

Abstract
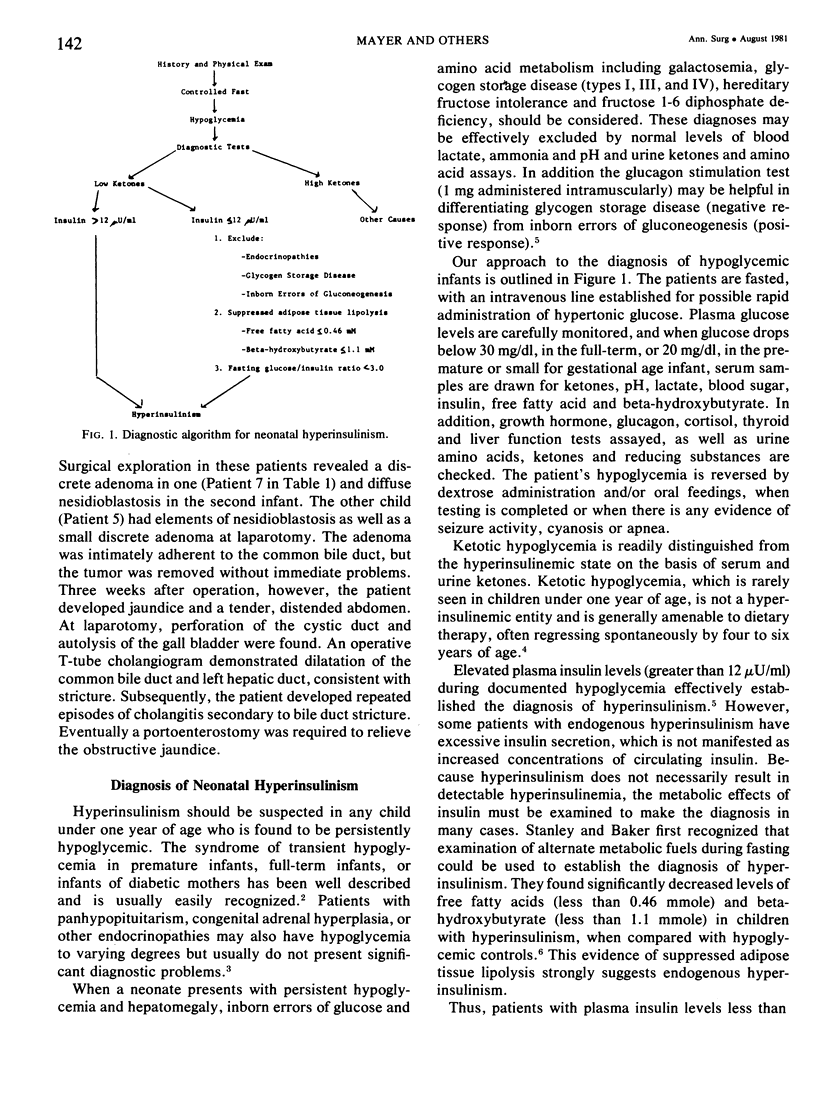
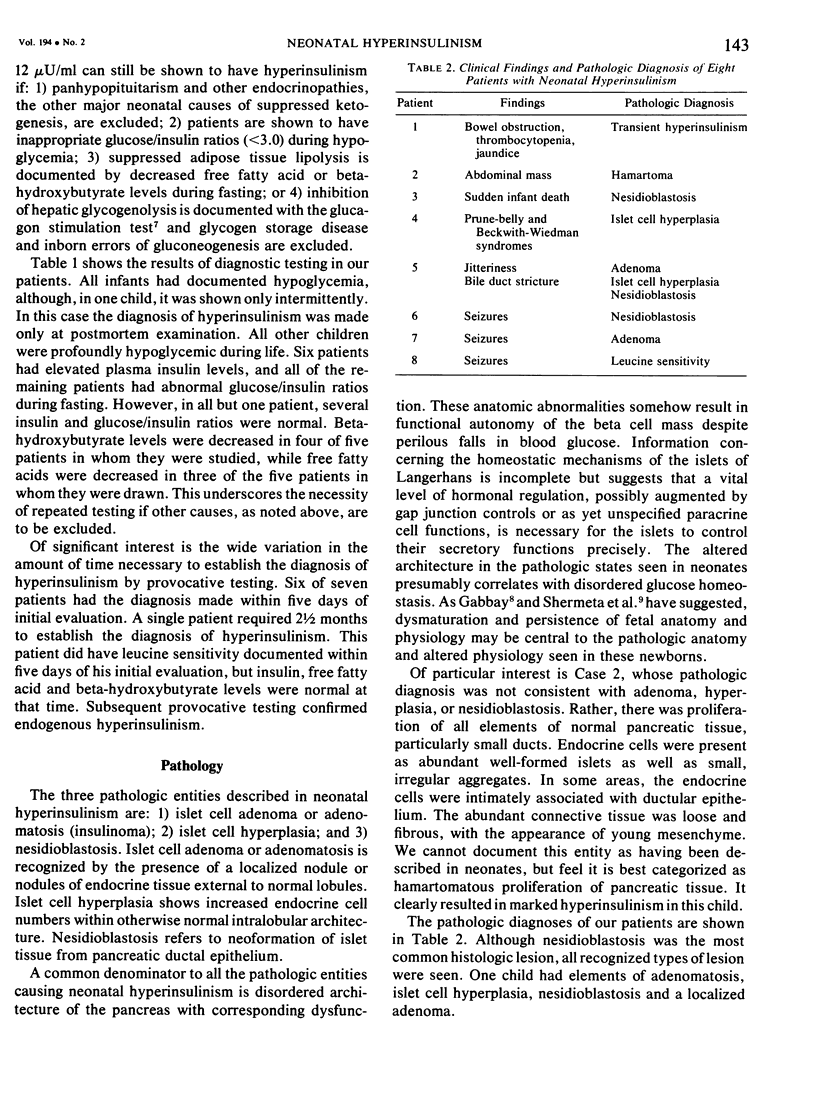
Endogenous hyperinsulinism is the leading cause of persistent hypoglycemia in children under one year of age. Classically, the symptoms of neonatal hypoglycemia have been referable to central nervous system dysfunction, with seizures described in nearly all patients. Our experience with eight neonates emphasizes the protean manifestations of this disease. One patient presented with a maternal history of diuretic use, and developed asymptomatic hyperinsulinism documented by provocative testing. The hyperinsulinism cleared after two weeks of medical therapy. This transient hyperinsulinism may have been secondary to use of a thiazide-type diuretic. A second patient presented, as a neonate, with a large abdominal mass but no seizure activity. Exploratory laparotomy revealed an 11 x 5 x 3 cm pancreatic tumor, which required splenectomy, 60% gastrectomy and duodenectomy for removal. Histologic examination demonstrated an insulin-secreting hamartoma. A third patient died suddenly without prior symptoms, and was found to have striking nesidioblastosis on pathologic examination. One infant presented with absence of the abdominal musculature (prune belly syndrome) and features of the Beck-with-Wiedeman syndrome, as well as profound hypoglycemia. Only three patients had seizures, and an additional patient had jitteriness. Pathologic diagnoses were: nesidioblastosis (n = 2); islet cell hyperplasia (n = 1); adenoma (n = 1); hamartoma (n = 1); transient hyperinsulinism (n = 1). One patient's pancreas showed areas of nesidioblastosis, islet cell hyperplasia, and a discrete adenoma in the region of the common bile duct. Careful diagnostic testing is essential in these patients, inasmuch as hypoglycemia is poorly tolerated by neonates and infants. Using the diagnostic algorithm presented here, all patients' endogenous hyperinsulinism was documented quickly and efficiently. Recognition of the broad spectrum of symptoms with which these patients may present is essential if serious neurologic sequelae are to be avoided.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Becker K., Wendel U., Przyrembel H., Tsotsalas M., Münterfering H., Bremer H. J. Beta cell nesidioblastosis. Eur J Pediatr. 1978 Jan 17;127(2):75–89. doi: 10.1007/BF00445763. [DOI] [PubMed] [Google Scholar]
- CORNBLATH M., ODELL G. B., LEVIN E. Y. Symptomatic neonatal hypoglycemia associated with toxemia of pregnancy. J Pediatr. 1959 Nov;55:545–562. doi: 10.1016/s0022-3476(59)80239-0. [DOI] [PubMed] [Google Scholar]
- Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 30-1978. N Engl J Med. 1978 Aug 3;299(5):241–248. doi: 10.1056/NEJM197808032990509. [DOI] [PubMed] [Google Scholar]
- GOLDNER M. G., ZAROWITZ H., AKGUN S. Hyperglycemia and glycosuria due to thiazide derivatives administered in diabetes mellitus. N Engl J Med. 1960 Feb 25;262:403–405. doi: 10.1056/NEJM196002252620807. [DOI] [PubMed] [Google Scholar]
- Gauderer M., Stanley C. A., Baker L., Bishop H. C. Pancreatic adenomas in infants and children: current surgical management. J Pediatr Surg. 1978 Dec;13(6D):591–596. doi: 10.1016/s0022-3468(78)80099-2. [DOI] [PubMed] [Google Scholar]
- Obenshain S. S., Adam P. A., King K. C., Teramo K., Raivio K. O., Räihä N., Schwartz R. Human fetal insulin response to sustained maternal hyperglycemia. N Engl J Med. 1970 Sep 10;283(11):566–570. doi: 10.1056/NEJM197009102831104. [DOI] [PubMed] [Google Scholar]
- Pagliara A. S., Karl I. E., Haymond M., Kipnis D. M. Hypoglycemia in infancy and childhood. II. J Pediatr. 1973 Apr;82(4):558–577. doi: 10.1016/s0022-3476(73)80581-5. [DOI] [PubMed] [Google Scholar]
- Rich R. H., Dehner L. P., Okinaga K., Deeb L. C., Ulstrom R. A., Leonard A. S. Surgical management of islet-cell adenoma in infancy. Surgery. 1978 Oct;84(4):519–526. [PubMed] [Google Scholar]
- Schwartz S. S., Rich B. H., Lucky A. W., Straus F. H., 2nd, Gonen B., Wolfsdorf J., Thorp F. W., Burrington J. D., Madden J. D., Rubenstein A. H. Familial nesidioblastosis: severe neonatal hypoglycemia in two families. J Pediatr. 1979 Jul;95(1):44–53. doi: 10.1016/s0022-3476(79)80080-3. [DOI] [PubMed] [Google Scholar]
- Shermeta D. W., Mendelsohn G., Haller J. A., Jr Hyperinsulinemic hypoglycemia of the neonate associated with persistent fetal histology and function of the pancreas. Ann Surg. 1980 Feb;191(2):182–186. doi: 10.1097/00000658-198002000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanley C. A., Baker L. Hyperinsulinism in infancy: diagnosis by demonstration of abnormal response to fasting hypoglycemia. Pediatrics. 1976 May;57(5):702–711. [PubMed] [Google Scholar]
- Stanley C. A., Baker L. Hyperinsulinism in infants and children: diagnosis and therapy. Adv Pediatr. 1976;23:315–355. [PubMed] [Google Scholar]
- Woo D., Scopes J. W., Polak J. M. Idiopathic hypoglycaemia in sibs with morphological evidence of nesidioblastosis of the pancreas. Arch Dis Child. 1976 Jul;51(7):528–531. doi: 10.1136/adc.51.7.528. [DOI] [PMC free article] [PubMed] [Google Scholar]