

Abstract
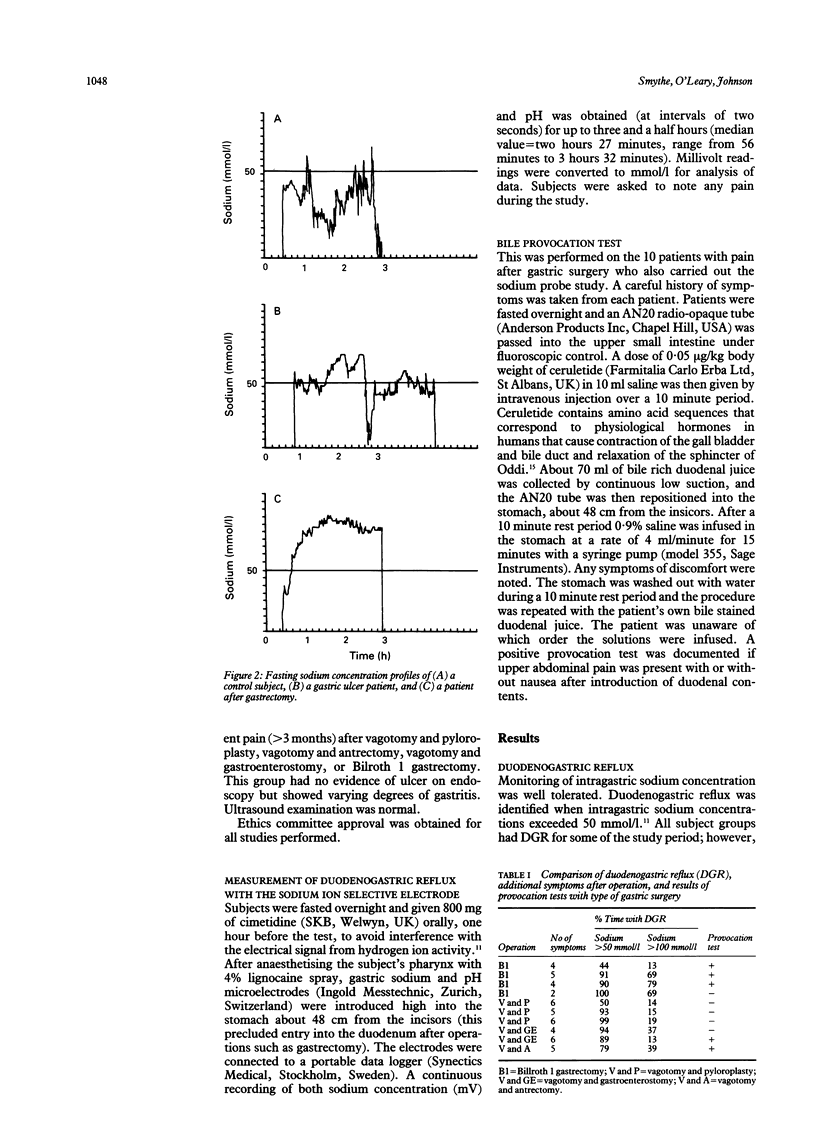
Duodenogastric reflux (DGR) was investigated with a sodium ion selective electrode in 10 normal controls, 10 patients with persistent pain after gastric surgery, and five patients with gastric ulcer. During an average study time of two and a half hours, normal controls had reflux for 12% of the study, whereas patients after gastric surgery had reflux for 91% of the study time (p < 0.0002). Patients with a gastric ulcer had reflux on average for 67% of the study (p < 0.001). The patients who had had gastric surgery had several symptoms, but there was no association between the number or nature of symptoms and the severity of DGR as determined by the sodium electrode. Patients with positive bile provocation tests did not show any significant difference in the duration of reflux compared with those with a negative provocation test (79% and 87%). There was also no relation between the results of the provocation test and the number and nature of symptoms. Continuous monitoring of intragastric sodium ions with a selective electrode is a practical means of assessing DGR. Results suggest that symptoms due to DGR may be related to the sensitivity of the gastric lining as well as the amounts of duodenal contents flowing back into the stomach.
Full text
PDF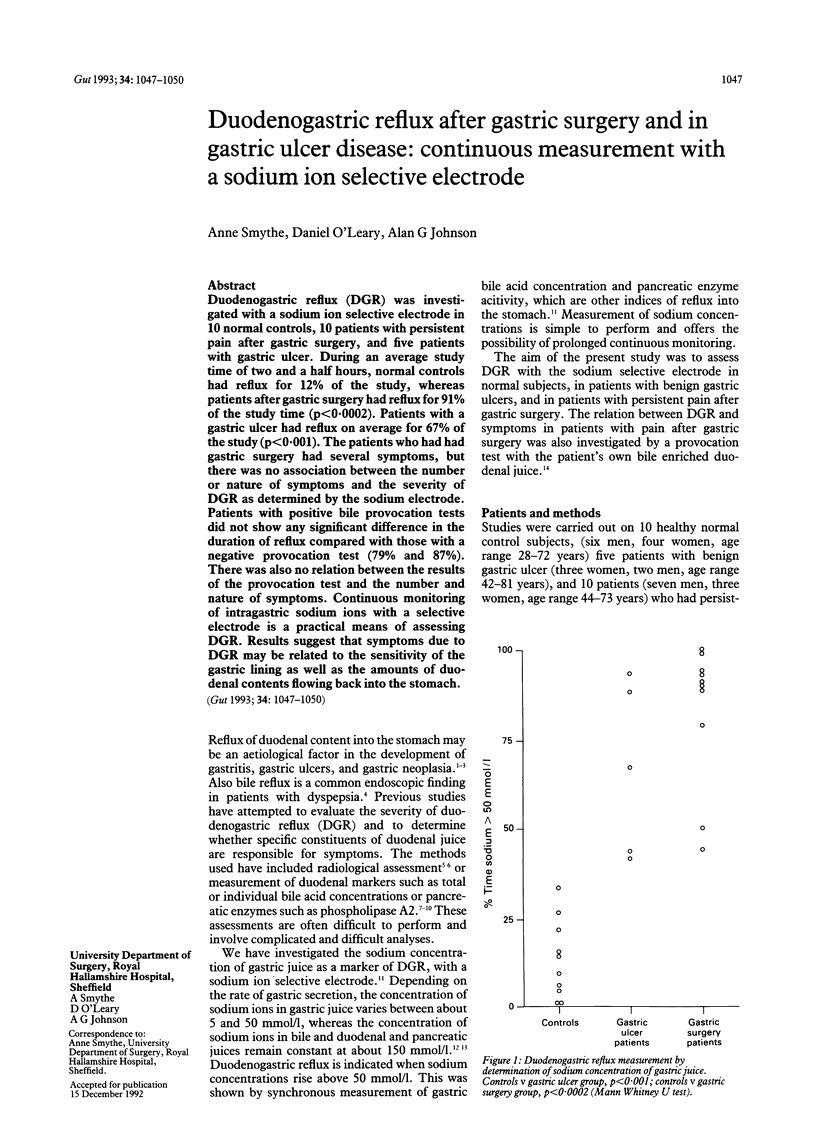
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bertaccini G., Braibanti T., Uva F. Cholecystokinetic activity of the new peptide caerulein in man. Gastroenterology. 1969 May;56(5):862–867. [PubMed] [Google Scholar]
- Capper W. M., Airth G. R., Kilby J. O. A test for pyloric regurgitation. Lancet. 1966 Sep 17;2(7464):621–623. doi: 10.1016/s0140-6736(66)91930-1. [DOI] [PubMed] [Google Scholar]
- Eyre-Brook I. A., Holroyd A. M., Johnson A. G. Is bile reflux at endoscopy a significant finding? Scand J Gastroenterol Suppl. 1984;92:203–205. [PubMed] [Google Scholar]
- Eyre-Brook I. A., Smythe A., Bird N. C., Mangnall Y., Johnson A. G. Relative contribution of bile and pancreatic juice duodenogastric reflux in gastric ulcer disease and cholelithiasis. Br J Surg. 1987 Aug;74(8):721–725. doi: 10.1002/bjs.1800740823. [DOI] [PubMed] [Google Scholar]
- Fiddian-Green R. G., Russell R. C., Hobsley M. Secretin-induced pyloric reflux: verification of the mathematical formula for eliminating reflux in gastric aspirate. Br J Surg. 1972 Nov;59(11):903–903. [PubMed] [Google Scholar]
- Frizis H. I., Whitfield P. F., Hobsley M. Maximal gastric secretion and duodenogastric reflux in patients with gastric or duodenal ulcer and in control subjects. Br J Surg. 1987 Feb;74(2):106–109. doi: 10.1002/bjs.1800740211. [DOI] [PubMed] [Google Scholar]
- Gadacz T. R., Zuidema G. D. Bile acid composition in patients with and without symptoms of postoperative refulx gastritis. Am J Surg. 1978 Jan;135(1):48–52. doi: 10.1016/0002-9610(78)90008-9. [DOI] [PubMed] [Google Scholar]
- Hoare A. M., McLeish A., Thompson H., Alexander-Williams J. Selection of patients for bile diversion surgery: use of bile acid measurement in fasting gastric aspirates. Gut. 1978 Mar;19(3):163–165. doi: 10.1136/gut.19.3.163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Houghton P. W., Mortensen N. J., Thomas W. E., Cooper M. J., Morgan A. P., Burton P. Intragastric bile acids and histological changes in gastric mucosa. Br J Surg. 1986 May;73(5):354–356. doi: 10.1002/bjs.1800730509. [DOI] [PubMed] [Google Scholar]
- Johnson A. G. The effects of cisapride on antroduodenal co-ordination and gastric emptying. Scand J Gastroenterol Suppl. 1989;165:36–43. doi: 10.3109/00365528909091229. [DOI] [PubMed] [Google Scholar]
- Keane F. B., Dimagno E. P., Malagelada J. R. Duodenogastric reflux in humans: its relationship to fasting antroduodenal motility and gastric, pancreatic, and biliary secretion. Gastroenterology. 1981 Oct;81(4):726–731. [PubMed] [Google Scholar]
- Meshkinpour H., Marks J. W., Schoenfield L. J., Bonnoris G. G., Carter S. Reflux gastritis syndrome: mechanism of symptoms. Gastroenterology. 1980 Dec;79(6):1283–1287. [PubMed] [Google Scholar]
- Meshkinpour H., Marks J. W., Schoenfield L. J., Bonnoris G. G., Carter S. Reflux gastritis syndrome: mechanism of symptoms. Gastroenterology. 1980 Dec;79(6):1283–1287. [PubMed] [Google Scholar]
- Müller-Lissner S. A., Fimmel C. J., Sonnenberg A., Will N., Müller-Duysing W., Heinzel F., Müller R., Blum A. L. Novel approach to quantify duodenogastric reflux in healthy volunteers and in patients with type I gastric ulcer. Gut. 1983 Jun;24(6):510–518. doi: 10.1136/gut.24.6.510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smythe A., Bird N. C., Johnson A. G. Continuous monitoring of sodium ion concentration in the human stomach--a new technique for the detection of duodenogastric reflux. Digestion. 1992;52(1):20–25. doi: 10.1159/000200934. [DOI] [PubMed] [Google Scholar]