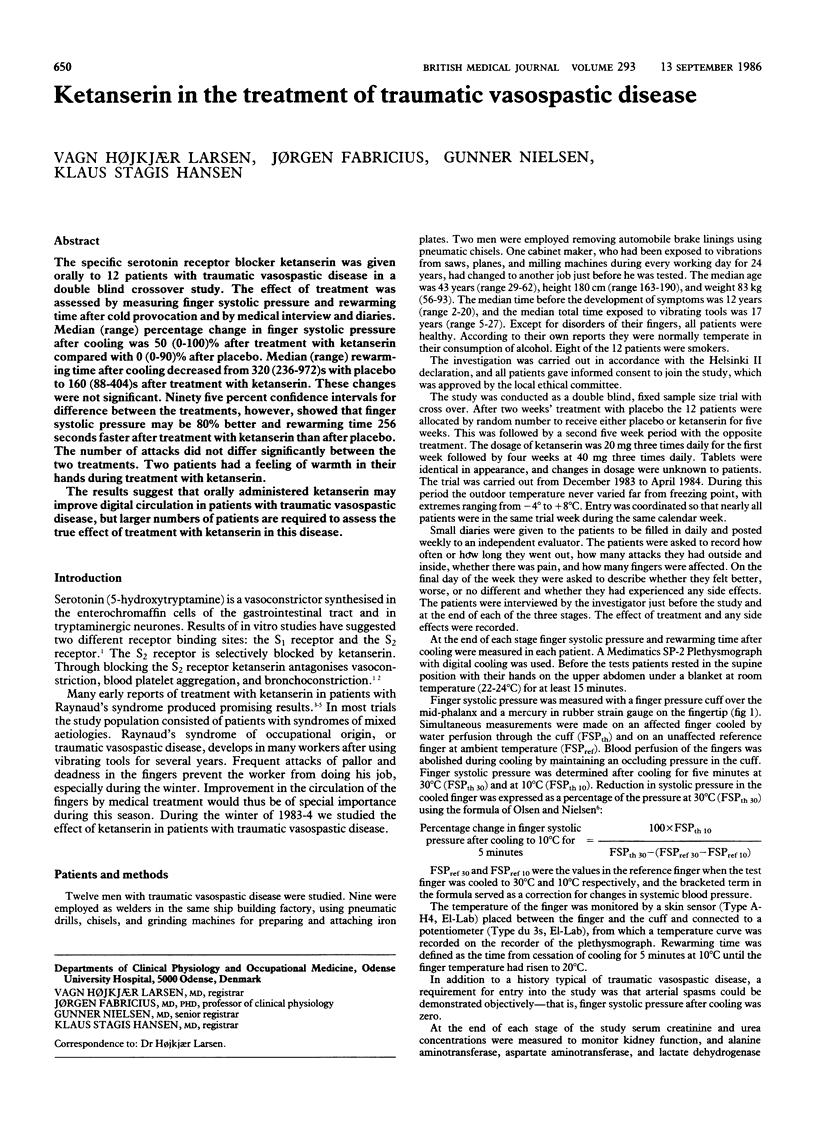

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Blunt R. J., Porter J. M. Raynaud syndrome. Semin Arthritis Rheum. 1981 May;10(4):282–308. doi: 10.1016/0049-0172(81)90006-8. [DOI] [PubMed] [Google Scholar]
- Feinstein A. R. Clinical biostatistics. XXXIV. The other side of 'statistical significance': alpha, beta, delta, and the calculation of sample size. Clin Pharmacol Ther. 1975 Oct;18(4):491–505. doi: 10.1002/cpt1975184491. [DOI] [PubMed] [Google Scholar]
- Freiman J. A., Chalmers T. C., Smith H., Jr, Kuebler R. R. The importance of beta, the type II error and sample size in the design and interpretation of the randomized control trial. Survey of 71 "negative" trials. N Engl J Med. 1978 Sep 28;299(13):690–694. doi: 10.1056/NEJM197809282991304. [DOI] [PubMed] [Google Scholar]
- Roald O. K., Seem E. Treatment of Raynaud's phenomenon with ketanserin in patients with connective tissue disorders. Br Med J (Clin Res Ed) 1984 Sep 8;289(6445):577–579. doi: 10.1136/bmj.289.6445.577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stranden E., Roald O. K., Krohg K. Treatment of Raynaud's phenomenon with the 5-HT2-receptor antagonist ketanserin. Br Med J (Clin Res Ed) 1982 Oct 16;285(6348):1069–1071. doi: 10.1136/bmj.285.6348.1069. [DOI] [PMC free article] [PubMed] [Google Scholar]