

Abstract
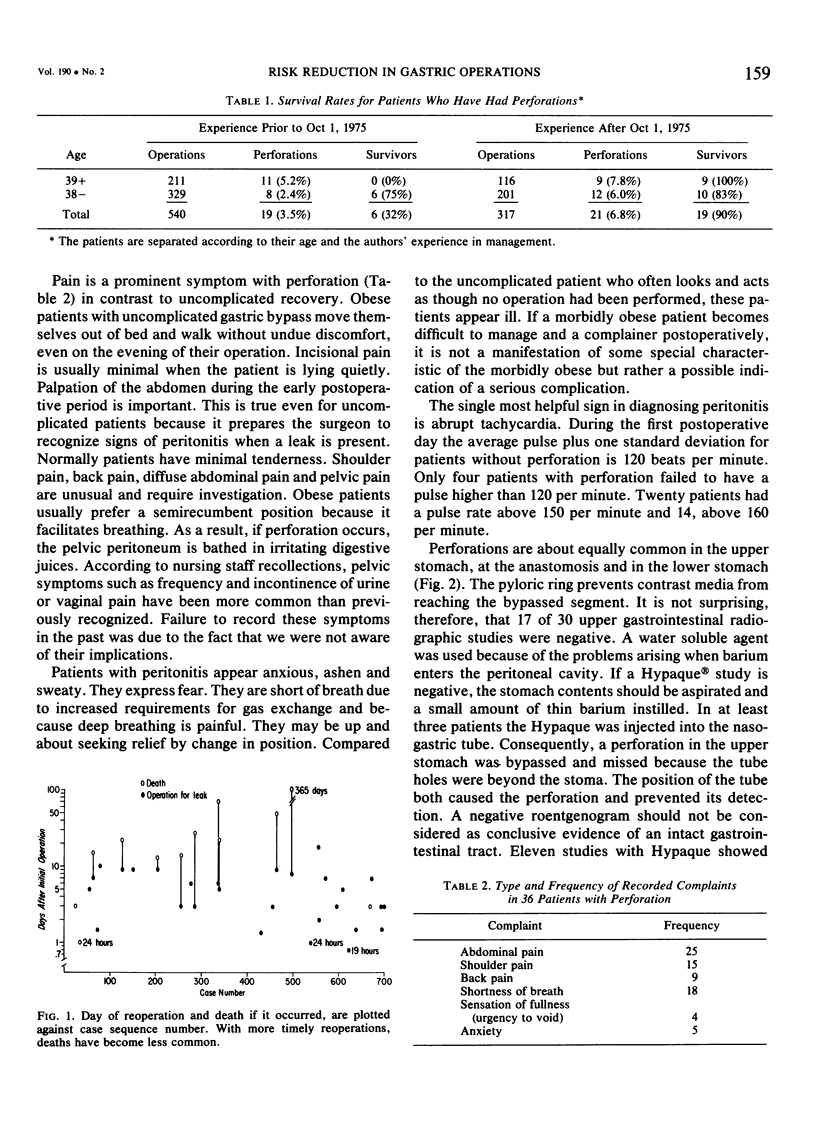
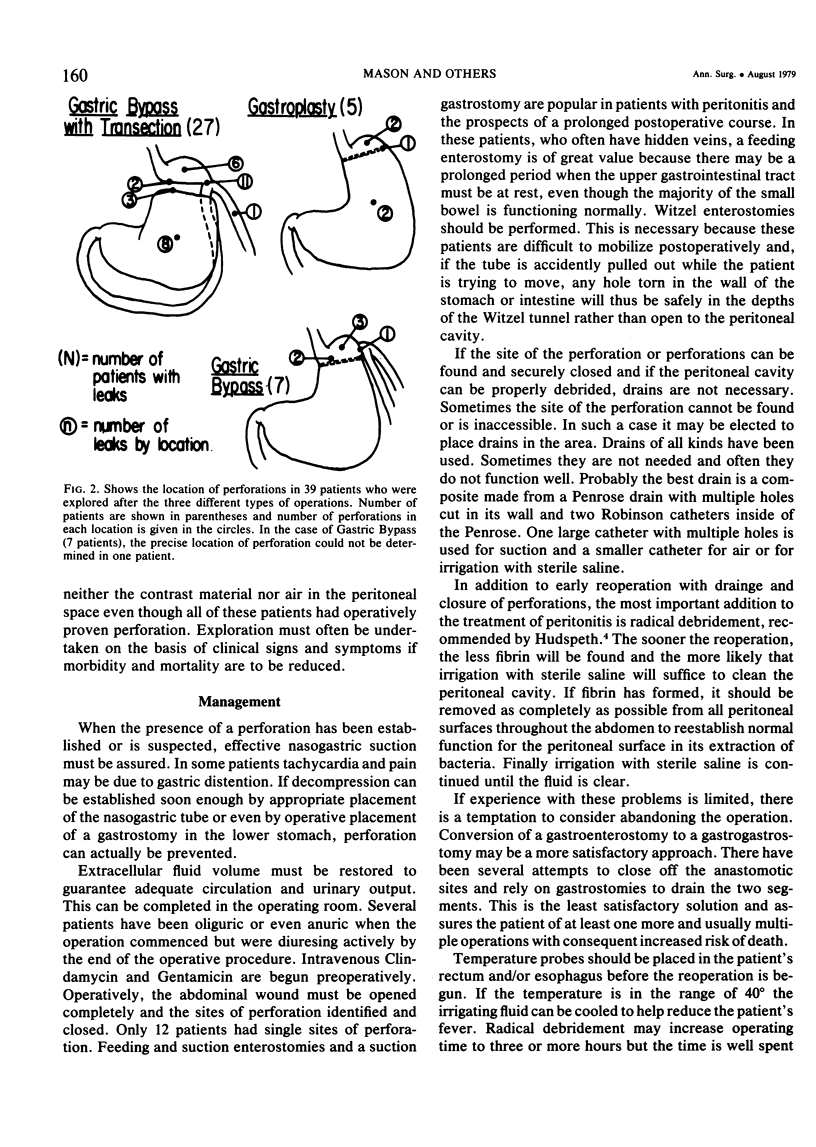
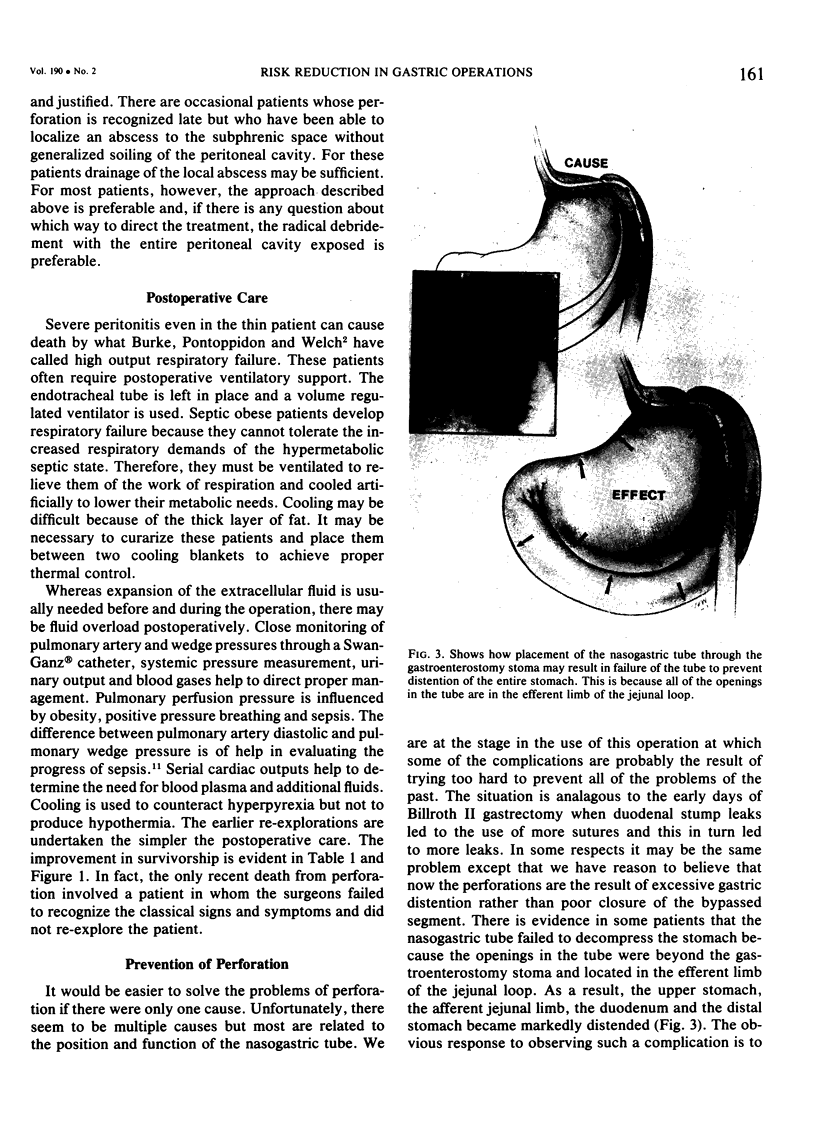
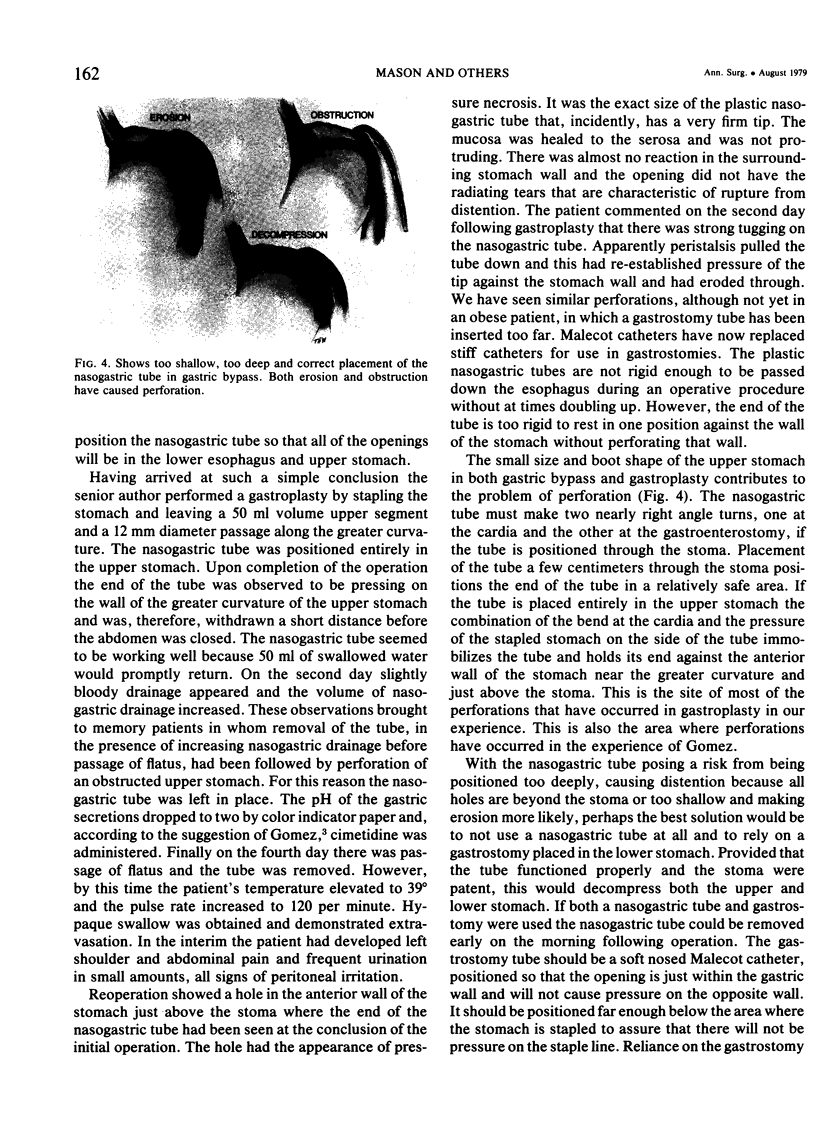
Although nearly devoid of late complications, gastric operations for obesity have resulted in 4.7% early postoperative perforations. For patients over 39 years of age who perforated, the first 11 patients died and the last 9 survived. Perforations are equally common in upper stomach, anastomosis, and lower stomach. They have become more frequent with the 50 ml upper stomach volume and 12 mm stoma that are required to assure optimum weight control. Perforation is as common with gastroplasty as with gastric bypass. If it occurs, it is normally within the first ten postoperative days. Acute dilatation and rupture of the stomach can happen if all the nasogastric tube holes are in the jejunum after gastric bypass. Erosion of the stomach by the hard end of the nasogastric tube has occurred when the tube was positioned in the upper stomach. This paper is dedicated to the prevention of death by early recognition and aggressive management of perforation and by prevention of perforations through careful attention to the details of these operations and early postoperative care.
Full text
PDF

Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Alder R. L., Terry B. E. Measurement and standardization of the gastric pouch in gastric bypass. Surg Gynecol Obstet. 1977 May;144(5):762–763. [PubMed] [Google Scholar]
- Hudspeth A. S. Radical surgical debridement in the treatment of advanced generalized bacterial peritonitis. Arch Surg. 1975 Oct;110(10):1233–1236. doi: 10.1001/archsurg.1975.01360160071012. [DOI] [PubMed] [Google Scholar]
- Maini B. S., Blackburn G. L., McDermott W. V., Jr Technical considerations in a gastric bypass operation for morbid obesity. Surg Gynecol Obstet. 1977 Dec;145(6):907–908. [PubMed] [Google Scholar]
- Mason E. E., Printen K. J., Blommers T. J., Scott D. H. Gastric bypass for obesity after ten years experience. Int J Obes. 1978;2(2):197–206. [PubMed] [Google Scholar]
- Mason E. E., Printen K. J., Hartford C. E., Boyd W. C. Optimizing results of gastric bypass. Ann Surg. 1975 Oct;182(4):405–414. doi: 10.1097/00000658-197510000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Printen K. J., Mason E. E. Gastric surgery for relief of morbid obesity. Arch Surg. 1973 Apr;106(4):428–431. doi: 10.1001/archsurg.1973.01350160046007. [DOI] [PubMed] [Google Scholar]
- Sibbald W. J., Paterson N. A., Holliday R. L., Anderson R. A., Lobb T. R., Duff J. H. Pulmonary hypertension in sepsis: measurement by the pulmonary arterial diastolic-pulmonary wedge pressure gradient and the influence of passive and active factors. Chest. 1978 May;73(5):583–591. doi: 10.1378/chest.73.5.583. [DOI] [PubMed] [Google Scholar]