

Abstract
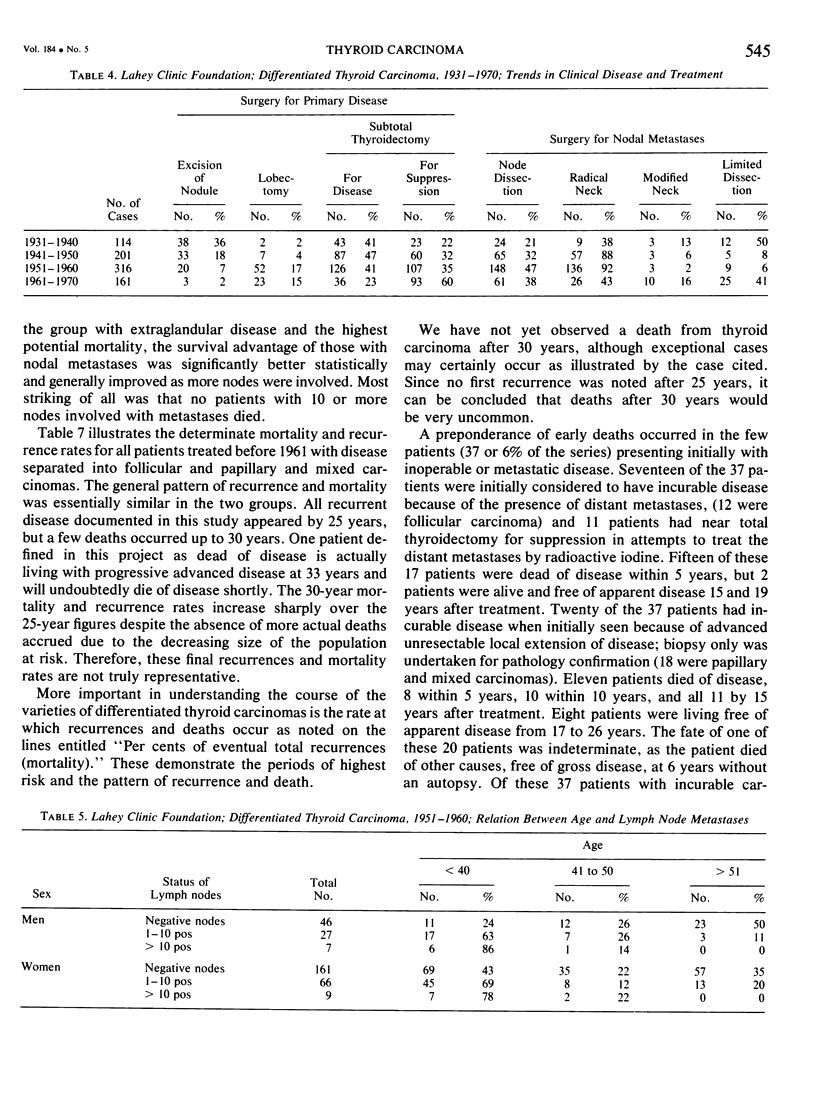
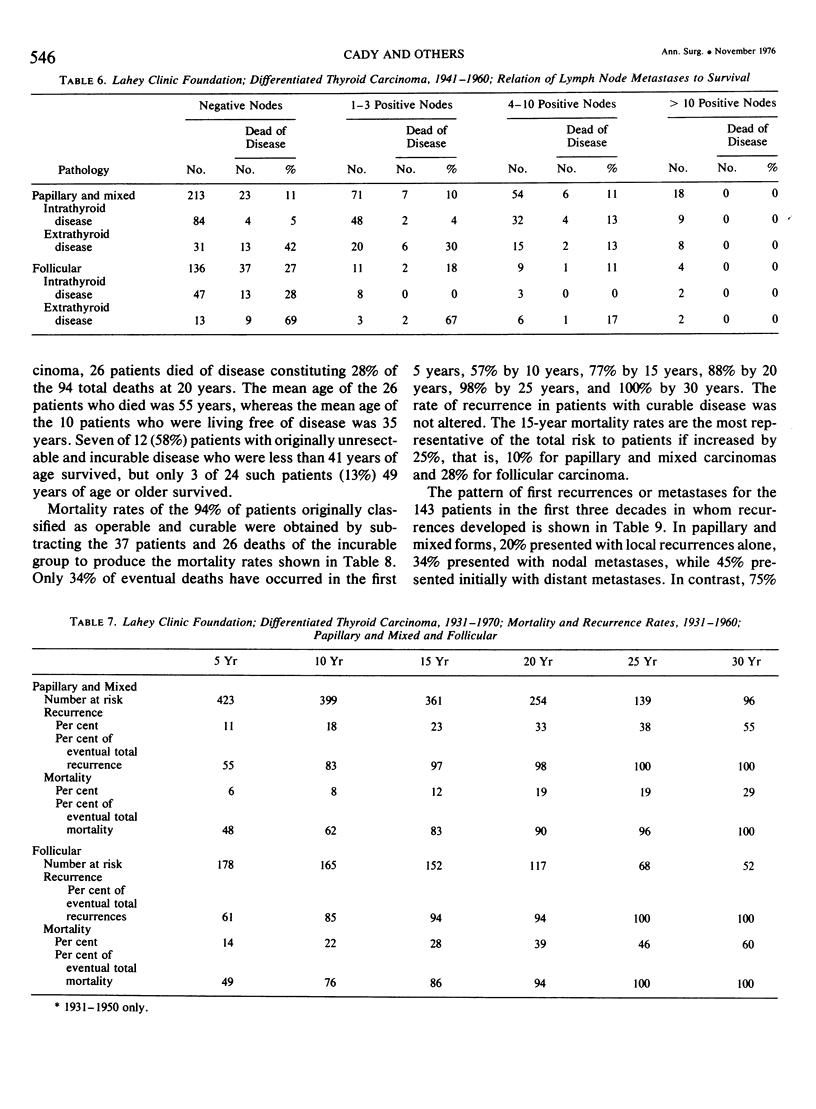
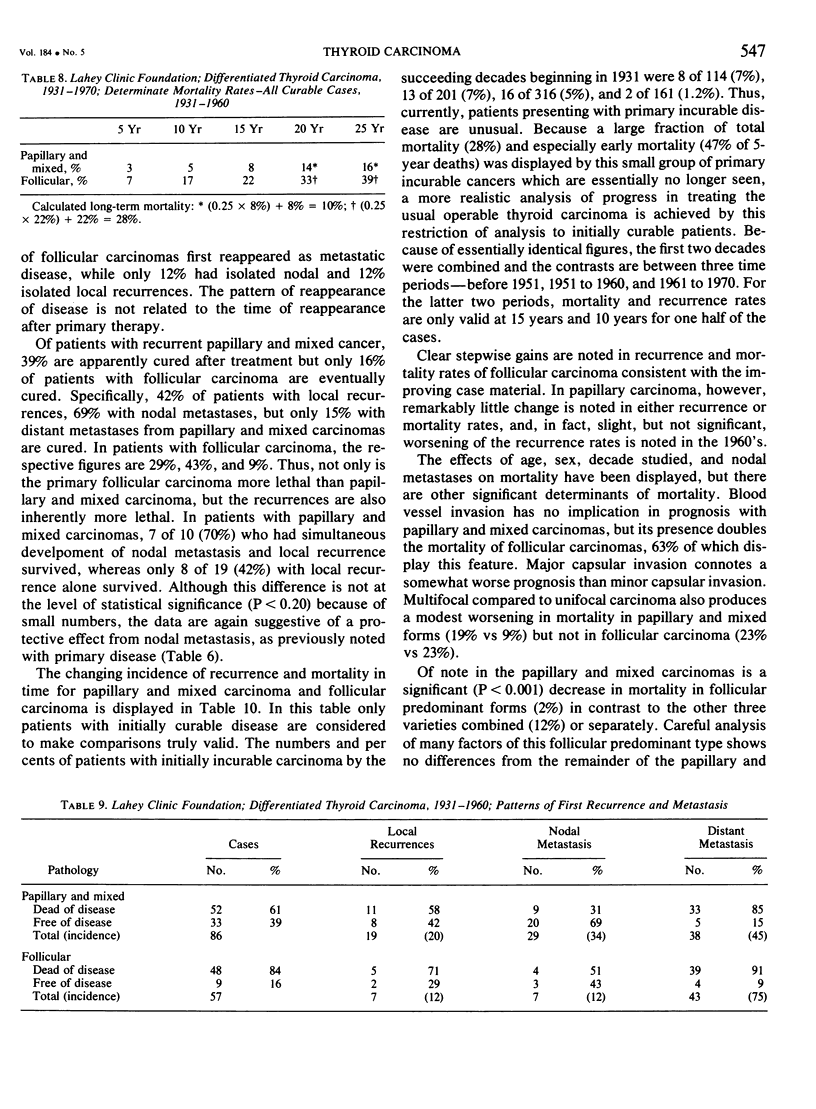
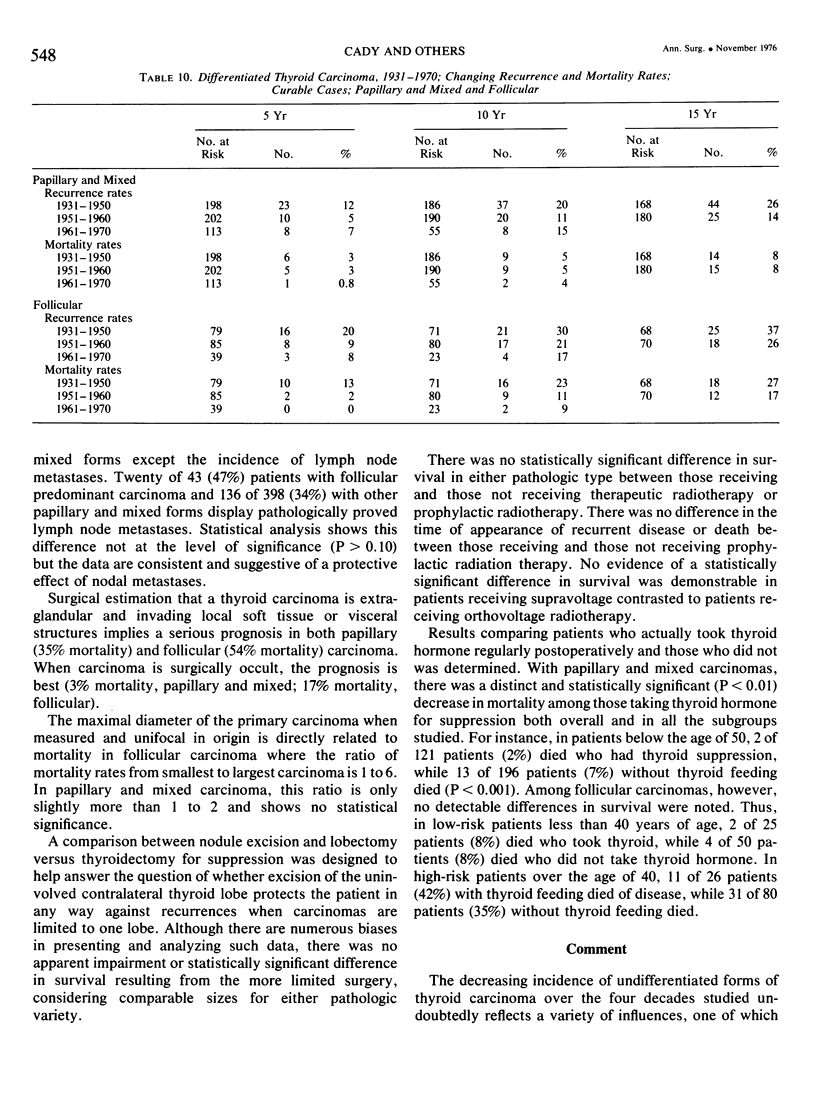
Records of 792 patients with differentiated thyroid carcinoma seen at the Lahey Clinic Foundation over a 40-year period were analyzed; 631 patients had a minimum followup period of 15 years. Differentiated types currently constitute nearly 90% of thyroid carcinomas. The clinical presentation has improved substantially through the years, and the results of treatment generally have improved. The per cent of patients with primarily incurable and locally unresectable disease or distant metastases has decreased from 7% before 1950 to 1% currently, and this group resulted in almost one third of the total fatalities and one half of fatalities within the first 5 years after treatment. Clear relationships were demonstrated between older age, men, extraglandular extension, blood vessel invasion, major capsular involvement, multifocal disease, and higher mortality rates. Lymph node metastases were found to exert a protective effect in all categories of disease analyzed, and this effect was directly related to the number of lymph node metastases present such that no deaths occurred in those patients who had more than 10 node metastases. Surgical treatment recommended is subtotal thyroidectomy for patients at high risk of death from disease as defined by combinations of age, sex, and extraglandular extension. Patients at low risk or with small carcinomas can be treated satisfactorily by lobectomy. Lymph node resections should be of a limited type or a modified neck dissection and should be performed only therapeutically. No improvement, as judged by mortality or recurrence rates, could be demonstrated by the use of radio therapy after surgery, and its use should be discouraged. Thyroid hormone administered for suppression of endogenous thyroid-stimulating hormone production improved mortality rates significantly in patients with papillary and mixed forms of carcinoma in all age groups but did not affect survival in patients with follicular carcinoma of the thyroid.20
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Amino N., Pysher T., Cohen E. P., Degroot L. J. Immunologic aspects of human thyroid cancer. Humoral and cell-mediated immunity, and a trial of immunotherapy. Cancer. 1975 Sep;36(3):963–973. doi: 10.1002/1097-0142(197509)36:3<963::aid-cncr2820360319>3.0.co;2-3. [DOI] [PubMed] [Google Scholar]
- Attie J. N., Khafif R. A., Steckler R. M. Elective neck dissection in papillary carcinoma of the thyroid. Am J Surg. 1971 Oct;122(4):464–471. doi: 10.1016/0002-9610(71)90469-7. [DOI] [PubMed] [Google Scholar]
- CLARK R. L., Jr, WHITE E. C., RUSSELL W. O. Total thyroidectomy for cancer of the thyroid: significance of intraglandular dissemination. Ann Surg. 1959 Jun;149(6):858–866. doi: 10.1097/00000658-195906000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- CRILE G., Jr SURVIVAL OF PATIENTS WITH PAPILLARY CARCINOMA OF THE THYROID AFTER CONSERVATIVE OPERATIONS. Am J Surg. 1964 Dec;108:862–866. doi: 10.1016/0002-9610(64)90048-0. [DOI] [PubMed] [Google Scholar]
- Clark R. L., Hickey R. C., Butler J. J., Ibanez M. L., Ballantyne A. J. Thyroid cancer discovered incidentally during treatment of an unrelated head and neck cancer: review of 16 cases. Ann Surg. 1966 May;163(5):665–671. doi: 10.1097/00000658-196605000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeGroot L., Paloyan E. Thyroid carcinoma and radiation. A Chicago endemic. JAMA. 1973 Jul 30;225(5):487–491. [PubMed] [Google Scholar]
- Favus M. J., Schneider A. B., Stachura M. E., Arnold J. E., Ryo U. Y., Pinsky S. M., Colman M., Arnold M. J., Frohman L. A. Thyroid cancer occurring as a late consequence of head-and-neck irradiation. Evaluation of 1056 patients. N Engl J Med. 1976 May 6;294(19):1019–1025. doi: 10.1056/NEJM197605062941901. [DOI] [PubMed] [Google Scholar]
- HIRABAYASHI R. N., LINDSAY S. THE RELATION OF THYROID CARCINOMA AND CHRONIC THYROIDITIS. Surg Gynecol Obstet. 1965 Aug;121:243–252. [PubMed] [Google Scholar]
- HIRABAYASHI R. N., LINDSAYS Carcinoma of the thyroid gland: a statistical study of 390 patients. J Clin Endocrinol Metab. 1961 Dec;21:1596–1610. doi: 10.1210/jcem-21-12-1596. [DOI] [PubMed] [Google Scholar]
- Hutter R. V., Tollefsen H. R., De Cosse J. J., Foote F. W., Jr, Frazell E. L. Spindle and giant cell metaplasia in papillary carcinoma of the thyroid. Am J Surg. 1965 Oct;110(4):660–668. doi: 10.1016/0002-9610(65)90057-7. [DOI] [PubMed] [Google Scholar]
- Ibanez M. L., Russell W. O., Albores-Saavedra J., Lampertico P., White E. C., Clark R. L. Thyroid carcinoma--biologic behavior and mortality. Postmortem findings in 42 cases, including 27 in which the disease was fatal. Cancer. 1966 Aug;19(8):1039–1052. doi: 10.1002/1097-0142(196608)19:8<1039::aid-cncr2820190802>3.0.co;2-1. [DOI] [PubMed] [Google Scholar]
- MEIER D. W., WOOLNER L. B., BEAHRS O. H., McCONAHEY W. M. Parenchymal findings in thyroidal carcinoma: pathologic study of 256 cases. J Clin Endocrinol Metab. 1959 Jan;19(1):162–171. doi: 10.1210/jcem-19-1-162. [DOI] [PubMed] [Google Scholar]
- Marchetta F. C., Sako K., Matsuura H. Modified neck dissection for carcinoma of the thyroid gland. Am J Surg. 1970 Oct;120(4):452–455. doi: 10.1016/s0002-9610(70)80005-8. [DOI] [PubMed] [Google Scholar]
- Noguchi S., Noguchi A., Murakami N. Papillary carcinoma of the thyroid. I. Developing pattern of metastasis. Cancer. 1970 Nov;26(5):1053–1060. doi: 10.1002/1097-0142(197011)26:5<1053::aid-cncr2820260513>3.0.co;2-x. [DOI] [PubMed] [Google Scholar]
- Smedal M. I., Salzman F. A., Meissner W. A. The value of 3 mv. roentgen-ray therapy in differentiated thyroid carcinoma. Am J Roentgenol Radium Ther Nucl Med. 1967 Feb;99(2):352–364. doi: 10.2214/ajr.99.2.352. [DOI] [PubMed] [Google Scholar]
- Tollefsen H. R., Shah J. P., Huvos A. G. Papillary carcinoma of the thyroid. Recurrence in the thyroid gland after initial surgical treatment. Am J Surg. 1972 Oct;124(4):468–472. doi: 10.1016/0002-9610(72)90068-2. [DOI] [PubMed] [Google Scholar]
- VEITH F. J., BROOKS J. R., GRIGSBY W. P., SELENKOW H. A. THE NODULAR THYROID GLAND AND CANCER. A PRACTICAL APPROACH TO THE PROBLEM. N Engl J Med. 1964 Feb 27;270:431–436. doi: 10.1056/NEJM196402272700901. [DOI] [PubMed] [Google Scholar]
- Wilson S. M., Platz C., Block G. M. Thyroid carcinoma after irradiation. Characteristics and treatment. Arch Surg. 1970 Apr;100(4):330–337. doi: 10.1001/archsurg.1970.01340220006002. [DOI] [PubMed] [Google Scholar]