

Abstract
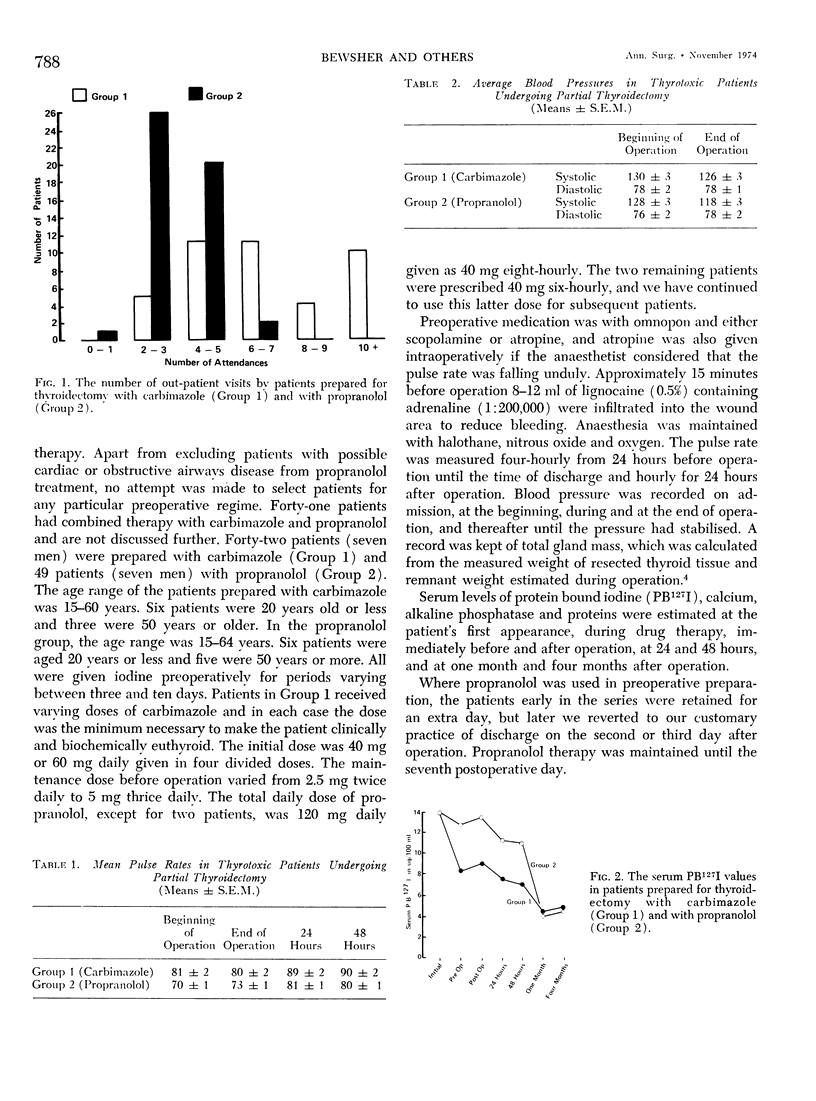
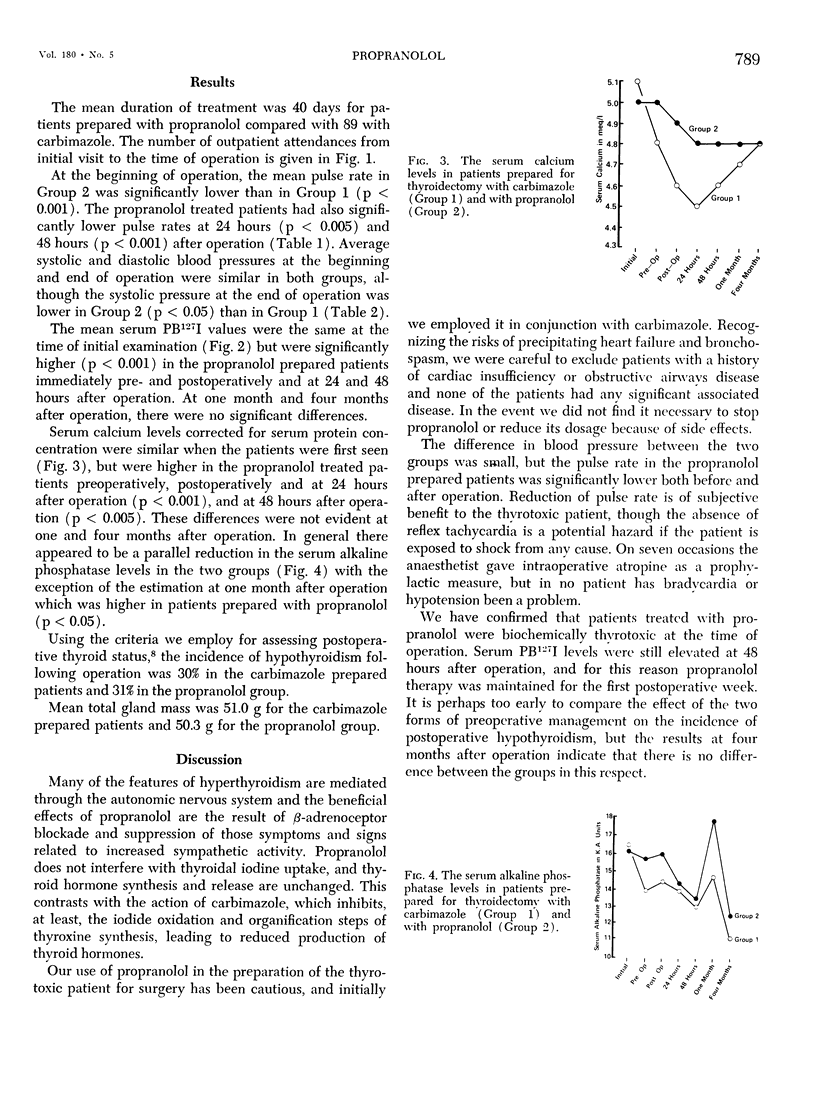
Forty-nine thyrotoxic patients prepared for partial thyroidectomy with the β-adrenoceptor blocking drug, propranolol, and iodine are compared with 42 patients prepared with carbimazole and iodine. The age and sex distribution of the two groups were comparable, but patients with obstructive airways disease and possible cardiac insufficiency were excluded from preparation with propranolol. The mean duration of preoperative treatment with propranolol was 40 days, compared with 89 days for carbimazole. Propranolol treated patients had lower pulse rates before and after operation. The serum PB127I values immediately before and after operation were higher in the propranolol group than in the carbimazole group, but were the same in both groups one and four months after operation. The incidence of hypothyroidism at one year after operation was 30% in the carbimazole prepared patients and 31% in the propranolol patients. Serum calcium levels were higher in the propranolol group at the time of operation. No adverse effects from the use of propranolol and at operation the thyroid gland prepared with propranolol was firmer, less friable, more easily mobilised and less likely to bleed than the gland prepared with carbimazole. There is, consequently, less risk of damage to the parathyroid glands and recurrent laryngeal nerves. However, the basal metabolic rate remains high on propranolol therapy and very careful supervision is advised.
Full text
PDF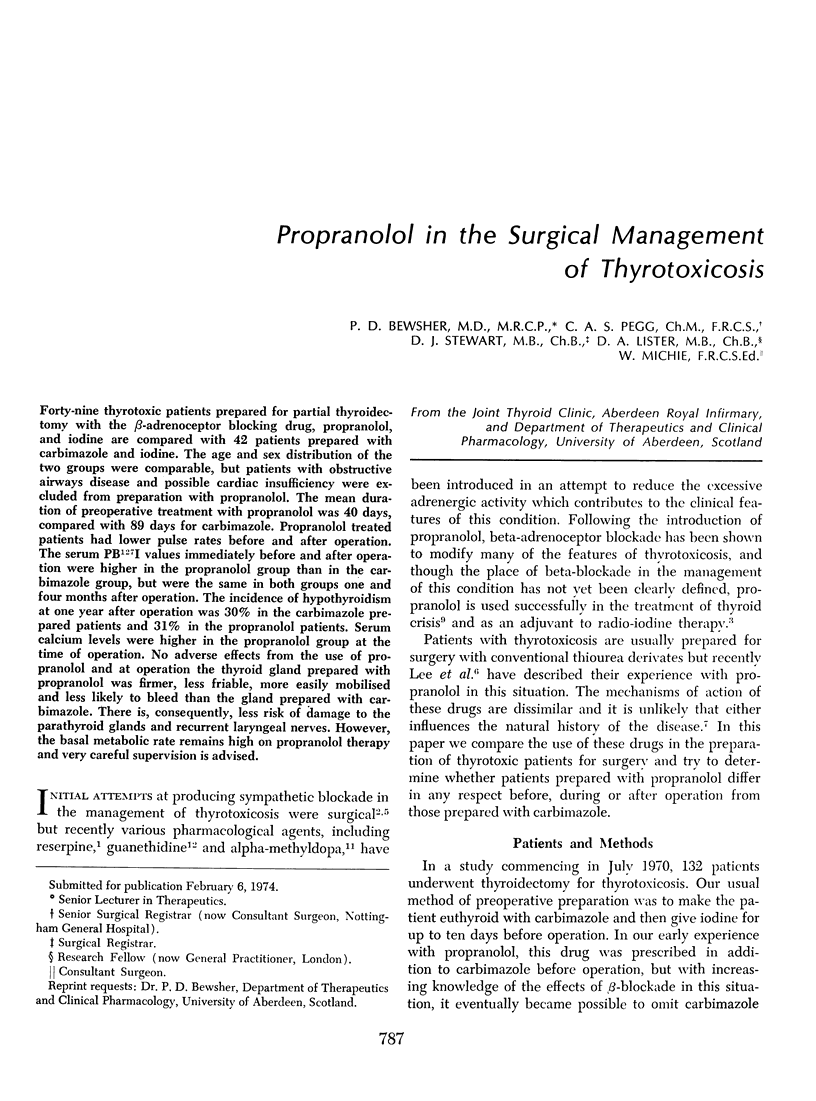

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BUCHANAN J., BUCHANAN W. W., CROOKS J., GALE G. E. The use of reserpine in the treatment of thyrotoxicosis. Scott Med J. 1959 Oct;4:486–490. doi: 10.1177/003693305900401004. [DOI] [PubMed] [Google Scholar]
- Hadden D. R., Montgomery D. A., Shanks R. G., Weaver J. A. Propranolol and iodine-131 in the management of thyrotoxicosis. Lancet. 1968 Oct 19;2(7573):852–854. doi: 10.1016/s0140-6736(68)91003-9. [DOI] [PubMed] [Google Scholar]
- Lee T. C., Coffey R. J., Mackin J., Cobb M., Routon J., Canary J. J. The use of propranolol in the surgical treatment of thyrotoxic patients. Ann Surg. 1973 Jun;177(6):643–647. [PMC free article] [PubMed] [Google Scholar]
- McLarty D. G., Brownlie B. E., Alexander W. D., Papapetrou P. D., Horton P. Remission of thyrotoxicosis during treatment with propranolol. Br Med J. 1973 May 12;2(5862):332–334. doi: 10.1136/bmj.2.5862.332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michie W., Pegg C. A., Bewsher P. D. Prediction of hypothyroidism after partial thyroidectomy for thyrotoxicosis. Br Med J. 1972 Jan 1;1(5791):13–17. doi: 10.1136/bmj.1.5791.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parsons V., Jewitt D. Beta-adrenergic blockade in the management of acute thyrotoxic crisis, tachycardia and arrhythmias. Postgrad Med J. 1967 Dec;43(506):756–762. doi: 10.1136/pgmj.43.506.756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seedat Y. K., Vinik A. I., Stewart-Wynne E. G. Propranolol and serum calcium in thyrotoxicosis. Br Med J. 1970 Aug 29;3(5721):525–526. doi: 10.1136/bmj.3.5721.525-d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- THEILEN E. O., WILSON W. R., TUTUNJI F. J. The acute hemodynamic effects of alpha-methyldopa in thyrotoxic patients and normal subjects. Metabolism. 1963 Jul;12:625–630. [PubMed] [Google Scholar]
- WALDSTEIN S. S., WEST G. H., Jr, LEE W. Y., BRONSKY D. GUANETHIDINE IN HYPERTHYROIDISM. JAMA. 1964 Aug 24;189:609–612. doi: 10.1001/jama.1964.03070080015003. [DOI] [PubMed] [Google Scholar]