

Abstract
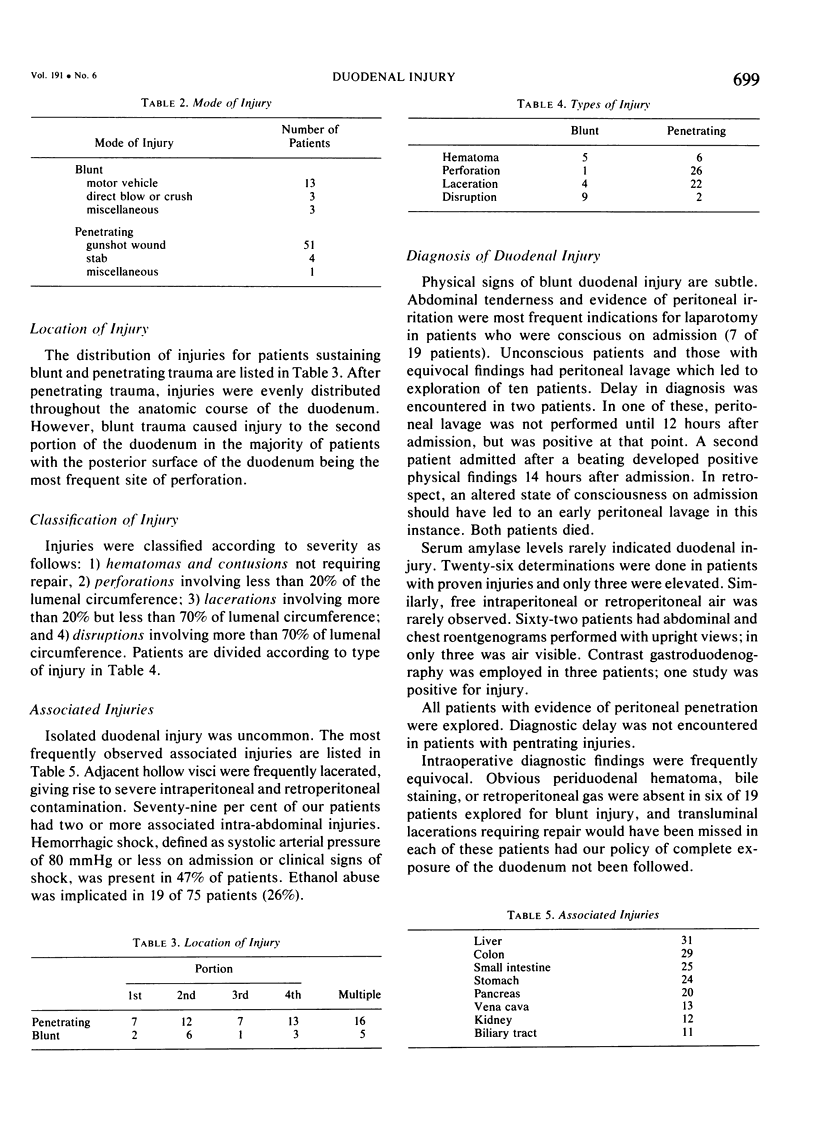
Seventy-five consecutive patients who sustained injuries to the duodenum were admitted to our hospital over a nine-year period. Nineteen blunt injuries and 56 penetrating injuries were encountered. Blunt injuries were usually the result of motor vehicle accidents and steering wheel impact was frequently implicated. Penetrating injuries most commonly followed gunshot wounds, particularly those where the bullet tract travelled transversely across the peritoneal cavity. Seventy-nine per cent of the patients had two or more associated intra-abdominal organ injuries with other intestinal injuries, biliary tract injuries, and pancreatic injuries predominating. Forty-seven per cent of the patients were admitted in shock. Following blunt injury, diagnostic delay was encountered in two patients. Adjuncts to diagnosis such as abdominal roentgenograms, serum amylase levels, and contrast gastroduodenography, were not helpful. Peritoneal lavage, however, was valuable in patients with equivocal physical findings. Intraoperative diagnosis was also challenging. Complete mobilization of the structures surrounding the duodenum to provide exposure of the entire duodenum was necessary. Six injuries that initially appeared trivial would have been missed had this procedure not been followed. Suture closure was the most common reparative technique used. Tube decompression of the duodenum was a valuable addition. No suture line dehiscences were encountered in ten patients so treated. Overall mortality in patients surviving more than 24 hours was 12%.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ahmad W., Polk H. C., Jr Blunt abdominal trauma: a prospective study with selective peritoneal lavage. Arch Surg. 1976 Apr;111(4):489–492. doi: 10.1001/archsurg.1976.01360220185032. [DOI] [PubMed] [Google Scholar]
- CATTELL R. B., BRAASCH J. W. A technique for the exposure of the third and fourth portions of the duodenum. Surg Gynecol Obstet. 1960 Sep;111:378–379. [PubMed] [Google Scholar]
- COCKE W. M., Jr, MEYER K. K. RETROPERITONEAL DUODENAL RUPTURE. PROPOSED MECHANISM, REVIEW OF LITERATURE AND REPORT OF A CASE. Am J Surg. 1964 Dec;108:834–839. doi: 10.1016/0002-9610(64)90043-1. [DOI] [PubMed] [Google Scholar]
- Corley R. D., Norcross W. J., Shoemaker W. C. Traumatic injuries to the duodenum: a report of 98 patients. Ann Surg. 1975 Jan;181(1):92–98. doi: 10.1097/00000658-197501000-00020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeMars J. J., Bubrick M. P., Hitchcock C. R. Duodenal perforation in blunt abdominal trauma. Surgery. 1979 Oct;86(4):632–638. [PubMed] [Google Scholar]
- Kelly G., Norton L., Moore G., Eiseman B. The continuing challenge of duodenal injuries. J Trauma. 1978 Mar;18(3):160–165. [PubMed] [Google Scholar]
- Miller R. T. RETROPERITONEAL RUPTURE OF THE DUODENUM BY BLUNT FORCE. Ann Surg. 1916 Nov;64(5):550–578. doi: 10.1097/00000658-191611000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stone H. H., Fabian T. C. Management of duodenal wounds. J Trauma. 1979 May;19(5):334–339. doi: 10.1097/00005373-197905000-00006. [DOI] [PubMed] [Google Scholar]
- Talbot W. A., Shuck J. M. Retroperitoneal duodenal injury due to blunt abdominal trauma. Am J Surg. 1975 Dec;130(6):659–666. doi: 10.1016/0002-9610(75)90416-x. [DOI] [PubMed] [Google Scholar]