

Abstract
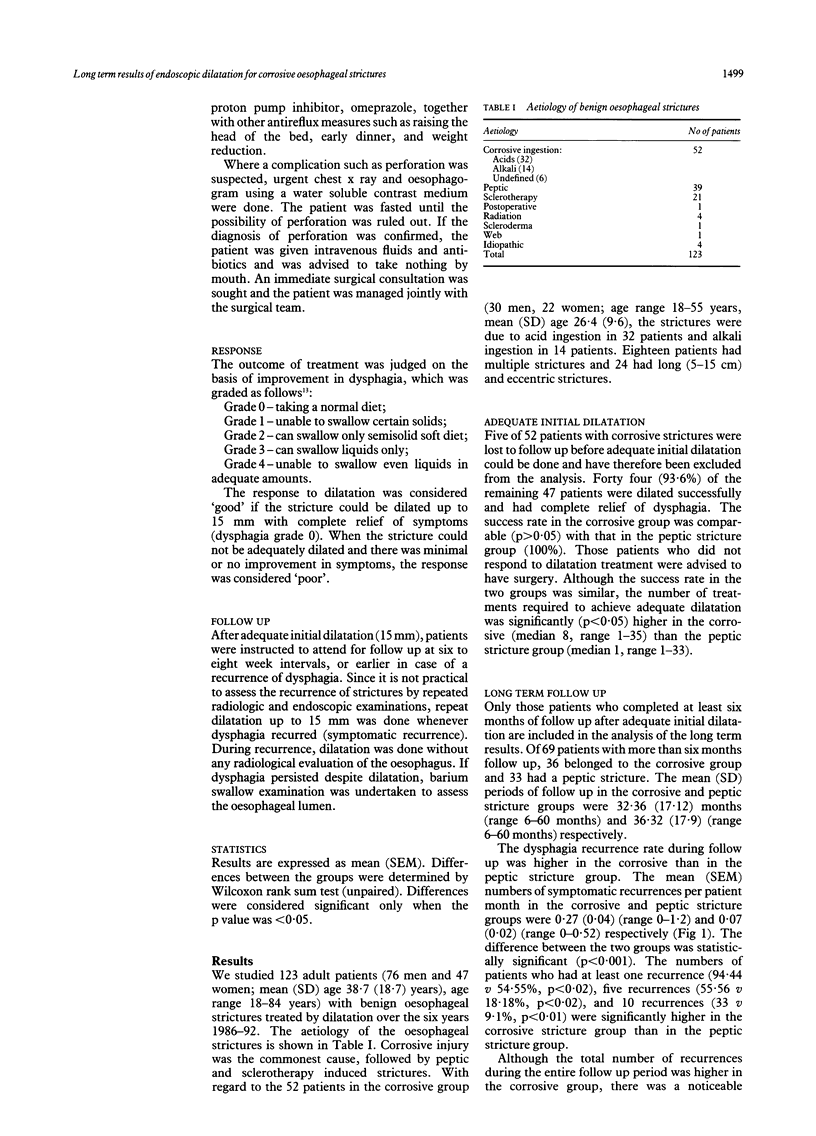
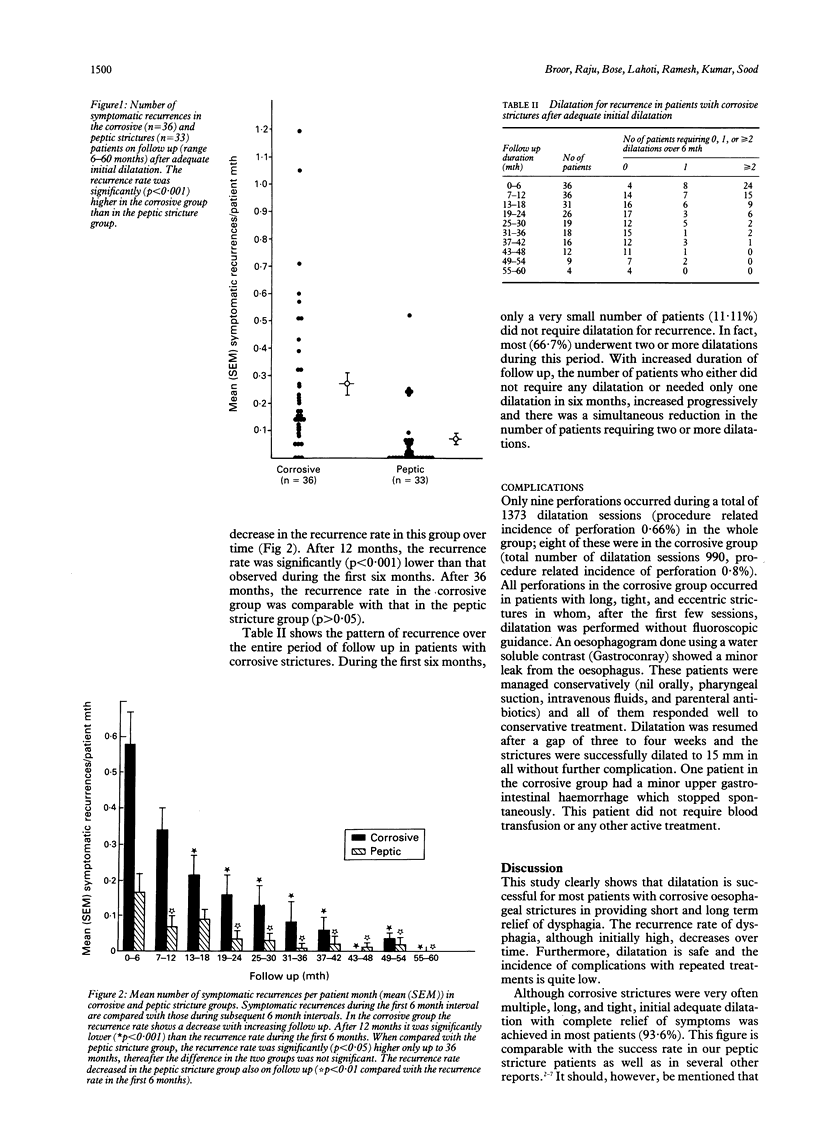
Although dilatation is the treatment of choice for most patients with benign oesophageal strictures, there is little information on its efficacy and safety in corrosive oesophageal strictures. Of 123 adults with benign oesophageal strictures treated by endoscopic dilatation, 52 (42.3%) had strictures after corrosive ingestion and 39 (31.7%) had peptic strictures. Treatment was considered adequate if the oesophageal lumen could be dilated to 15 mm and there was complete relief of dysphagia. If dysphagia recurred after adequate initial dilatation, the stricture was dilated again up to 15 mm. Initial dilatation was adequate in 93.6% of patients with corrosive strictures and this success rate was comparable with that of the peptic stricture group (100%, p > 0.05). Long term success after adequate initial dilatation was studied in 36 patients with corrosive strictures (mean follow up 32.36 (17.12) months, range 6-60) and 33 patients with peptic strictures (mean follow up 36.32 (17.9) months, range 6-60). The mean (SEM) number of symptomatic recurrences per patient month during the total follow up period in the corrosive group was significantly higher than that in the peptic group (0.27 (0.04) v 0.07 (0.02), p < 0.001). The recurrence rate in the corrosive group, however, decreased over time, and after 12 months it was significantly (p < 0.001) lower than the recurrence rate in the first six months. After 36 months, the difference in the recurrence rate in the two groups was not significant (p > 0.05). Only nine oesophageal perforations occurred during a total of 1373 dilatation treatments (procedure related incidence 0.66%), and eight of these were in the corrosive stricture group. These patients were managed conservatively and subsequently strictures were dilated adequately in all. Endoscopic dilatation is safe and effective for short and long term relief of dysphagia in patients with corrosive oesophageal strictures.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Atkinson M., Ferguson R., Ogilvie A. L. Management of malignant dysphagia by intubation at endoscopy. J R Soc Med. 1979 Dec;72(12):894–897. doi: 10.1177/014107687907201206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Broor S. L., Kumar A., Chari S. T., Singal A., Misra S. P., Kumar N., Sarin S. K., Vij J. C. Corrosive oesophageal strictures following acid ingestion: clinical profile and results of endoscopic dilatation. J Gastroenterol Hepatol. 1989 Jan-Feb;4(1):55–61. doi: 10.1111/j.1440-1746.1989.tb00807.x. [DOI] [PubMed] [Google Scholar]
- Cox J. G., Winter R. K., Maslin S. C., Jones R., Buckton G. K., Hoare R. C., Sutton D. R., Bennett J. R. Balloon or bougie for dilatation of benign oesophageal stricture? An interim report of a randomised controlled trial. Gut. 1988 Dec;29(12):1741–1747. doi: 10.1136/gut.29.12.1741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dilawari J. B., Singh S., Rao P. N., Anand B. S. Corrosive acid ingestion in man - a clinical and endoscopic study. Gut. 1984 Feb;25(2):183–187. doi: 10.1136/gut.25.2.183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- FATTI L., MARCHAND P., CRAWSHAW G. R. The treatment of caustic strictures of the esophagus. Surg Gynecol Obstet. 1956 Feb;102(2):195–206. [PubMed] [Google Scholar]
- Gerzic Z. B., Knezevic J. B., Milicevic M. N., Jovanovic B. K. Esophagocoloplasty in the management of postcorrosive strictures of the esophagus. Ann Surg. 1990 Mar;211(3):329–336. doi: 10.1097/00000658-199003000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glick M. E. Clinical course of esophageal stricture managed by bougienage. Dig Dis Sci. 1982 Oct;27(10):884–888. doi: 10.1007/BF01316571. [DOI] [PubMed] [Google Scholar]
- Ogilvie A. L., Ferguson R., Atkinson M. Outlook with conservative treatment of peptic oesophageal stricture. Gut. 1980 Jan;21(1):23–25. doi: 10.1136/gut.21.1.23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- PETROV B. A. Retrosternal artificial esophagus from jejunum and colon. Surgery. 1959 Jun;45(6):890–898. [PubMed] [Google Scholar]
- Patterson D. J., Graham D. Y., Smith J. L., Schwartz J. T., Alpert E., Lanza F. L., Cain G. D. Natural history of benign esophageal stricture treated by dilatation. Gastroenterology. 1983 Aug;85(2):346–350. [PubMed] [Google Scholar]
- Rago E., Boesby S., Spencer J. Results of Eder-Puestow dilatation in the management of esophageal peptic strictures. Am J Gastroenterol. 1983 Jan;78(1):6–8. [PubMed] [Google Scholar]
- Ti T. K., Sivaloganathan V. Oesophageal resection with cervical oesophagogastrostomy for corrosive oesophageal stricture. Br J Surg. 1978 Apr;65(4):256–258. doi: 10.1002/bjs.1800650412. [DOI] [PubMed] [Google Scholar]
- Wesdorp I. C., Bartelsman J. F., den Hartog Jager F. C., Huibregtse K., Tytgat G. N. Results of conservative treatment of benign esophageal strictures: a follow-up study in 100 patients. Gastroenterology. 1982 Mar;82(3):487–493. [PubMed] [Google Scholar]
- Williamson R. C. The management of peptic oesophageal stricture. Br J Surg. 1975 Jun;62(6):448–454. doi: 10.1002/bjs.1800620607. [DOI] [PubMed] [Google Scholar]
- Zargar S. A., Kochhar R., Nagi B., Mehta S., Mehta S. K. Ingestion of corrosive acids. Spectrum of injury to upper gastrointestinal tract and natural history. Gastroenterology. 1989 Sep;97(3):702–707. [PubMed] [Google Scholar]