

Abstract
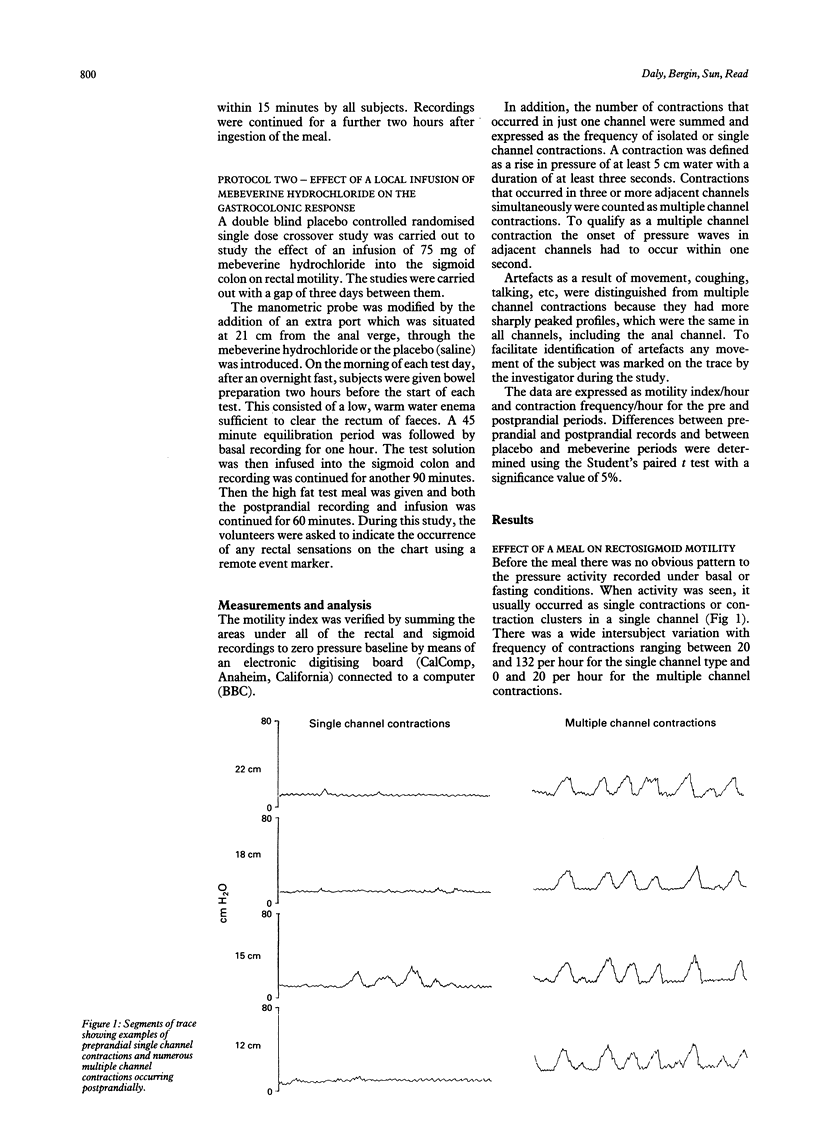
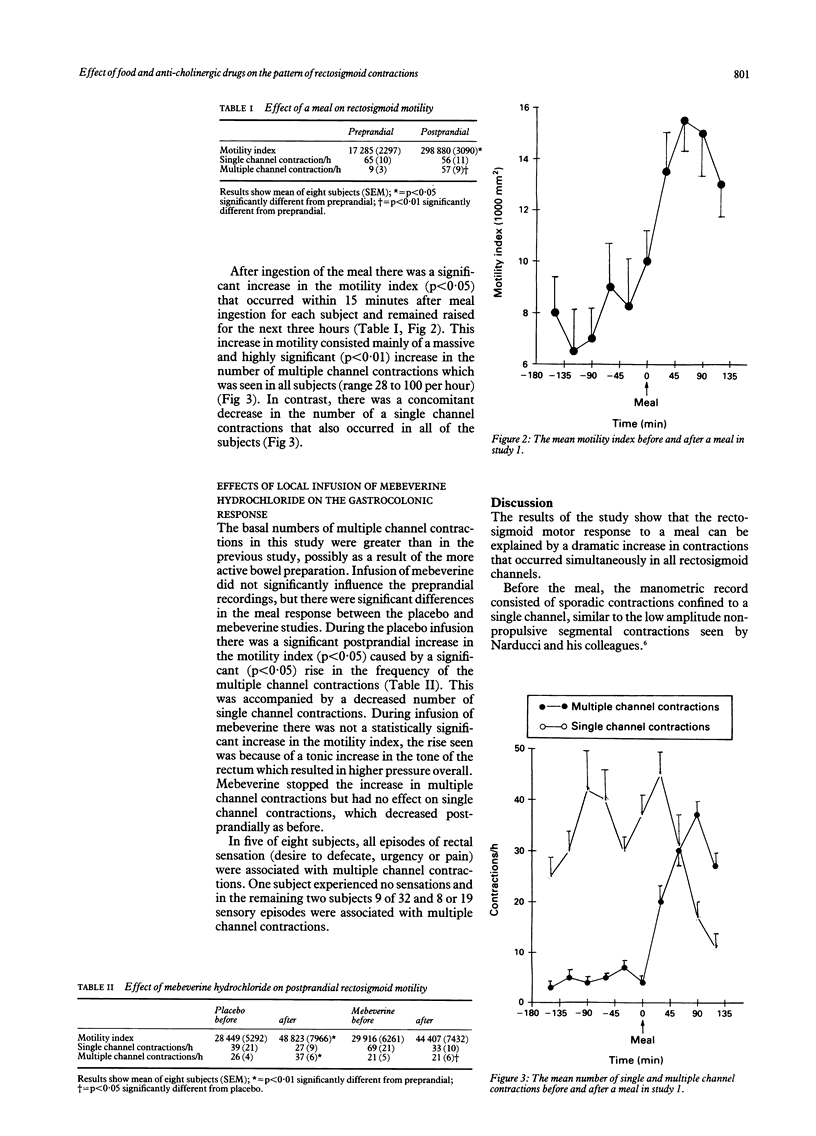
The colonic response to a meal is often used to test the effect of drugs on colonic motility, but this test is hindered by its inconsistency. This study has used multiple manometric sensors situated in the rectosigmoid region to investigate whether recording of the site and type of contraction offers a clear discrimination of the colonic response to a meal and the effect of drugs. Two studies were carried out on 16 healthy volunteers. Before the meal, rectosigmoid motility consisted mainly of isolated contractions occurring in a single manometric channel. The motility index increased in every subject after the meal (p < 0.05), but this increase entirely consisted of a massive increase in contractions occurring simultaneously in three or more manometric channels (multiple channel contractions), the number increasing from 9 per hour preprandially to 57 per hour (p < 0.01). There was a concomitant decrease in the number of the single channel contractions from 65 to 56 per hour. In a second study an infusion of an antispasmodic drug, mebeverine hydrochloride, into the sigmoid colon of healthy volunteers stopped the postprandial increase in the multiple channel contractions and prevented the significant rise in the motility index. The decrease in single channel contractions was unaffected. These results show that the colonic response to a meal consists of a change in the pattern of rectosigmoid contractions and suggest that multiple channel contractions may be a more sensitive indicator of the effect of a meal on the rectosigmoid colon than the motility index.
Full text
PDF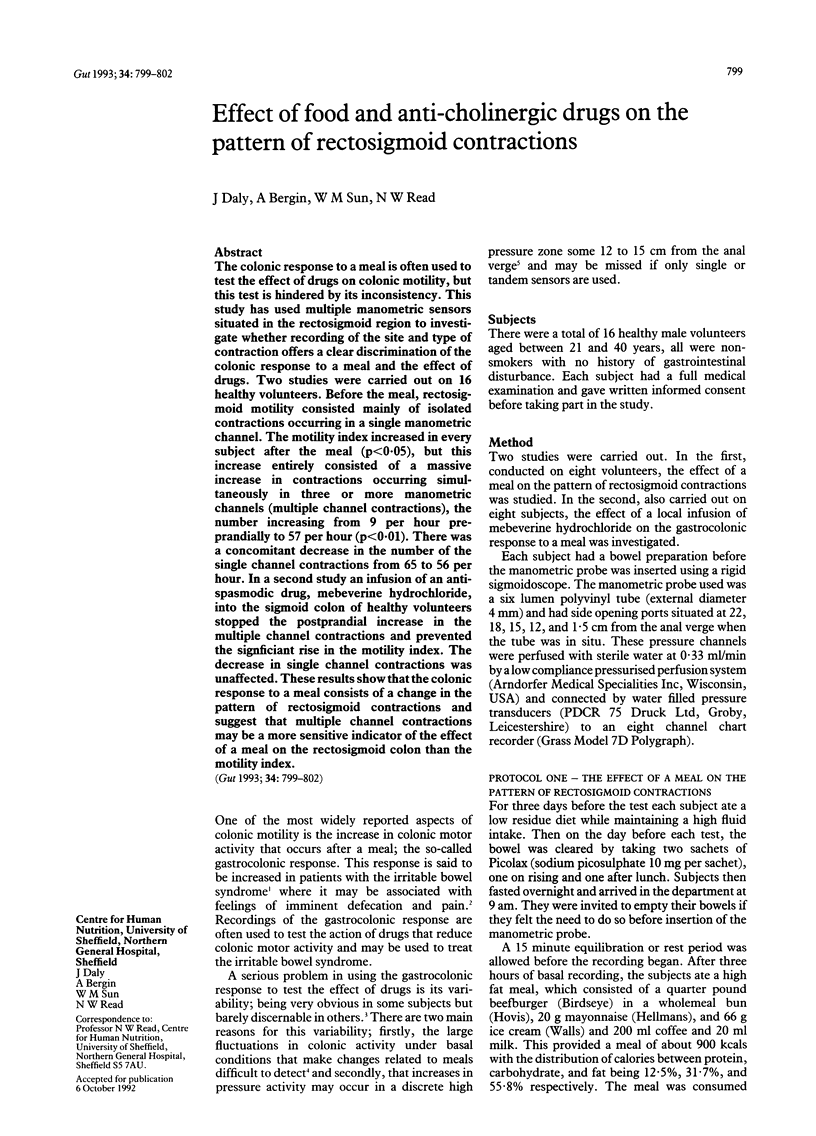

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Chowdhury A. R., Dinoso V. P., Lorber S. H. Characterization of a hyperactive segment at the rectosigmoid junction. Gastroenterology. 1976 Oct;71(4):584–588. [PubMed] [Google Scholar]
- Dinoso V. P., Jr, Murthy S. N., Goldstein J., Rosner B. Basal motor activity of the distal colon: a reappraisal. Gastroenterology. 1983 Sep;85(3):637–642. [PubMed] [Google Scholar]
- Kock N. G., Hultén L., Leandoer L. A study of the motility in different parts of the human colon. Resting activity, response to feeding and to prostigmine. Scand J Gastroenterol. 1968;3(2):163–169. doi: 10.3109/00365526809180117. [DOI] [PubMed] [Google Scholar]
- Loening-Baucke V., Anuras S. Effects of a meal on the motility of the sigmoid colon and rectum in healthy adults. Am J Gastroenterol. 1983 Jul;78(7):393–397. [PubMed] [Google Scholar]
- Moreno-Osset E., Bazzocchi G., Lo S., Trombley B., Ristow E., Reddy S. N., Villanueva-Meyer J., Fain J. W., Jing J., Mena I. Association between postprandial changes in colonic intraluminal pressure and transit. Gastroenterology. 1989 May;96(5 Pt 1):1265–1273. doi: 10.1016/s0016-5085(89)80013-7. [DOI] [PubMed] [Google Scholar]
- Narducci F., Bassotti G., Gaburri M., Morelli A. Twenty four hour manometric recording of colonic motor activity in healthy man. Gut. 1987 Jan;28(1):17–25. doi: 10.1136/gut.28.1.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sun W. M., Edwards C. A., Prior A., Rao S. S., Read N. W. Effect of oral nicardipine on anorectal function in normal human volunteers and patients with irritable bowel syndrome. Dig Dis Sci. 1990 Jul;35(7):885–890. doi: 10.1007/BF01536803. [DOI] [PubMed] [Google Scholar]
- Tomlin J., Brown S. R., Cann P. A., Read N. W. Is rectosigmoid response to food modulated by proximal colon stimulation? Dig Dis Sci. 1991 Oct;36(10):1481–1485. doi: 10.1007/BF01296819. [DOI] [PubMed] [Google Scholar]