

Abstract
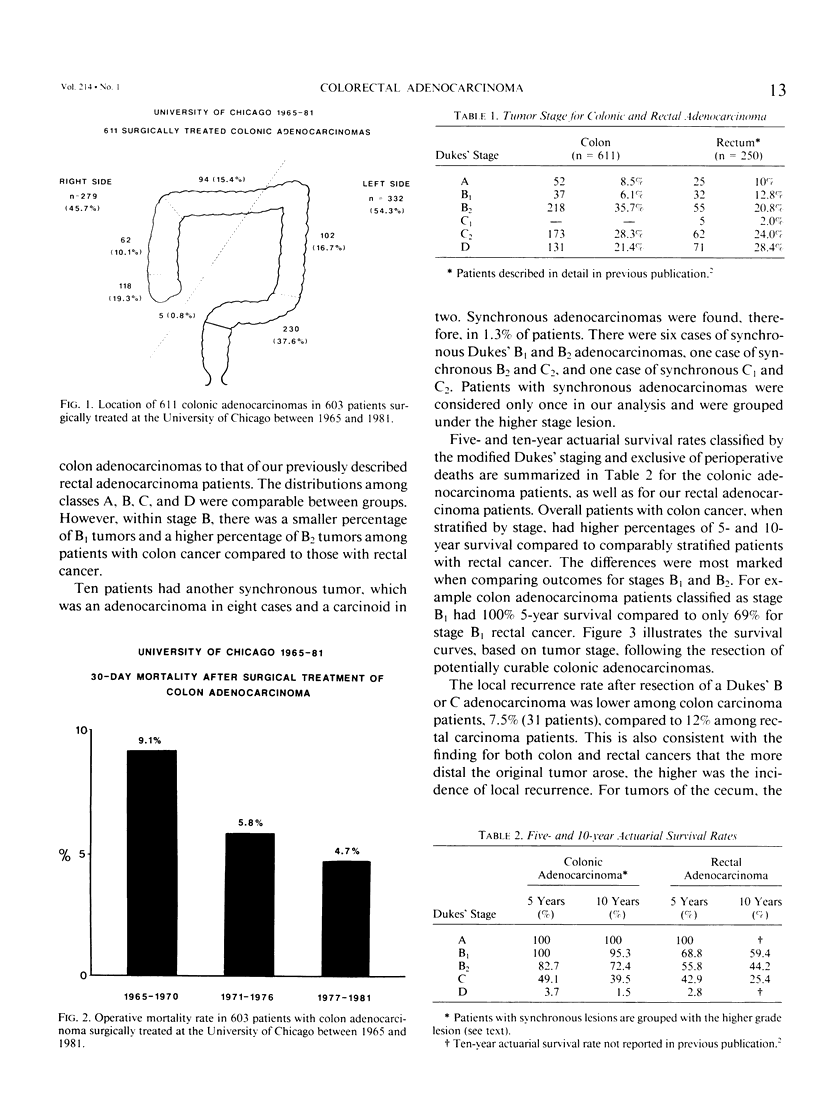
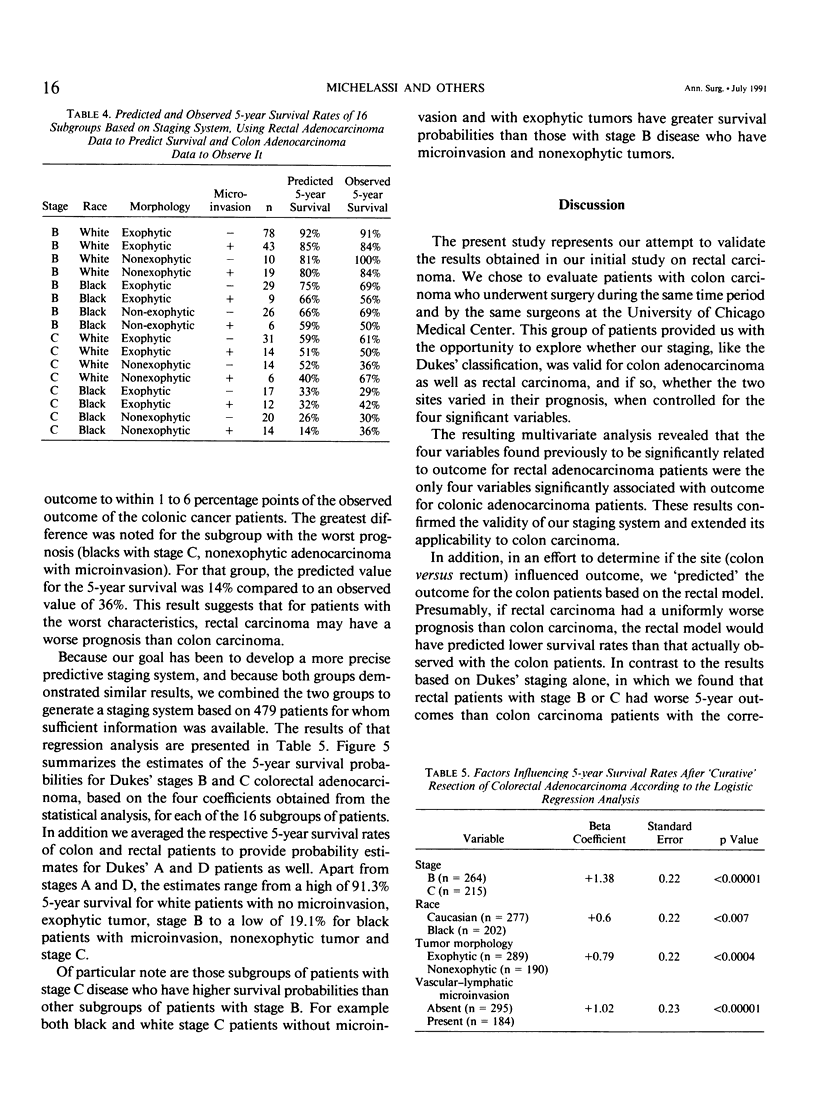
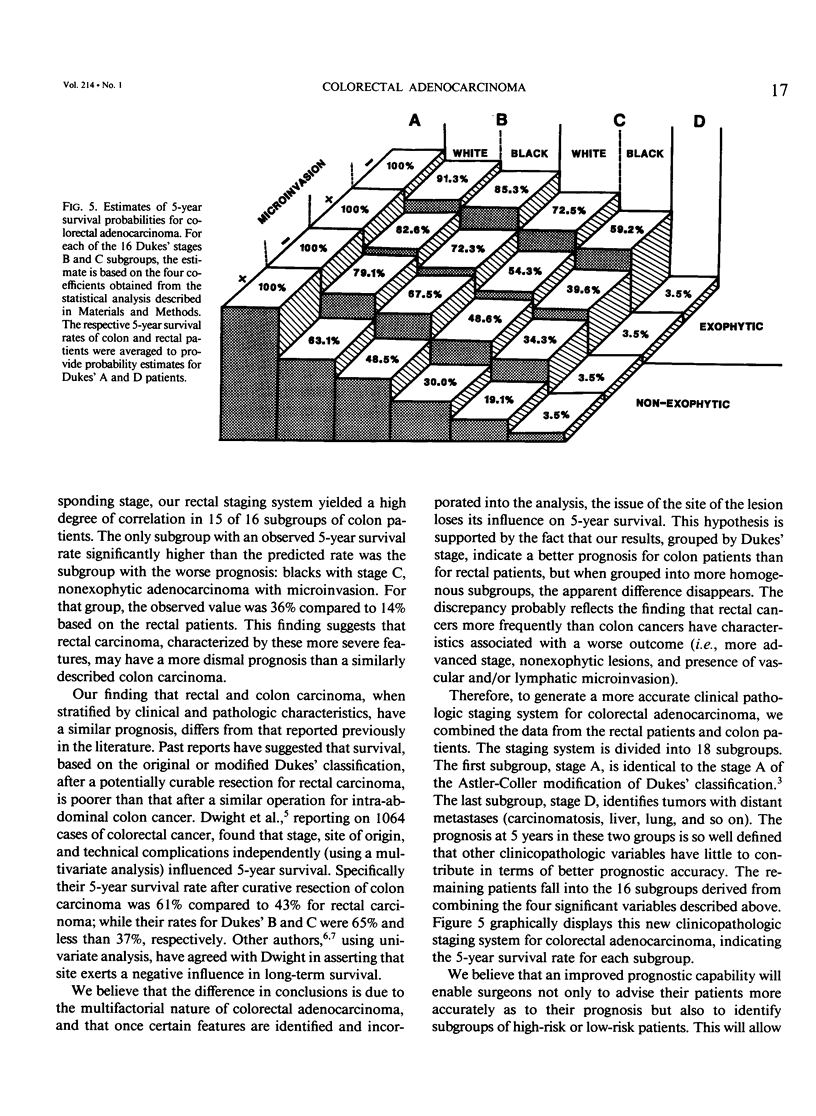
Rectal adenocarcinoma is said to have a poorer outcome than colon adenocarcinoma when compared on the basis of Dukes' staging. However a new staging system, determined by a multivariate analysis of 147 patients with rectal adenocarcinoma, has revealed three other variables significantly related to outcome. Therefore this study analyzed the authors' experience with colonic carcinoma during the same time period as they had studied for rectal carcinoma to determine whether the new staging system is valid for colon carcinoma as well, and, if so, to compare the outcome of patients with colon and rectal carcinoma on the basis of this new staging. A total of 603 patients with 611 colonic adenocarcinoma were operated on at the University of Chicago Medical Center between 1965 and 1981. Two hundred seventy-nine adenocarcinomas (45.7%) were located proximal to the splenic flexure and 332 (54.3%) were located between the splenic flexure and the rectosigmoid. Four hundred sixty-two patients underwent segmental colectomy, 46 subtotal colectomy, 26 total colectomy, 18 proctocolectomy, 5 abdominal-perineal resection, 1 appendectomy, while 20 had local excision of the tumor through colotomy and 25 had permanent diverting stoma as the only procedure. The operative mortality rate was 6.1% in the whole group, but was only 2.7% in the group of potentially curable patients. Complete follow-up was obtained in all patients. To validate a previous staging system for Dukes' B and C rectal adenocarcinoma, the authors investigated the correlation between 5-year survival for colonic carcinoma patients and all relevant variables that they had considered potentially meaningful in the previous study with rectal adenocarcinoma. The resulting multivariate analysis using Cox regression showed that the four variables found previously to be significantly related to outcome for rectal adenocarcinoma patients (stage, race, tumor morphology, and vascular and/or lymphatic microinvasion) were the only four variables significantly (p less than 0.05) associated with outcome for colonic adenocarcinoma patients. In addition, by using the results of their previous staging system for rectal adenocarcinoma patients, they 'predicted' the 5-year survival rates of the colon adenocarcinoma patients, divided in 16 staging subgroups. In subgroups of at least 15 patients, the rectal staging system predicted the outcome to within 1 to 6 percentage points of the observed outcome of the colonic adenocarcinoma patients. Thus this study validates this staging system, incorporating stage, race, tumor morphology, and microinvasion to predict 5-year survival rate more accurately than Dukes' staging alone for both colon and rectal adenocarcinoma.(ABSTRACT TRUNCATED AT 400 WORDS)
Full text
PDF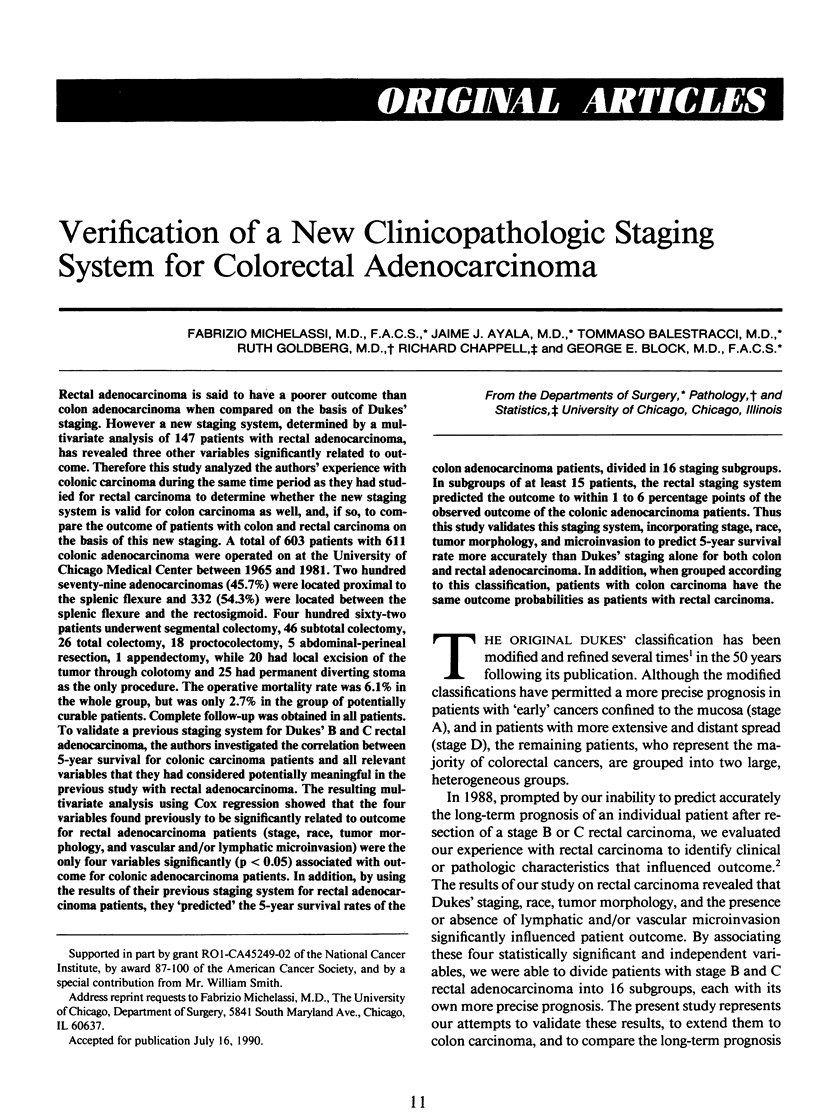

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ASTLER V. B., COLLER F. A. The prognostic significance of direct extension of carcinoma of the colon and rectum. Ann Surg. 1954 Jun;139(6):846–852. doi: 10.1097/00000658-195406000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dwight R. W., Higgins G. A., Keehn R. J. Factors influencing survival after resection in cancer of the colon and rectum. Am J Surg. 1969 Apr;117(4):512–522. doi: 10.1016/0002-9610(69)90010-5. [DOI] [PubMed] [Google Scholar]
- Michelassi F., Block G. E., Vannucci L., Montag A., Chappell R. A 5- to 21-year follow-up and analysis of 250 patients with rectal adenocarcinoma. Ann Surg. 1988 Sep;208(3):379–389. doi: 10.1097/00000658-198809000-00016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sanfelippo P. M., Beahrs O. H. Factors in the prognosis of adenocarcinoma of the colon and rectum. Arch Surg. 1972 Apr;104(4):401–406. doi: 10.1001/archsurg.1972.04180040015003. [DOI] [PubMed] [Google Scholar]
- Spratt J. S., Jr, Spjut H. J. Prevalence and prognosis of individual clinical and pathologic variables associated with colorectal carcinoma. Cancer. 1967 Nov;20(11):1976–1985. doi: 10.1002/1097-0142(196711)20:11<1976::aid-cncr2820201125>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]