

Abstract
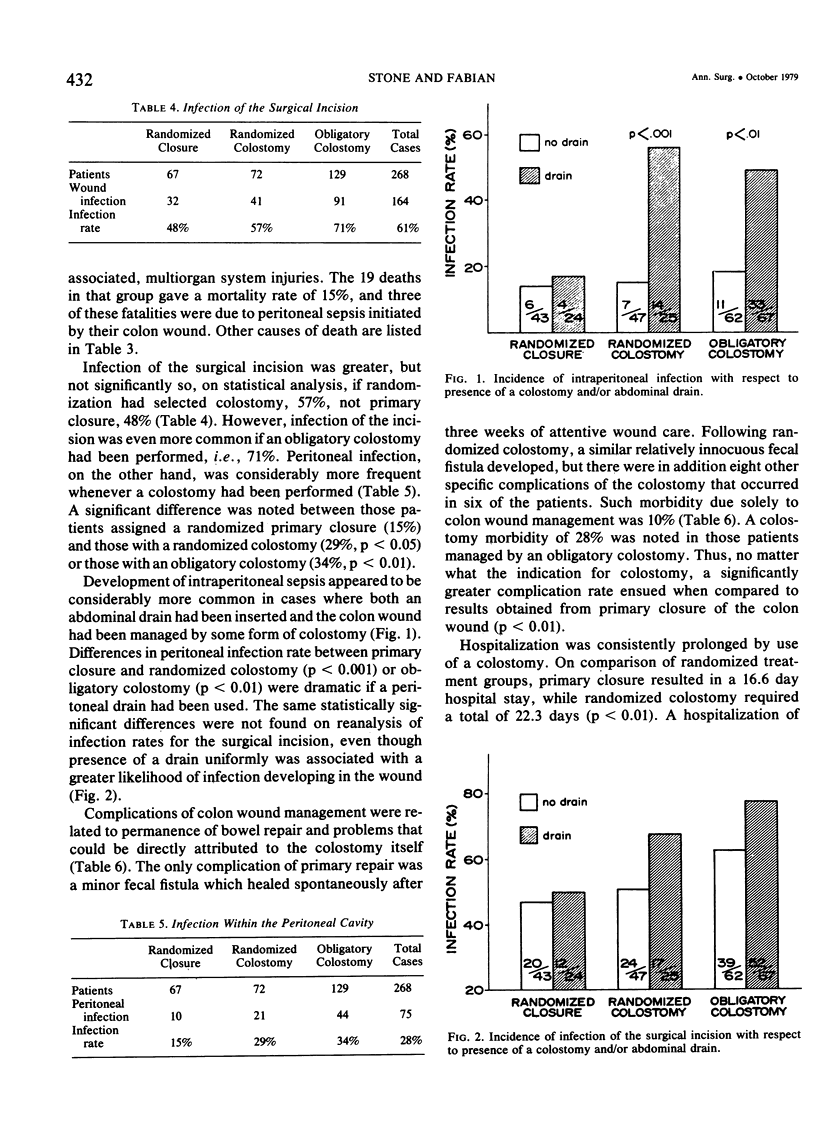
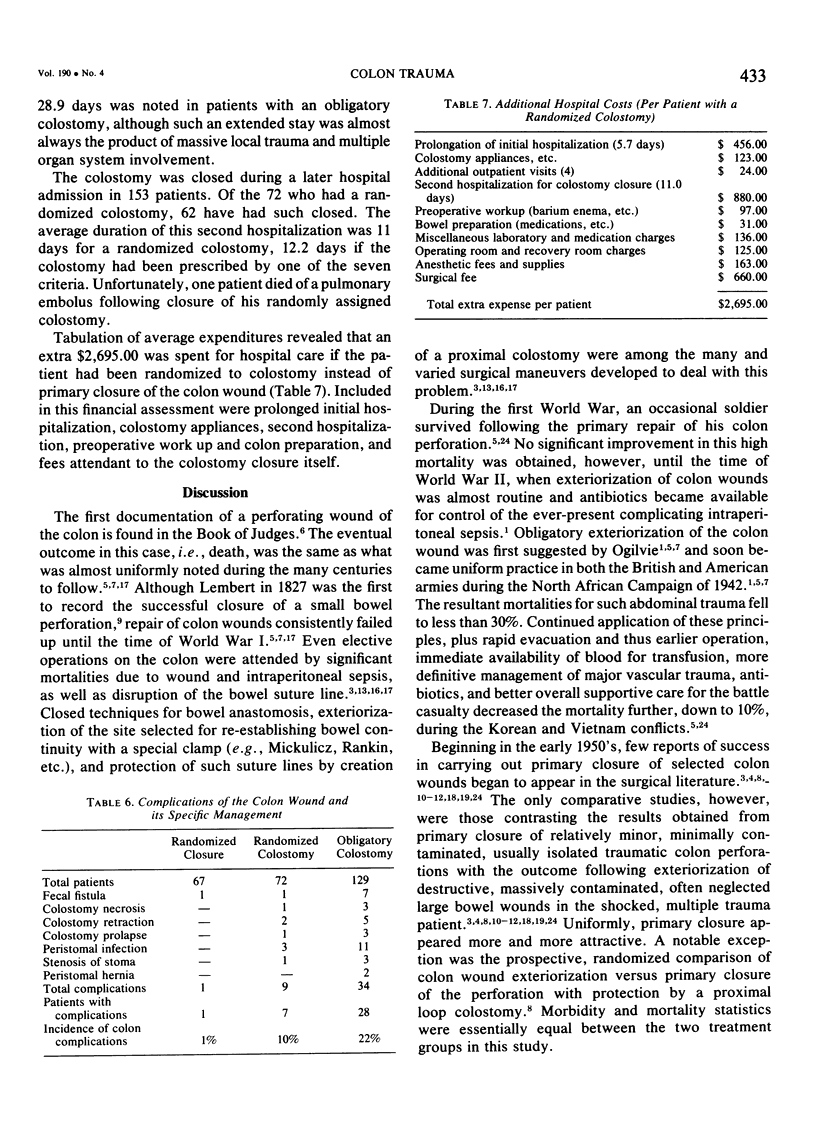
During a 44 month trial, 268 patients with wounds of the colon were entered into a prospective, randomized, nonblinded study. Consideration for primary closure demanded that: preoperative shock was never profound, blood loss was less than 20% of estimated normal volume, no more than two intra-abdominal organ systems had been injured, fecal contamination was minimal, operation was begun within eight hours, and wounds of colon and abdominal wall were never so destructive as to require resection. Once such criteria had been satisfied, colon wound management was dictated by last digit in the randomly assigned hospital number; odd indicated primary closure; even, exteriorization of the wound or primary closure with protection by a proximal vent. Results obtained in 139 determinant patients eligible for randomization revealed that primary closure (67 patients) had a lower infection rate of the incision (48% vs S7%, p > 0.05) and a still lower infection rate for the abdomen proper (15% vs 29%, p < 0.05) on comparison to the 72 patients with a randomized colostomy. Morbidity otherwise for the randomized colostomy was tenfold greater than if a primary closure had been performed. Average postoperative stay was six days longer (p < 0.01) if a colostomy had been created, exclusive of subsequent hospitalization for colostomy closure; while the total extra cost for management of the colon wound by colostomy was approximately $2,700.00. Although immediate mortalities were identical, one late death occurred following colostomy closure. These data not only confirm the safety of primary closure for colon wounds in selected cases, but also indicate that such should become the preferred method of treatment whenever specific criteria have been met.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Freeark R. J. The injured colon. J Trauma. 1977 Jul;17(7):563–564. [PubMed] [Google Scholar]
- Haygood F. D., Polk H. C., Jr Gunshot wounds of the colon. A review of 100 consecutive patients, with emphasis on complications and their causes. Am J Surg. 1976 Feb;131(2):213–218. doi: 10.1016/0002-9610(76)90100-8. [DOI] [PubMed] [Google Scholar]
- Haynes C. D., Gunn C. H., Martin J. D., Jr Colon injuries. Arch Surg. 1968 Jun;96(6):944–948. doi: 10.1001/archsurg.1968.01330240090021. [DOI] [PubMed] [Google Scholar]
- Kirkpatrick J. R., Rajpal S. G. The injured colon: therapeutic considerations. Am J Surg. 1975 Feb;129(2):187–191. doi: 10.1016/0002-9610(75)90296-2. [DOI] [PubMed] [Google Scholar]
- LoCicero J., 3rd, Tajima T., Drapanas T. A half-century of experience in the management of colon injuries: changing concepts. J Trauma. 1975 Jul;15(7):575–579. doi: 10.1097/00005373-197507000-00003. [DOI] [PubMed] [Google Scholar]
- Matolo N. M., Cohen S. E., Wolfman E. F., Jr Experimental evaluation of primary repair of colonic injuries. Arch Surg. 1976 Jan;111(1):78–80. doi: 10.1001/archsurg.1976.01360190080015. [DOI] [PubMed] [Google Scholar]
- Matolog N. M., Wolfman E. F. Primary repair of colonic injuries: a clinical evaluation. J Trauma. 1977 Jul;17(7):554–556. doi: 10.1097/00005373-197707000-00012. [DOI] [PubMed] [Google Scholar]
- Mulherin J. L., Jr, Sawyers J. L. Evaluation of three methods for managing penetrating colon injuries. J Trauma. 1975 Jul;15(7):580–587. doi: 10.1097/00005373-197507000-00004. [DOI] [PubMed] [Google Scholar]
- Nahai F., Lamb J. M., Havican R. G., Stone H. H. Factors involved in disruption of intestinal anastomoses. Am Surg. 1977 Jan;43(1):45–51. [PubMed] [Google Scholar]
- Robbs J. V. The alternative to colostomy for the injured colon. S Afr Med J. 1978 Jan 21;53(3):95–97. [PubMed] [Google Scholar]
- Steele M., Blaisdell F. W. Treatment of colon injuries. J Trauma. 1977 Jul;17(7):557–562. doi: 10.1097/00005373-197707000-00013. [DOI] [PubMed] [Google Scholar]
- Stone H. H., Hester T. R., Jr Incisional and peritoneal infection after emergency celiotomy. Ann Surg. 1973 Jun;177(6):669–678. doi: 10.1097/00000658-197306000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stone H. H., Kolb L. D., Geheber C. E. Incidence and significance of intraperitoneal anaerobic bacteria. Ann Surg. 1975 May;181(5):705–715. doi: 10.1097/00000658-197505000-00027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Voyles C. R., Flint L. M., Jr Wound management after trauma to the colon. South Med J. 1977 Sep;70(9):1067–1069. doi: 10.1097/00007611-197709000-00017. [DOI] [PubMed] [Google Scholar]
- Yajko R. D., Norton L. W., Bloemendal L., Eiseman B. Morbidity of colostomy closure. Am J Surg. 1976 Sep;132(3):304–306. doi: 10.1016/0002-9610(76)90380-9. [DOI] [PubMed] [Google Scholar]
- Yaw P. B., Smith R. N., Glover J. L. Eight years experience with civilian injuries of the colon. Surg Gynecol Obstet. 1977 Aug;145(2):203–205. [PubMed] [Google Scholar]