

Abstract
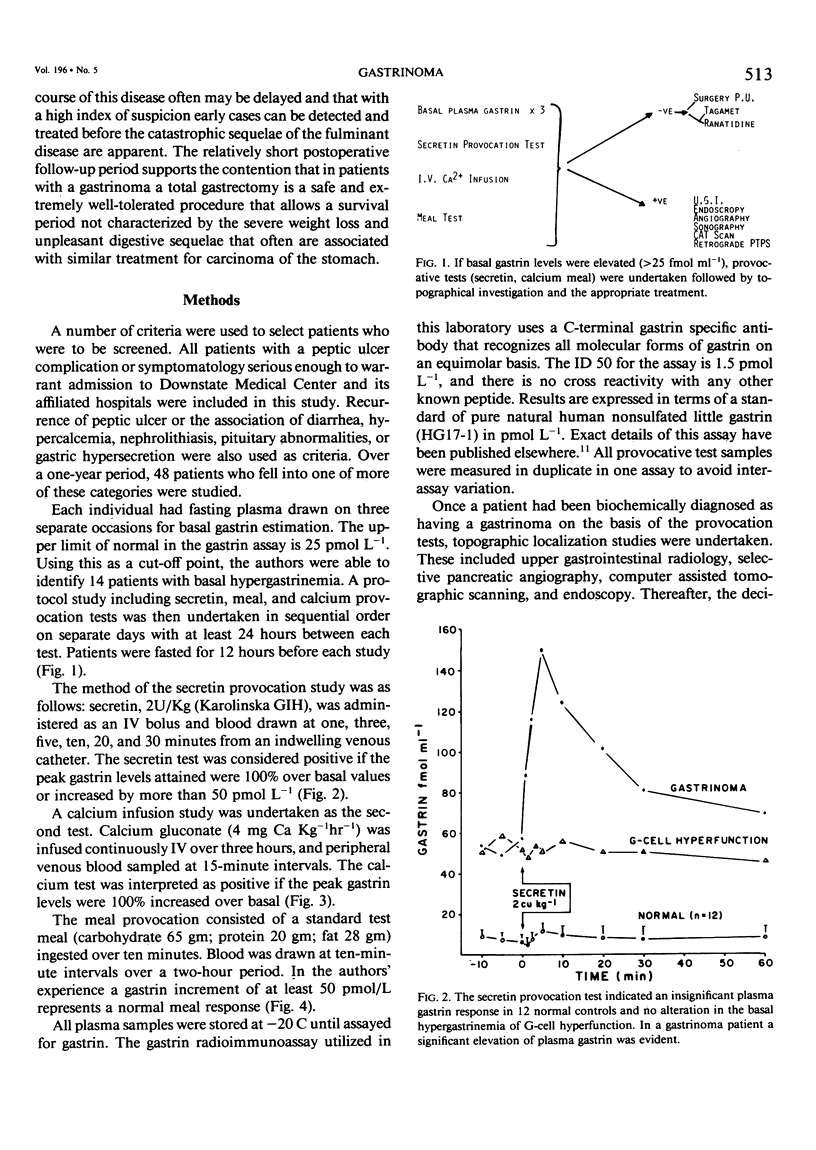
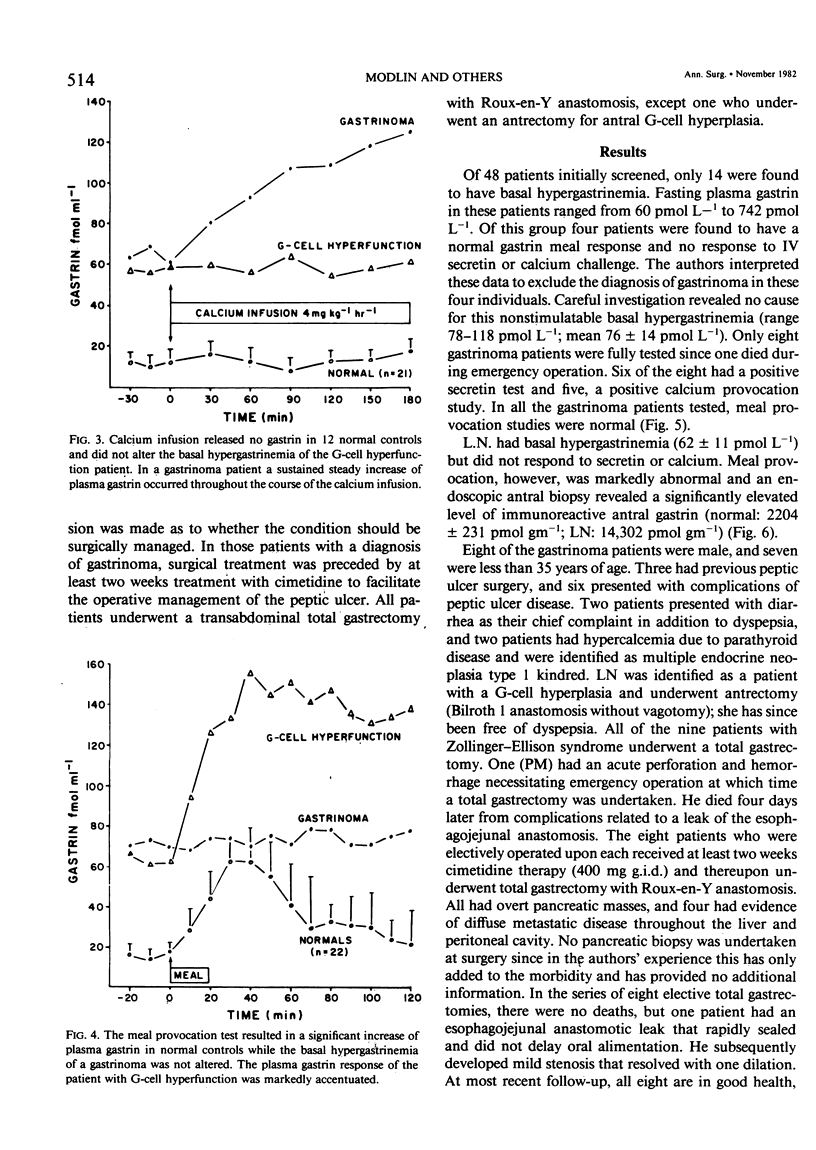
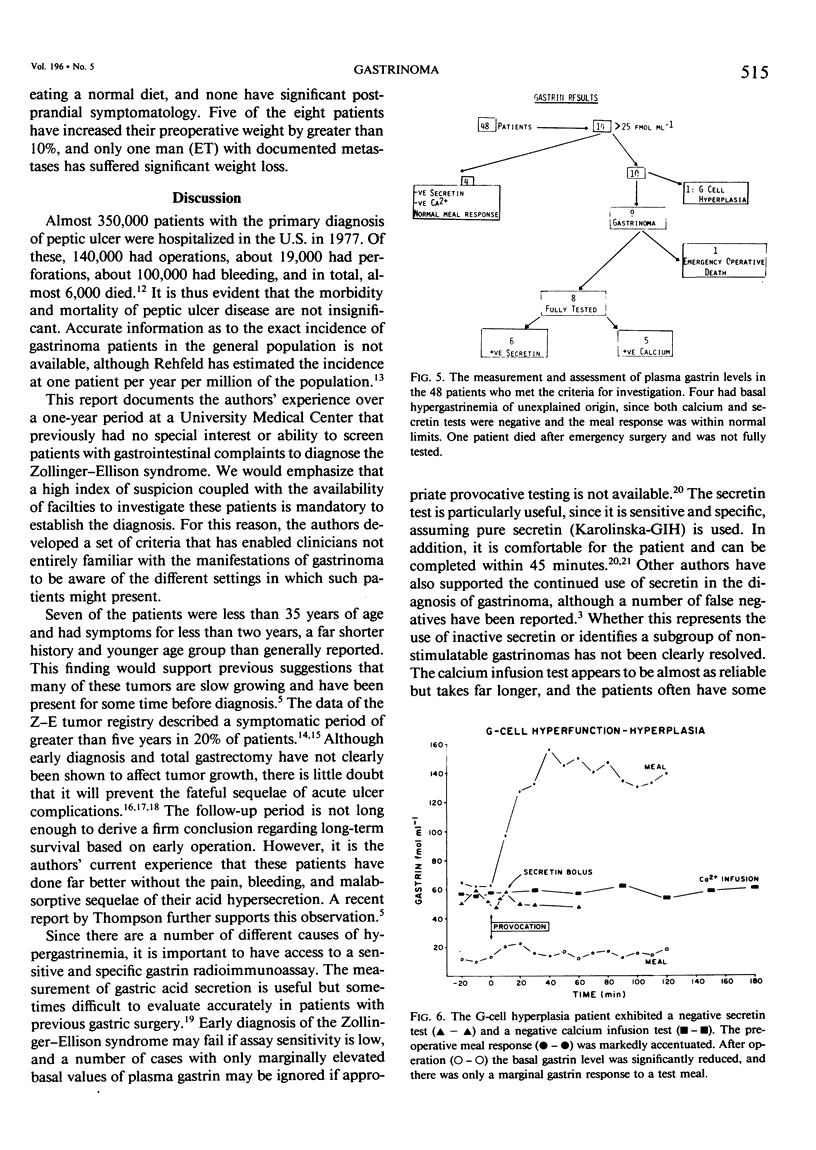
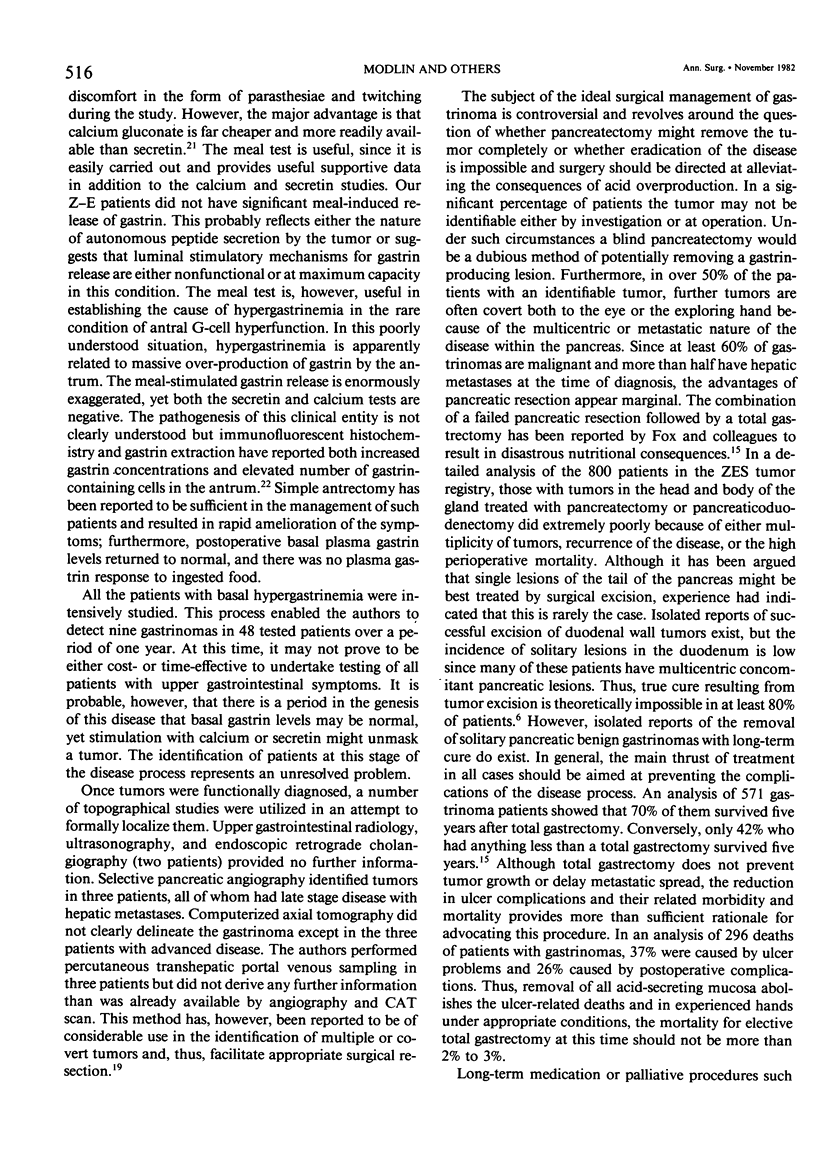
Despite the increasing awareness of gastrinoma and its lethal peptic ulcer sequelae, the diagnosis is often initially missed or made as a terminal event. The authors screened all patients with peptic ulcer symptoms serious enough to warrant hospital admission or those associated with diarrhea, nephrolithiasis, hypercalcemia, or pituitary abnormality. In a one-year period (1979-1980) nine (of 14 suspected) new gastrinoma patients were identified using a sensitive and specific gastrin radioimmunoassay in combination with provocative tests including IV secretin, calcium, and food. Conventional upper GI series, CAT scan, arteriography, and endoscopy provided no additional information other than to confirm the presence of ulcer disease. Basal plasma gastrin levels were more than 200 pmol L-1 in only three of the nine (normal fasting plasma gastrin levels are less than 25 pmol L-1). Three patients presented with acute¿ulcer perforation, and the diagnosis of gastrinoma was suspected because of multiple ulcers and pancreatic masses. In three other patients, previous duodenal ulcer surgery had failed. One patient with dyspepsia, high basal plasma gastrin, negative secretin and calcium infusion studies, and a positive meal test was diagnosed as having G-cell hyperplasia; this was confirmed by biopsy and antral gastrin extraction. Antrectomy alone resulted in cure. In all patients tested, a positive calcium infusion or secretin bolus (greater than 100% rise over basal) strongly suggested the diagnosis of gastrinoma, which was confirmed at surgery. In the acute perforations, initial management with omental patch and cimetidine therapy allowed survival of two patients, while emergency total gastrectomy in the third resulted in death due to esophagojejunal leak. Elective patients were treated with cimetidine initially for at least two weeks before total gastrectomy. In this group there were no operative mortalities, and postoperative morbidity was minimal. This series illustrates three important points: (1) careful screening of an ulcer population using gastrin radioimmunoassay and provocative tests has enabled a high yield of gastrinomas while conventional investigations are of minimal values; (2) a high index of suspicion in appropriate cases is necessary; and (3) total gastrectomy performed under elective circumstances is safe and allows the patients to resume a normal and healthy life without the sequelae of aggressive peptic ulceration or daily drug administration.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bradley E. L., 3rd, Isaacs J., Hersh T., Davidson E. D., Millikan W. Nutritional consequences of total gastrectomy. Ann Surg. 1975 Oct;182(4):415–429. doi: 10.1097/00000658-197510000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis C. E., Jr, Vansant J. H. Zollinger-Ellison syndrome. Spontaneous regression of advanced intra-abdominal metastases with 20 year survival. Ann Surg. 1979 May;189(5):620–626. doi: 10.1097/00000658-197905000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deveney C. W., Deveney K. S., Jaffe B. M., Jones R. S., Way L. W. Use of calcium and secretin in the diagnosis of gastrinoma (Zollinger-Ellison syndrome). Ann Intern Med. 1977 Dec;87(6):680–686. doi: 10.7326/0003-4819-87-6-680. [DOI] [PubMed] [Google Scholar]
- Deveney C. W., Deveney K. S., Way L. W. The Zollinger-Ellison syndrome--23 years later. Ann Surg. 1978 Sep;188(3):384–393. doi: 10.1097/00000658-197809000-00014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fabri P. J., Johnson J. A., Ellison E. C. Prediction of progressive disease in Zollinger-Ellison Syndrome-comparison of available preoperative tests. J Surg Res. 1981 Aug;31(2):93–97. doi: 10.1016/0022-4804(81)90035-4. [DOI] [PubMed] [Google Scholar]
- Fox P. S., Hofmann J. W., Decosse J. J., Wilson S. D. The influence of total gastrectomy on survival in malignant Zollinger-Ellison tumors. Ann Surg. 1974 Oct;180(4):558–566. doi: 10.1097/00000658-197410000-00020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fox P. S., Hofmann J. W., Wilson S. D., DeCosse J. J. Surgical management of the Zollinger-Ellison syndrome. Surg Clin North Am. 1974 Apr;54(2):395–407. doi: 10.1016/s0039-6109(16)40287-2. [DOI] [PubMed] [Google Scholar]
- Friesen S. R. Effect of total gastrectomy on the Zollinger-Ellison tumor: observations by second-look procedures. Surgery. 1967 Oct;62(4):609–613. [PubMed] [Google Scholar]
- Ganguli P. C., Polak J. M., Pearse A. G., Elder J. B., Hegarty M. Antral-gastrin-cell hyperplasia in peptic-ulcer disease. Lancet. 1974 Apr 6;1(7858):583–586. doi: 10.1016/s0140-6736(74)92647-6. [DOI] [PubMed] [Google Scholar]
- Ingemansson S., Larsson L. I., Lunderquist A., Stadil F. Pancreatic vein catheterization with gastrin assay in normal patients and in patients with the Zollinger-Ellison syndrome. Am J Surg. 1977 Nov;134(5):558–563. doi: 10.1016/0002-9610(77)90433-0. [DOI] [PubMed] [Google Scholar]
- Isenberg J. I., Walsh J. H., Passaro E., Jr, Moore E. W., Grossman M. I. Unusual effect of secretin on serum gastrin, serum calcium, and gastric acid secretion in a patient with suspected Zollinger-Ellison syndrome. Gastroenterology. 1972 Apr;62(4):626–631. [PubMed] [Google Scholar]
- Lamers C. G., Van Tongeren J. H. Comparative study of the value of the calcium, secretin, and meal stimulated increase in serum gastrin to the diagnosis of the Zollinger-Ellison syndrome. Gut. 1977 Feb;18(2):128–135. doi: 10.1136/gut.18.2.128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCarthy D. M. The place of surgery in the Zollinger-Ellison syndrome. N Engl J Med. 1980 Jun 12;302(24):1344–1347. doi: 10.1056/NEJM198006123022404. [DOI] [PubMed] [Google Scholar]
- Modlin I. M. Endocrine tumors of the pancreas. Surg Gynecol Obstet. 1979 Nov;149(5):751–769. [PubMed] [Google Scholar]
- Rehfeld J. F. Radioimmunoassay in diagnosis, localization and treatment of endocrine tumours in gut and pancreas. Scand J Gastroenterol Suppl. 1979;53:33–38. [PubMed] [Google Scholar]
- Richardson C. T., Feldman M., McClelland R. N., Dickerman R. M., Kumpuris D., Fordtran J. S. Effect of vagotomy in Zollinger-Ellison syndrome. Gastroenterology. 1979 Oct;77(4 Pt 1):682–686. [PubMed] [Google Scholar]
- Stage J. G., Stadil F. The clinical diagnosis of the Zollinger-Ellison syndrome. Scand J Gastroenterol Suppl. 1979;53:79–91. [PubMed] [Google Scholar]
- Zollinger R. M., Ellison E. C., Fabri P. J., Johnson J., Sparks J., Carey L. C. Primary peptic ulcerations of the jejunum associated with islet cell tumors. Twenty-five-year appraisal. Ann Surg. 1980 Sep;192(3):422–430. doi: 10.1097/00000658-198009000-00018. [DOI] [PMC free article] [PubMed] [Google Scholar]