

Abstract
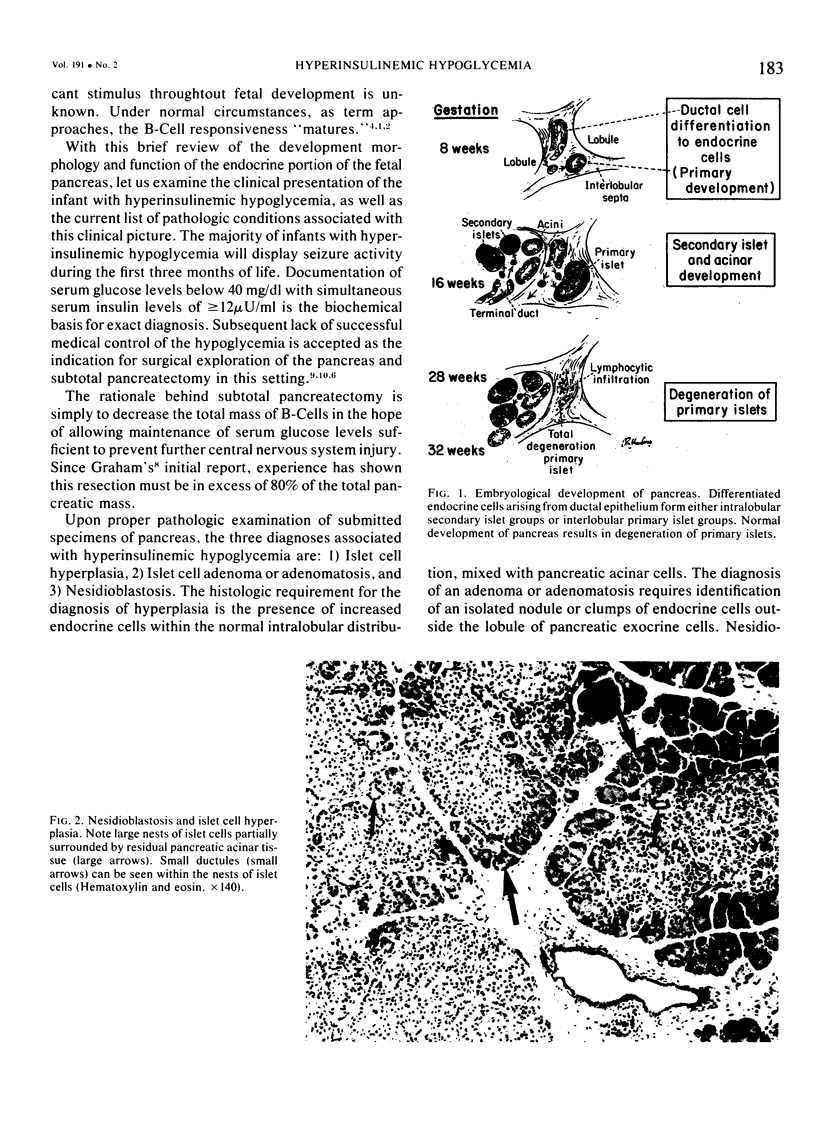
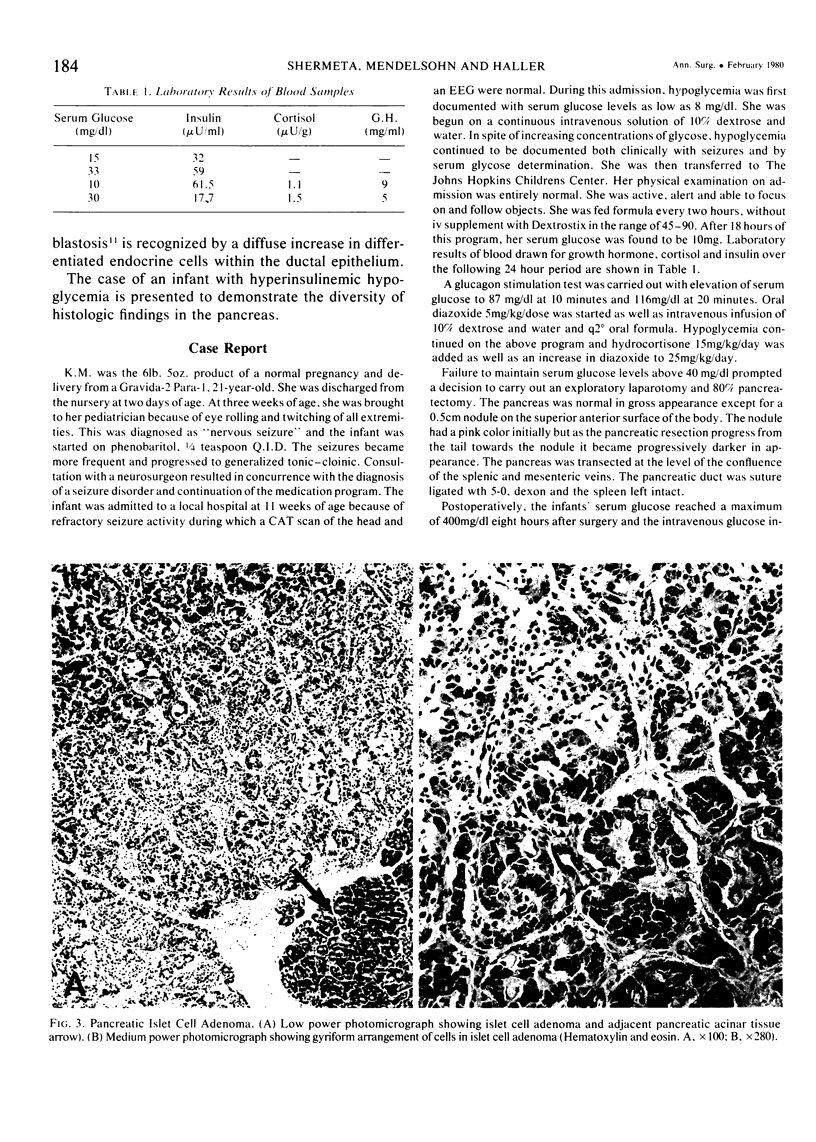
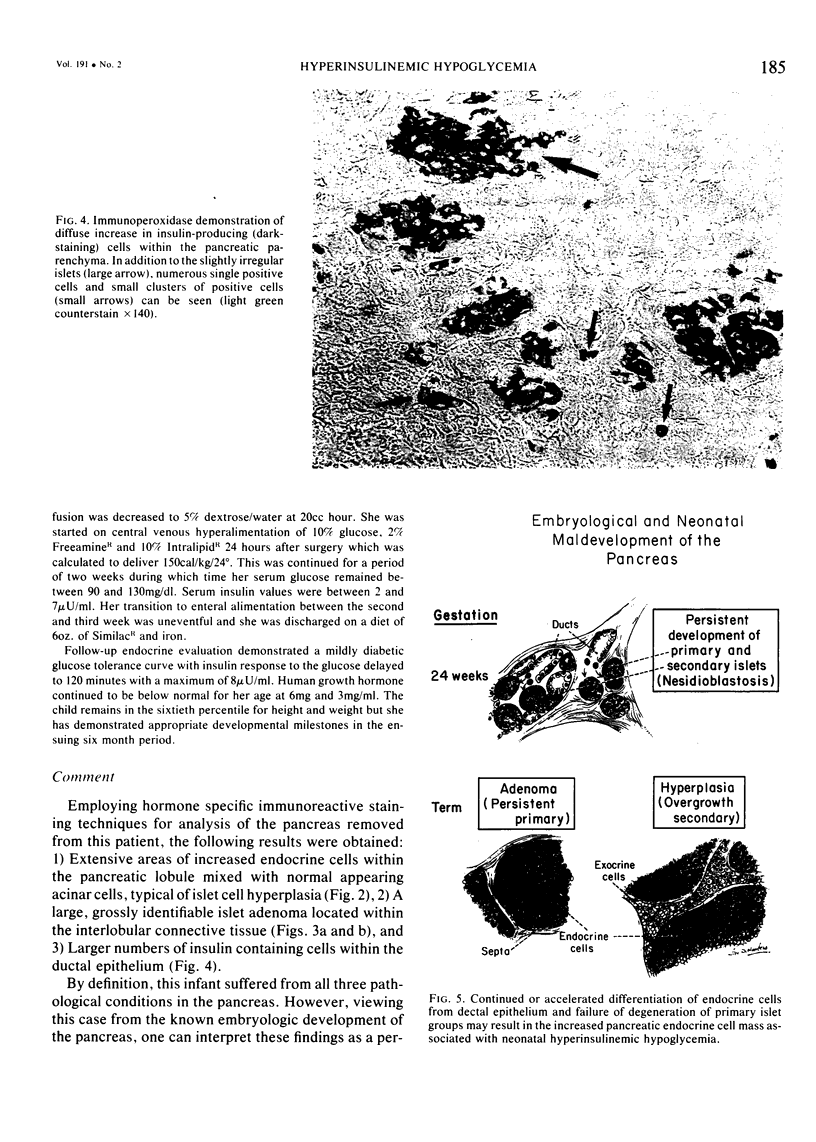
Early in development, the fetal pancreas is characterized by the presence of two distinct generations of endocrine cells and a B-Cell mass that is unresponsive to acute changes in circulating glucose levels. Near the end of intrauterine development, the normal pancreas has "matured" and contains a single generation of endocrine cells and B-Cells that are responsive to changes in glucose concentrations. Recent microscopic examination of resected pancreatic tissue from an infant with hyperinsulinemic hypoglycermia revealed a combination of all three of the currently accepted findings in this neonatal condition: hyperplasia, adenomatosis, and nesidioblastosis. These observations prompted the following hypothesis: When compared to the usual histology of the developing pancreas, nesidioblastosis may be interpreted as an abnormal continuation of normal proliferation of endocrine cells; hyperplasia may be a specific overproduction of the Secondary Islands of Langerhans; and adenomatosis may be an abnormal continuation or overgrowth of the Primary Island of Langerhans. Such extrapolation suggests that infants with hyperinsulinemic hypoglycemia may represent a failure in the normal histological and functional maturation of the endocrine portion of the fetal pancreas.
Full text
PDF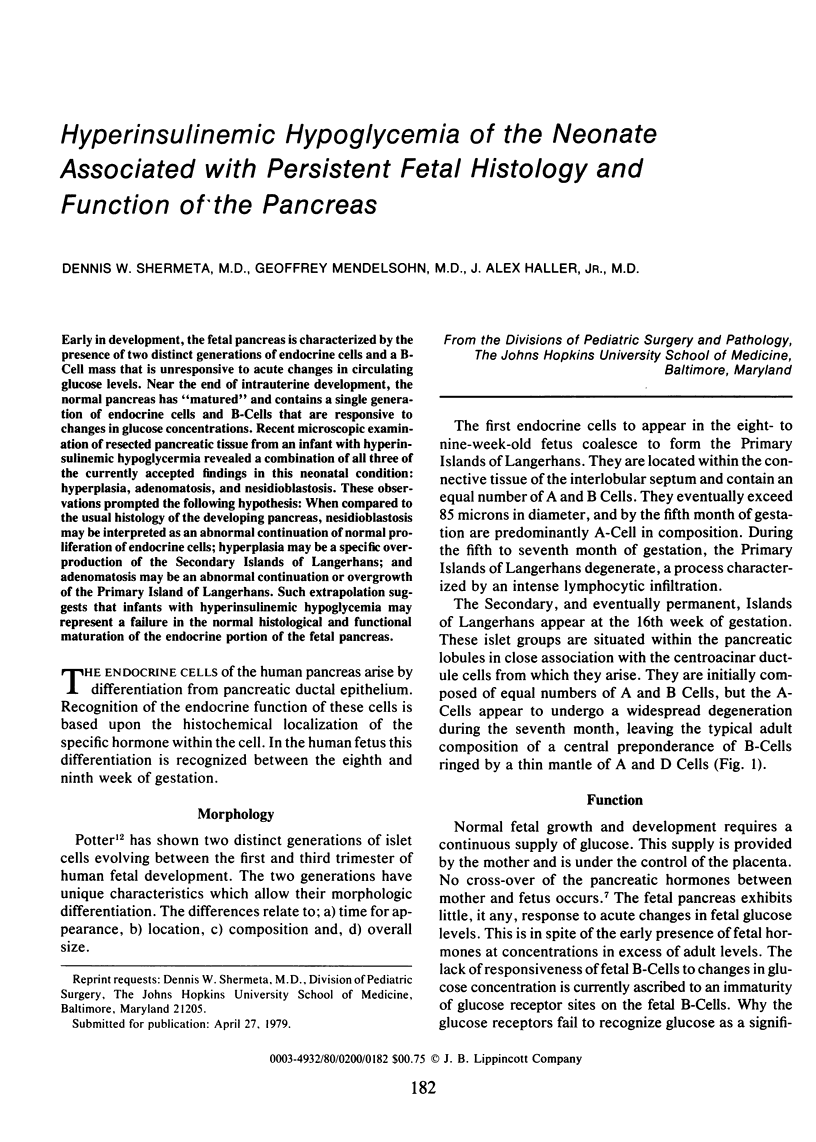

Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Alexander D. P., Britton H. G., Nixon D. A. Further observations on the administration of anti-insulin serum to lambs in the perinatal period. Biol Neonate. 1971;19(4):451–458. doi: 10.1159/000240437. [DOI] [PubMed] [Google Scholar]
- Asplund K. Dynamics of insulin release from the foetal and neonatal rat pancreas. Eur J Clin Invest. 1973 Jul;3(4):338–344. doi: 10.1111/j.1365-2362.1973.tb00360.x. [DOI] [PubMed] [Google Scholar]
- Bucha V., Taylor R. E., Berger R., Haury E. W. Geomagnetic Intensity: Changes during the Past 3000 Years in the Western Hemisphere. Science. 1970 Apr 3;168(3927):111–114. doi: 10.1126/science.168.3927.111. [DOI] [PubMed] [Google Scholar]
- Crowder W. L., Maclaren N. K., Gutberlet R. L., Frost J. L., Mason G. R., Cornblath M. Neonatal pancreatic beta-cell hyperplasia: report of a case with failure of diazoxide and benefit of early subtotal pancreatectomy. Pediatrics. 1976 Jun;57(6):897–900. [PubMed] [Google Scholar]
- FERNER H. The A- and B-cells of the pancreatic islets as sources of the antagonistic hormones glucagon and insulin; the shift of the AB-relation in diabetes mellitus. Am J Dig Dis. 1953 Oct;20(10):301–306. doi: 10.1007/BF02895538. [DOI] [PubMed] [Google Scholar]
- Fonkalsrud E. W., Trout H. H., 3rd, LaFranchi S., Dakake C. Idiopathic hypoglycemia in infancy. Surgical management. Arch Surg. 1974 Jun;108(6):801–804. doi: 10.1001/archsurg.1974.01350300043012. [DOI] [PubMed] [Google Scholar]
- Gabbe S. G., Quilligan E. J. Fetal carbohydrate metabolism: its clinical importance. Am J Obstet Gynecol. 1977 Jan 1;127(1):92–103. doi: 10.1016/0002-9378(77)90321-0. [DOI] [PubMed] [Google Scholar]
- Hamilton J. P., Baker L., Kaye R., Koop C. E. Subtotal pancreatectomy in the management of severe persistant idiopathic hypoglycemia in children. Pediatrics. 1967 Jan;39(1):49–58. [PubMed] [Google Scholar]
- Heitz P. U., Klöppel G., Häcki W. H., Polak J. M., Pearse A. G. Nesidioblastosis: the pathologic basis of persistent hyperinsulinemic hypoglycemia in infants. Morphologic and quantitative analysis of seven cases based on specific immunostaining and electron microscopy. Diabetes. 1977 Jul;26(7):632–642. doi: 10.2337/diab.26.7.632. [DOI] [PubMed] [Google Scholar]
- LIU H. M., POTTER E. L. Development of the human pancreas. Arch Pathol. 1962 Nov;74:439–452. [PubMed] [Google Scholar]