

Abstract
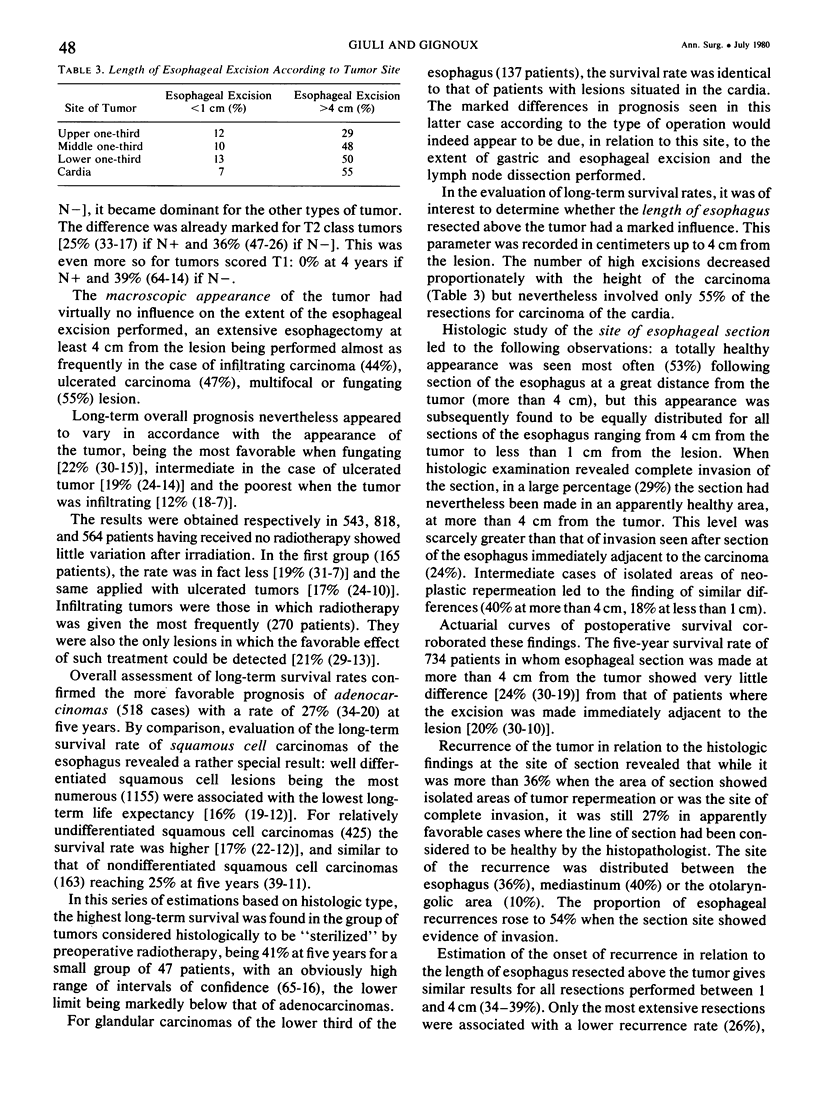
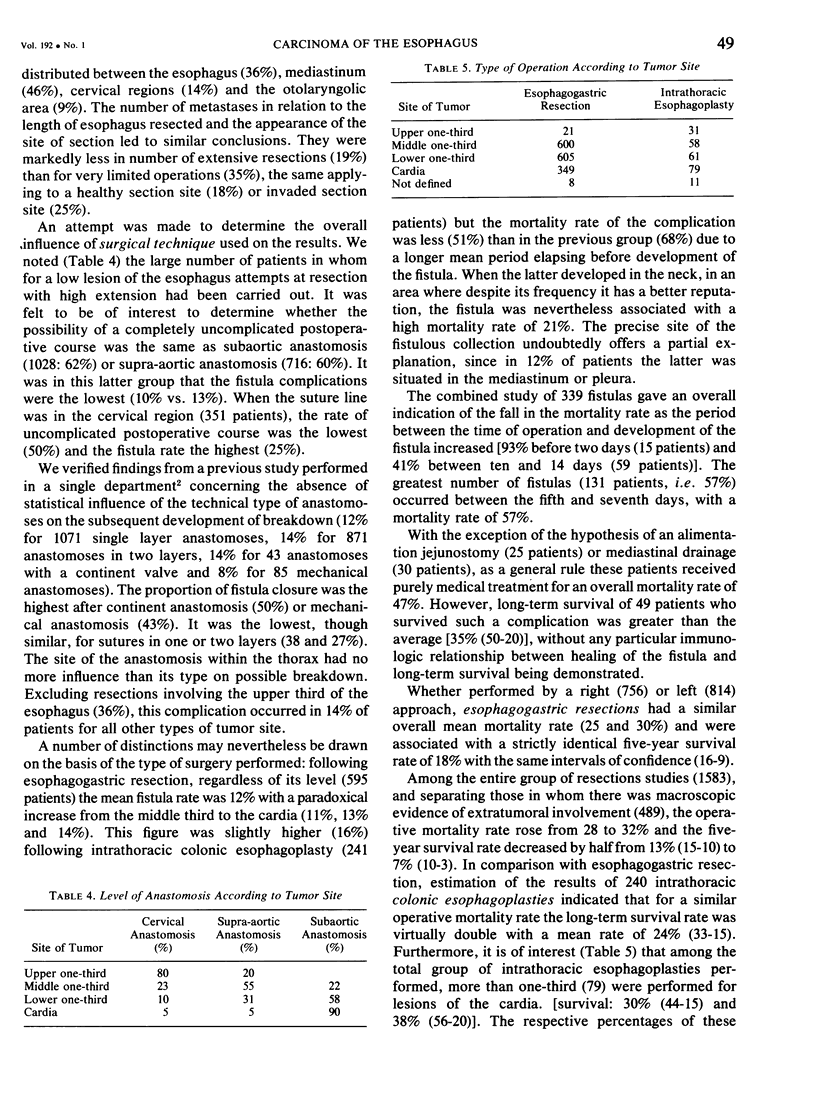
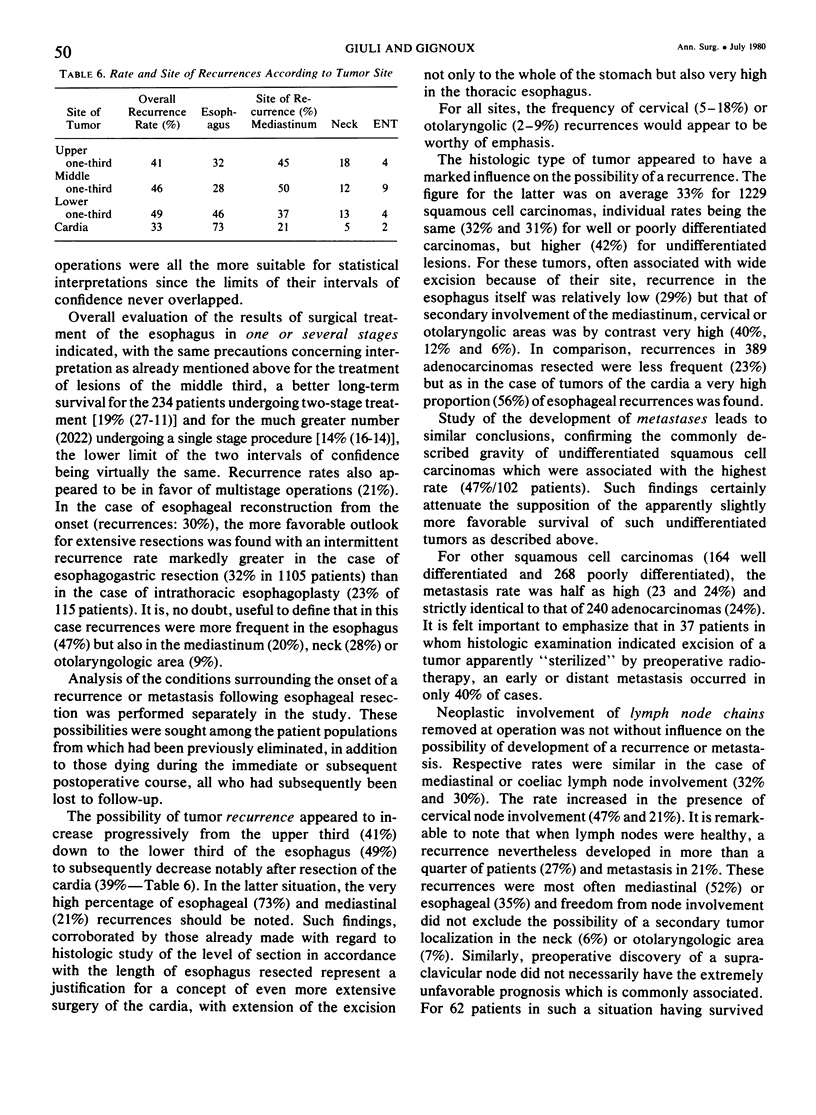
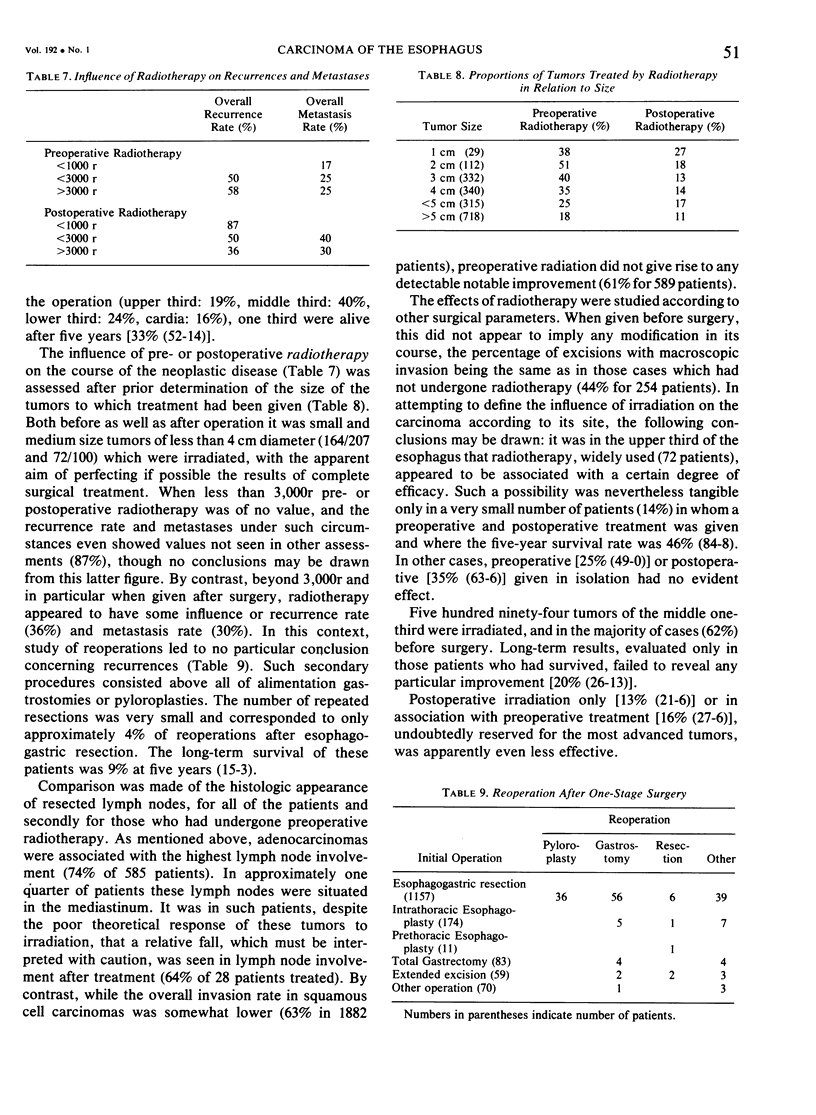
A multicenter retrospective statistical study of 2,400 patients with tumors of the esophagus and cardia was undertaken. Study of individual sites revealed the operability of certain carcinomas of the upper third of the esophagus with a reasonable five-year survival rate despite macroscopic invasion seen in more than half the patients. For the middle third of the esophagus, intrathoracic colonic esophagoplasty with esophageal resection extending as high as possible appeared to offer the best long-term results, particularly if the anastomosis was performed in the neck. Tumors of the lower third of the esophagus were also associated with better results when the esophageal anastomosis was made at a level above the aortic arch, resulting in an improved survival rate for patients undergoing intrathoracic colonic esophagoplasties. For carcinomas of the cardia, use of total gastrectomy was superior to the use of upper polar gastrectomy, but the results were better when gastric excision was also associated with esophageal excision. The finding of normal lymph nodes did not preclude recurrence of the tumor in approximately one-fourth of the patients. Esophageal sections at a distance from the tumor was not necessarily synonymous with section in a healthy area, since the sites of sections studied were either invaded (29%) or areas of neoplastic repermeation (40%). Existence of a histologically normal esophageal section site did not preclude recurrences in 27% of patients with more than one-third in the esophagus. Undifferentiated or poorly differentiated squamous cell carcinomas paradoxically appeared to have a somewhat better long-term prognosis than well differentiated forms, but the increased number of metastases associated with them confirms their unfavorable prognosis. The importance of the T/N classification was confirmed for tumors in classes T1 and T2. From Stage T3, the N criterion was not important. Incidence of postoperative mortality from fistulas appeared to decrease progressively, chiefly due to appropriate medical treatment. Cervical fistulas were associated with a mortality rate of 21%. After esophageal anastomosis above the aortic arch was performed, more than 10% of the recurrences were seen in the neck, indicating the need for extension of the incision as high as possible. Metastases to the bone were present in 15% of the patients. Preoperative radiotherapy did not lessen the number of lymph nodes found to be invaded at the time of excision; the tumors considered to be histologically “sterilized” by irradiation were nevertheless associated with a high incidence of lymph node involvement (approximately one-third) and with more than a 40% rate of distant metastases. Excisions considered to be “palliative” by the surgeon nevertheless were of definite value. The mean survival rate at five years was 12%, and one-third of these patients showed no recurrence of neoplasm.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Giuli R., Estenne B., Clot P., Faure J. C., Hay J. M., Richard C. A., Lortat-Jacob J. L. Résultats éloignés de 482 interventions d'exérèse pour cancer gastrique. Valeur de la gastrectomie totale élargie. Ann Chir. 1972 Dec;26(25):1283–1296. [PubMed] [Google Scholar]
- Giuli R., Estenne B., Faure J. C., Clot P., Richard C. A., Lortat-Jacob J. L. La désunion des anastomoses oesophago-gastriques dans la chirurgie du cancer de l'osesophage. Bilan de 415 interventions. Ann Chir. 1973 Jun;27(6):567–577. [PubMed] [Google Scholar]