

Abstract
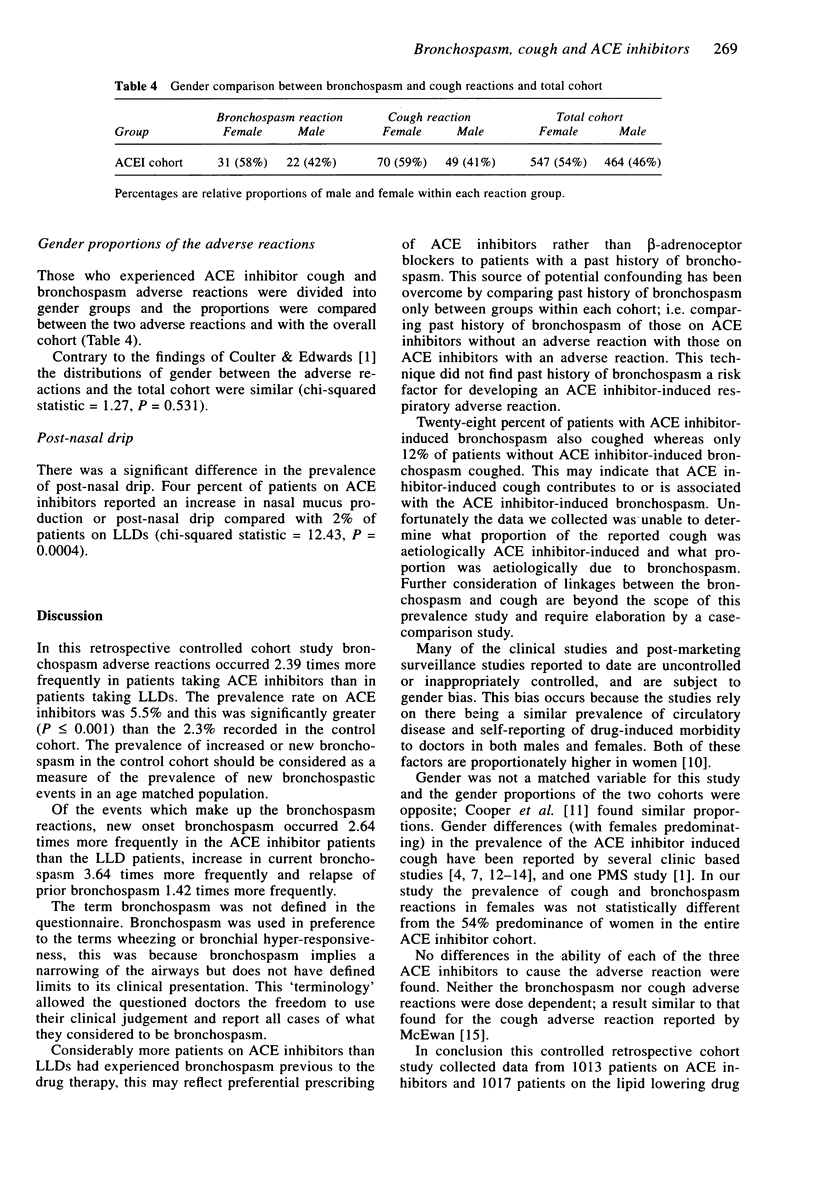
1. We report a controlled retrospective cohort study of respiratory adverse reactions to ACE inhibitors. Bronchospasm and cough occurred at a higher rate in patients treated with ACE inhibitors, no links with sex, past history of bronchospasm, drug type or dose were found. 2. Cohorts of 1013 patients on angiotensin converting enzyme (ACE) inhibitors and 1017 patients on lipid lowering drugs (LLDs) were compared for the occurrence of new bronchospasm, relapse of previous bronchospasm, increase of current bronchospasm, and cough. 3. The prevalence of bronchospasm was 5.5% for patients on ACE inhibitors and 2.3% for patients on LLDs, P < 0.001. The relative risk of a bronchospasm adverse reaction for a patient on an ACE inhibitor compared with a patient on a LLD was 2.39, 95% confidence interval 1.47 to 3.90. 4. No ACE inhibitor specificity, or significant sex differences were found in the prevalence of bronchospasm or cough after correcting for bias implicit in the original cohorts. The bronchospastic reactions were not dose dependent. 5. The prevalence of a past history of bronchospasm in patients reporting ACE inhibitor-induced bronchospasm (16%) was not significantly different from the prevalence in patients on ACE inhibitors without an adverse reaction (13%), P = 0.447. 6. The prevalence of ACE inhibitor cohort cough was 12.3% and 2.7% in the patients on LLDs, P < 0.0001. Cough did not occur more commonly in patients on ACE inhibitors who had experienced any bronchospasm (28%) than in patients on LLDs with bronchospasm (27%).
Full text
PDF



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Boulet L. P., Milot J., Lampron N., Lacourcière Y. Pulmonary function and airway responsiveness during long-term therapy with captopril. JAMA. 1989 Jan 20;261(3):413–416. [PubMed] [Google Scholar]
- Cooper W. D., Sheldon D., Brown D., Kimber G. R., Isitt V. L., Currie W. J. Post-marketing surveillance of enalapril: experience in 11,710 hypertensive patients in general practice. J R Coll Gen Pract. 1987 Aug;37(301):346–349. [PMC free article] [PubMed] [Google Scholar]
- Coulter D. M., Edwards I. R. Cough associated with captopril and enalapril. Br Med J (Clin Res Ed) 1987 Jun 13;294(6586):1521–1523. doi: 10.1136/bmj.294.6586.1521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fuller R. W., Choudry N. B. Increased cough reflex associated with angiotensin converting enzyme inhibitor cough. Br Med J (Clin Res Ed) 1987 Oct 24;295(6605):1025–1026. doi: 10.1136/bmj.295.6605.1025-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hood S., Nicholls M. G., Gilchrist N. L. Cough with angiotensin converting-enzyme inhibitors. N Z Med J. 1987 Jan 28;100(816):6–7. [PubMed] [Google Scholar]
- Irvin J. D., Viau J. M. Safety profiles of the angiotensin converting enzyme inhibitors captopril and enalapril. Am J Med. 1986 Oct 31;81(4C):46–50. doi: 10.1016/0002-9343(86)90945-9. [DOI] [PubMed] [Google Scholar]
- Morris J. A., Gardner M. J. Calculating confidence intervals for relative risks (odds ratios) and standardised ratios and rates. Br Med J (Clin Res Ed) 1988 May 7;296(6632):1313–1316. doi: 10.1136/bmj.296.6632.1313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Semple P. F., Herd G. W. Cough and wheeze caused by inhibitors of angiotensin-converting enzyme. N Engl J Med. 1986 Jan 2;314(1):61–61. doi: 10.1056/NEJM198601023140119. [DOI] [PubMed] [Google Scholar]
- Skidgel R. A., Erdös E. G. The broad substrate specificity of human angiotensin I converting enzyme. Clin Exp Hypertens A. 1987;9(2-3):243–259. doi: 10.3109/10641968709164184. [DOI] [PubMed] [Google Scholar]
- Strocchi E., Valtancoli G., Ambrosioni E. The incidence of cough during treatment with angiotensin converting enzyme inhibitors. J Hypertens Suppl. 1989 Dec;7(6):S308–S309. doi: 10.1097/00004872-198900076-00150. [DOI] [PubMed] [Google Scholar]
- Town G. I., Hallwright G. P., Maling T. J., O'Donnell T. V. Angiotensin converting enzyme inhibitors and cough. N Z Med J. 1987 Mar 25;100(820):161–163. [PubMed] [Google Scholar]
- Wingard D. L., Cohn B. A., Kaplan G. A., Cirillo P. M., Cohen R. D. Sex differentials in morbidity and mortality risks examined by age and cause in the same cohort. Am J Epidemiol. 1989 Sep;130(3):601–610. doi: 10.1093/oxfordjournals.aje.a115374. [DOI] [PubMed] [Google Scholar]
- Yeo W. W., Foster G., Ramsay L. E. Prevalence of persistent cough during long-term enalapril treatment: controlled study versus nifedipine. Q J Med. 1991 Sep;80(293):763–770. [PubMed] [Google Scholar]
- Yeo W. W., Ramsay L. E. Persistent dry cough with enalapril: incidence depends on method used. J Hum Hypertens. 1990 Oct;4(5):517–520. [PubMed] [Google Scholar]