

Abstract
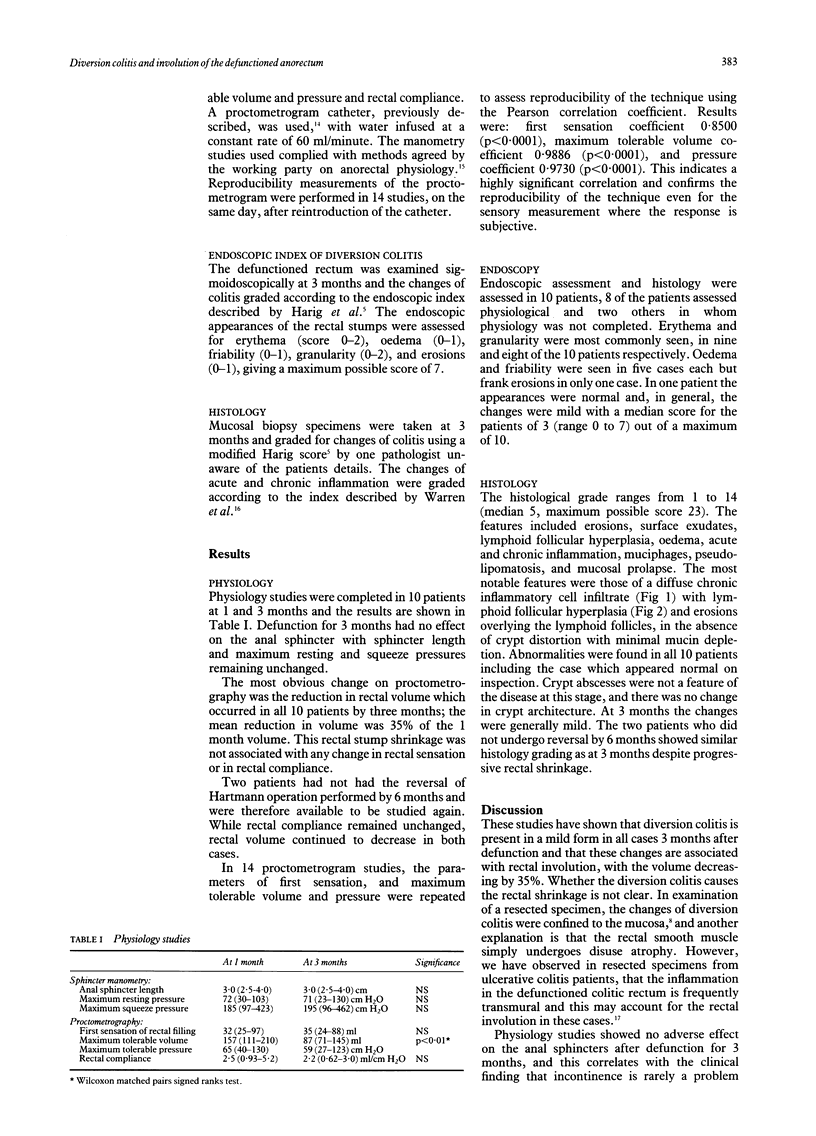
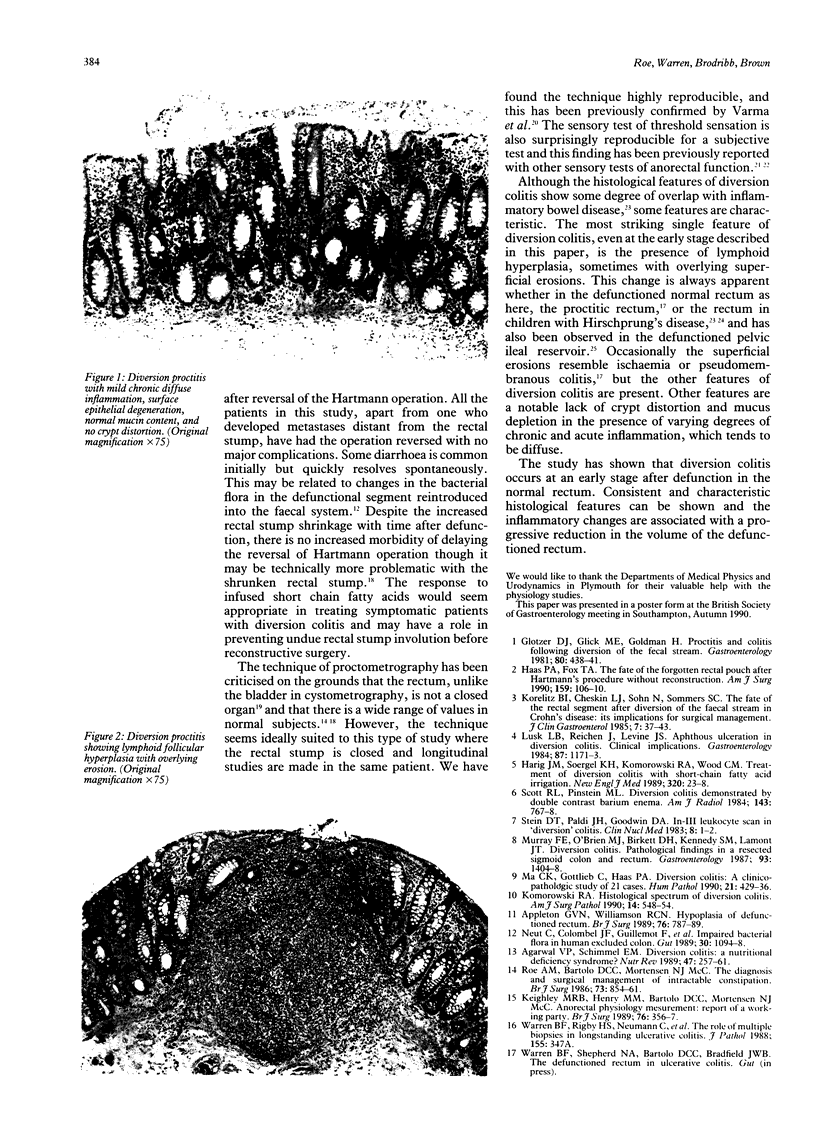
To measure the effects of defunction in the anorectum, 12 patients (seven men and five women aged 59 (44-81) years) were studied after the Hartmann operation. The operation was for septic complications of diverticular disease in nine and sigmoid carcinoma in three patients. Physiology studies were undertaken 1 and 3 months after surgery, and diversion colitis was assessed endoscopically and by mucosal biopsy at 3 months. There was no change in anal sphincter function by three months. Proctometrogram studies, however, showed an appreciable decrease in rectal volume in all cases, by a mean of 35% of the 1 month volume. The maximum tolerable volume at 1 month was 157 (111-210) ml and at 3 months 87 (71-145) ml; p < 0.01. There was no change in rectal sensation or compliance. Erythema and granularity without gross erosions or ulceration were found at endoscopy. Histology showed abnormalities in all cases by 3 months. The characteristic features were of a chronic inflammatory cell infiltrate with surface exudate, microscopic erosions, and lymphoid follicular hyperplasia. Crypt abscesses were not a feature at this stage and there was no distortion of crypt architecture. After defunction the previously normal rectum is affected by diversion colitis which, at 3 months, is mild but has characteristics that distinguish the changes from those of inflammatory bowel disease. It is associated with progressive rectal stump involution.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Agarwal V. P., Schimmel E. M. Diversion colitis: a nutritional deficiency syndrome? Nutr Rev. 1989 Sep;47(9):257–261. doi: 10.1111/j.1753-4887.1989.tb02857.x. [DOI] [PubMed] [Google Scholar]
- Appleton G. V., Williamson R. C. Hypoplasia of defunctioned rectum. Br J Surg. 1989 Aug;76(8):787–789. doi: 10.1002/bjs.1800760807. [DOI] [PubMed] [Google Scholar]
- Geraghty J. M., Talbot I. C. Diversion colitis: histological features in the colon and rectum after defunctioning colostomy. Gut. 1991 Sep;32(9):1020–1023. doi: 10.1136/gut.32.9.1020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glotzer D. J., Glick M. E., Goldman H. Proctitis and colitis following diversion of the fecal stream. Gastroenterology. 1981 Mar;80(3):438–441. [PubMed] [Google Scholar]
- Haas P. A., Fox T. A., Jr The fate of the forgotten rectal pouch after Hartmann's procedure without reconstruction. Am J Surg. 1990 Jan;159(1):106–111. doi: 10.1016/s0002-9610(05)80614-2. [DOI] [PubMed] [Google Scholar]
- Keighley M. R., Henry M. M., Bartolo D. C., Mortensen N. J. Anorectal physiology measurement: report of a working party. Br J Surg. 1989 Apr;76(4):356–357. doi: 10.1002/bjs.1800760414. [DOI] [PubMed] [Google Scholar]
- Komorowski R. A. Histologic spectrum of diversion colitis. Am J Surg Pathol. 1990 Jun;14(6):548–554. doi: 10.1097/00000478-199006000-00005. [DOI] [PubMed] [Google Scholar]
- Korelitz B. I., Cheskin L. J., Sohn N., Sommers S. C. The fate of the rectal segment after diversion of the fecal stream in Crohn's disease: its implications for surgical management. J Clin Gastroenterol. 1985 Feb;7(1):37–43. doi: 10.1097/00004836-198502000-00005. [DOI] [PubMed] [Google Scholar]
- Lusk L. B., Reichen J., Levine J. S. Aphthous ulceration in diversion colitis. Clinical implications. Gastroenterology. 1984 Nov;87(5):1171–1173. [PubMed] [Google Scholar]
- Ma C. K., Gottlieb C., Haas P. A. Diversion colitis: a clinicopathologic study of 21 cases. Hum Pathol. 1990 Apr;21(4):429–436. doi: 10.1016/0046-8177(90)90206-k. [DOI] [PubMed] [Google Scholar]
- Madoff R. D., Orrom W. J., Rothenberger D. A., Goldberg S. M. Rectal compliance: a critical reappraisal. Int J Colorectal Dis. 1990 Feb;5(1):37–40. doi: 10.1007/BF00496148. [DOI] [PubMed] [Google Scholar]
- Murray F. E., O'Brien M. J., Birkett D. H., Kennedy S. M., LaMont J. T. Diversion colitis. Pathologic findings in a resected sigmoid colon and rectum. Gastroenterology. 1987 Dec;93(6):1404–1408. [PubMed] [Google Scholar]
- Neut C., Colombel J. F., Guillemot F., Cortot A., Gower P., Quandalle P., Ribet M., Romond C., Paris J. C. Impaired bacterial flora in human excluded colon. Gut. 1989 Aug;30(8):1094–1098. doi: 10.1136/gut.30.8.1094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roe A. M., Bartolo D. C., Mortensen N. J. Diagnosis and surgical management of intractable constipation. Br J Surg. 1986 Oct;73(10):854–861. doi: 10.1002/bjs.1800731031. [DOI] [PubMed] [Google Scholar]
- Rogers J., Laurberg S., Misiewicz J. J., Henry M. M., Swash M. Anorectal physiology validated: a repeatability study of the motor and sensory tests of anorectal function. Br J Surg. 1989 Jun;76(6):607–609. doi: 10.1002/bjs.1800760628. [DOI] [PubMed] [Google Scholar]
- Scott R. L., Pinstein M. L. Diversion colitis demonstrated by double-contrast barium enema. AJR Am J Roentgenol. 1984 Oct;143(4):767–768. doi: 10.2214/ajr.143.4.767. [DOI] [PubMed] [Google Scholar]
- Stein D. T., Paldi J. H., Goodwin D. A. In-111 leukocyte scan in "diversion" colitis. Clin Nucl Med. 1983 Jan;8(1):1–2. doi: 10.1097/00003072-198301000-00001. [DOI] [PubMed] [Google Scholar]
- Varma J. S., Smith A. N. Reproducibility of the proctometrogram. Gut. 1986 Mar;27(3):288–292. doi: 10.1136/gut.27.3.288. [DOI] [PMC free article] [PubMed] [Google Scholar]