

Abstract
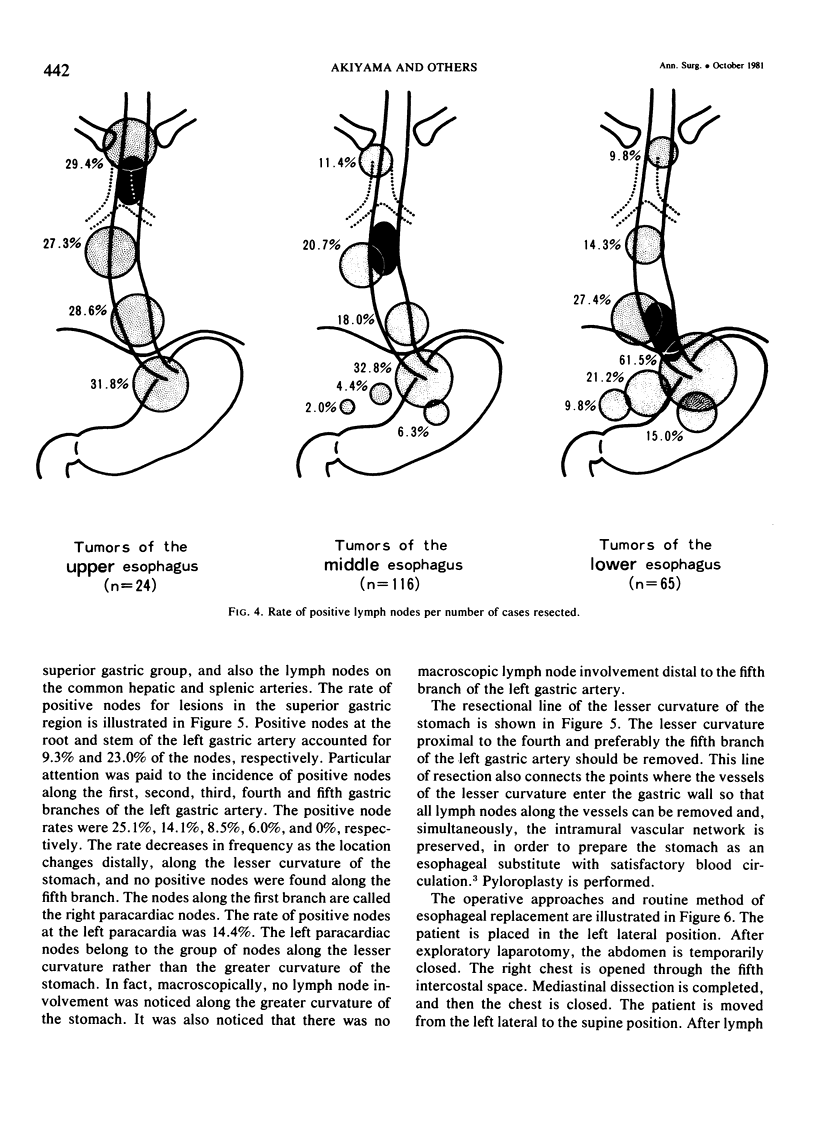
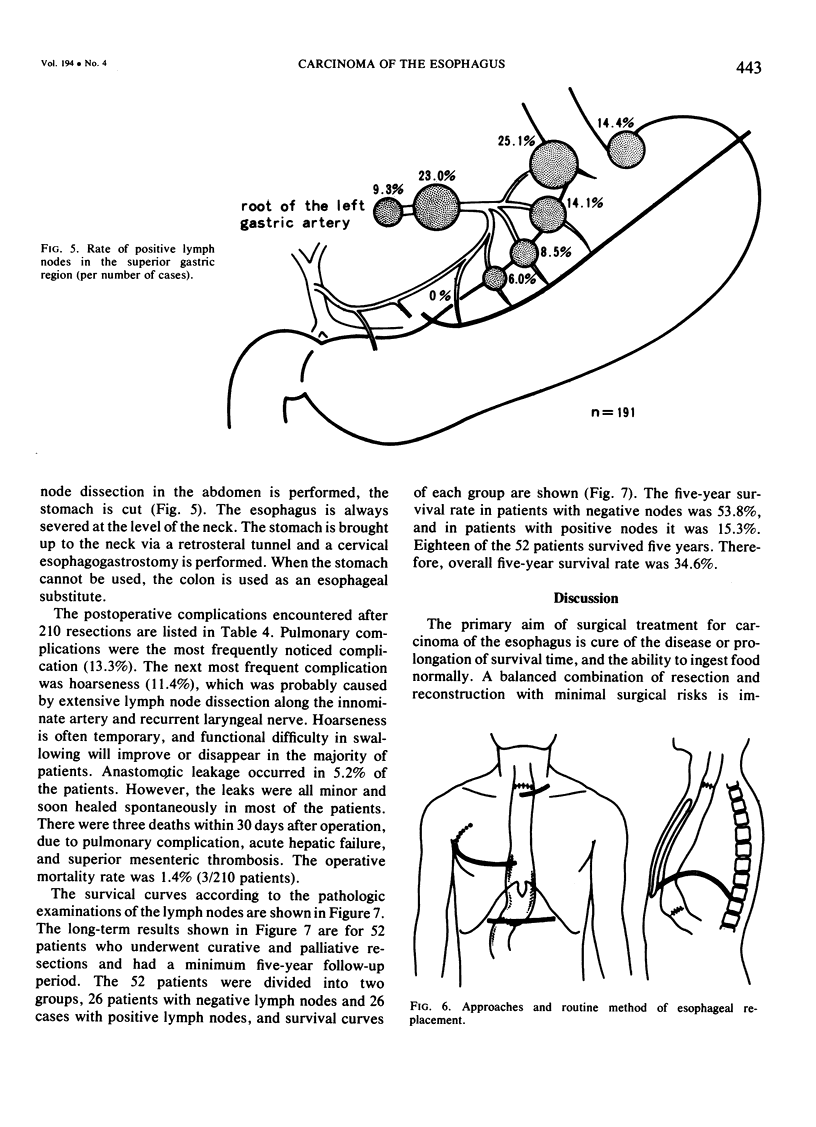
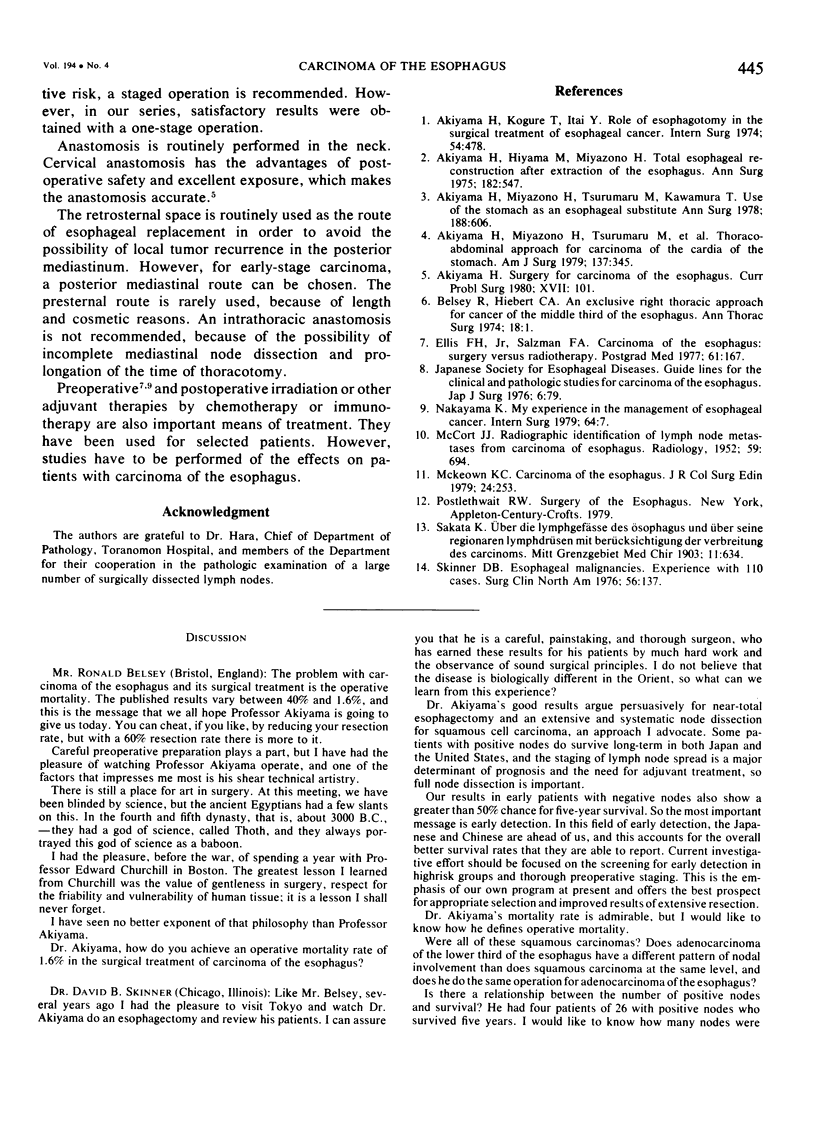
Extensive lymph node dissections in the posterior mediastinum and abdomen were performed during resections of esophageal carcinomas. Analysis of lymph nodes demonstrated a widespread distribution of positive lymph nodes regardless of the location of the tumor. The distribution of positive lymph nodes was noticed in the area between the superior mediastinum and the celiac region. The studies were also made on the distribution of positive lymph nodes in the superior gastric region, particularly in the region of the lesser curvature of the stomach. The following principles should be followed when carcinoma of the esophagus is surgically treated. 1) Lymph node dissection of the whole length of the posterior mediastinum, superior gastric region, and celiac region must be performed. 2) Total thoracic and abdominal esophagectomy with resection of the proximal lesser curvature and cardia, including the first to fourth branches, and preferably the fifth branch of the left gastric artery, is mandatory in order to remove possible lymphatic and intramural spread of tumors. 3) Satisfactory esophageal replacement in one stage must follow. Of the Toranomon Hospital, 210 underwent resections and reconstructions, for a resectability rate of 59.3%. The operative mortality rate was 1.4% and the overall five-year survival rate was 34.6%.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Akiyama H., Hiyama M., Miyazono H. Total esophageal reconstruction after extraction of the esophagus. Ann Surg. 1975 Nov;182(5):547–552. doi: 10.1097/00000658-197511000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Akiyama H., Kogure T., Itai Y. Role of esophagotomy in the surgical treatment of esophageal cancer. Int Surg. 1974 Sep;59(9):478–482. [PubMed] [Google Scholar]
- Akiyama H., Miyazono H., Tsurumaru M., Hashimoto C., Kawamura T. Thoracoabdominal approach for carcinoma of the cardia of the stomach. Am J Surg. 1979 Mar;137(3):345–349. doi: 10.1016/0002-9610(79)90064-3. [DOI] [PubMed] [Google Scholar]
- Akiyama H., Miyazono H., Tsurumaru M., Hashimoto C., Kawamura T. Use of the stomach as an esophageal substitute. Ann Surg. 1978 Nov;188(5):606–610. doi: 10.1097/00000658-197811000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Belsey R., Hiebert C. A. An exclusive right thoracic approach for cancer of the middle third of the esophagus. Ann Thorac Surg. 1974 Jul;18(1):1–15. doi: 10.1016/s0003-4975(10)65712-8. [DOI] [PubMed] [Google Scholar]
- Ellis F. H., Jr, Salzman F. A. Carcinoma of the esophagus: surgery versus radiotherapy. Postgrad Med. 1977 Feb;61(2):167–174. doi: 10.1080/00325481.1977.11712123. [DOI] [PubMed] [Google Scholar]
- MCCORT J. J. Radiographic identification of lymph node metastases from carcinoma of the esophagus. Radiology. 1952 Nov;59(5):694–711. doi: 10.1148/59.5.694. [DOI] [PubMed] [Google Scholar]
- Nakayama K. My experience in the management of esophageal cancer. Int Surg. 1979 May-Jul;64(4):7–11. [PubMed] [Google Scholar]
- Skinner D. B. Esophageal malignancies. Experience with 110 cases. Surg Clin North Am. 1976 Feb;56(1):137–147. doi: 10.1016/s0039-6109(16)40842-x. [DOI] [PubMed] [Google Scholar]