

Abstract
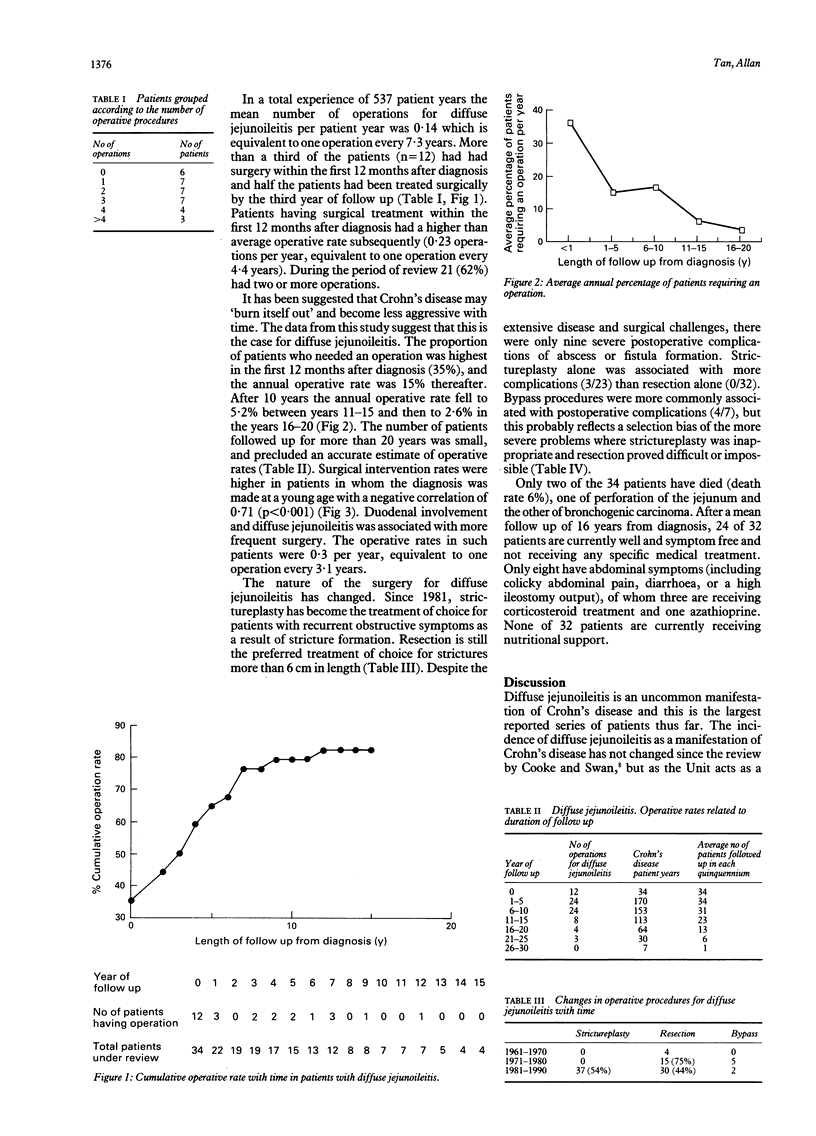
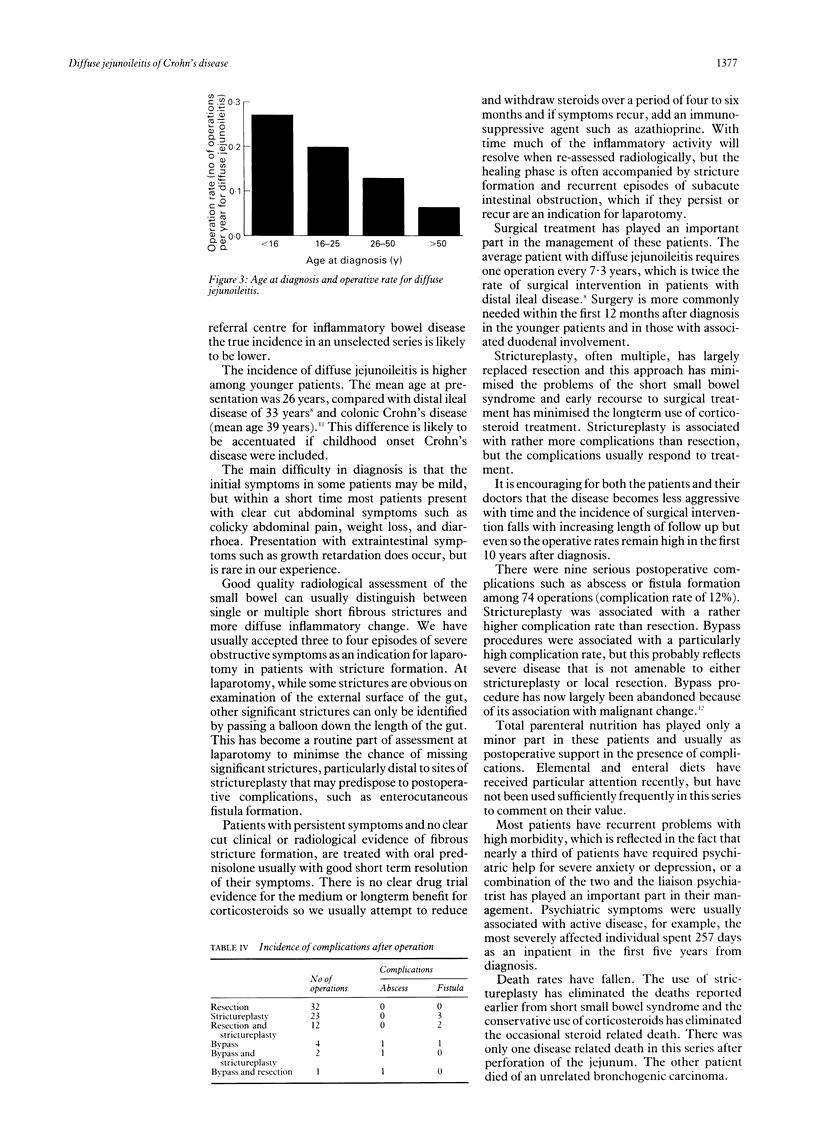
Diffuse jejunoileitis is an uncommon, but important manifestation of Crohn's disease because of the associated high morbidity and challenges in medical management. Despite this there have been no studies of prognosis or management of diffuse jejunoileitis for nearly 20 years. This study analysed the outcome among 34 patients (20 women and 14 men) with diffuse jejunoileitis diagnosed between 1960 and 1991 including clinical features, medical and surgical management, death rates, current status, and prognosis. Diffuse jejunoileitis presents in younger patients (mean age at diagnosis 26.4 years) than those with distal ileal Crohn's disease (mean age at diagnosis 33.3 years). Nearly all presented with clear cut abdominal symptoms including a combination of colicky abdominal pain (91%), weight loss (62%), and diarrhoea (53%). Most patients had severe symptoms reflected by the fact that 77% had been treated with corticosteroids for periods of more than six months at some stage during their follow up. The mean follow up from diagnosis was 16 years. Twenty eight patients (82%) had at least one operation for diffuse jejunoileitis and two thirds of the patients (n = 21) required two or more operations. The frequency of surgical intervention was particularly high in the younger patients (r = 0.71, p < 0.001). The proportion of patients requiring surgery was highest in the first year after diagnosis. The annual operative rate was 15% for the first 10 years and then it fell to 5.2% in years 11-15, and 2.6% in years 16-20. The data suggest that the disease does burn itself out over time. The increasing use of strictureplasty for short strictures and the minimal use of resection has eliminated problems associated with the short small bowel syndrome. The longterm prognosis of this patients is good. Only two patients died (one of perforation of the jejunum and another of an unrelated bronchogenic carcinoma). After a mean interval from diagnosis of 16 year, 24 of 32 living patients are well and symptom free. Only eight have abdominal symptoms of whom three are receiving corticosteroid treatment and one azathioprine. The combination of anti-inflammatory drugs with the relief of recurrent obstructive symptoms by strictureplasty can together produce a good longterm prognosis in most patients with diffuse jejunoileitis.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Andrews H. A., Keighley M. R., Alexander-Williams J., Allan R. N. Strategy for management of distal ileal Crohn's disease. Br J Surg. 1991 Jun;78(6):679–682. doi: 10.1002/bjs.1800780614. [DOI] [PubMed] [Google Scholar]
- Andrews H. A., Lewis P., Allan R. N. Prognosis after surgery for colonic Crohn's disease. Br J Surg. 1989 Nov;76(11):1184–1190. doi: 10.1002/bjs.1800761123. [DOI] [PubMed] [Google Scholar]
- Cooke W. T., Swan C. H. Diffuse jejuno-ileitis of Crohn's disease. Q J Med. 1974 Oct;43(172):583–601. [PubMed] [Google Scholar]
- Crohn B. B., Yunich A. M. ILEOJEJUNITIS. Ann Surg. 1941 Mar;113(3):371–380. doi: 10.1097/00000658-194103000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dehn T. C., Kettlewell M. G., Mortensen N. J., Lee E. C., Jewell D. P. Ten-year experience of strictureplasty for obstructive Crohn's disease. Br J Surg. 1989 Apr;76(4):339–341. doi: 10.1002/bjs.1800760407. [DOI] [PubMed] [Google Scholar]
- Greenstein A. J., Sachar D., Pucillo A., Kreel I., Geller S., Janowitz H. D., Aufses A., Jr Cancer in Crohn's disease after diversionary surgery. A report of seven carcinomas occurring in excluded bowel. Am J Surg. 1978 Jan;135(1):86–90. doi: 10.1016/0002-9610(78)90015-6. [DOI] [PubMed] [Google Scholar]
- Higgens C. S., Allan R. N. Crohn's disease of the distal ileum. Gut. 1980 Nov;21(11):933–940. doi: 10.1136/gut.21.11.933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones J. H., Lennard-Jones J. E. Corticosteroids and corticotrophin in the treatment of Crohn's disease. Gut. 1966 Apr;7(2):181–187. doi: 10.1136/gut.7.2.181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sayfan J., Wilson D. A., Allan A., Andrews H., Alexander-Williams J. Recurrence after strictureplasty or resection for Crohn's disease. Br J Surg. 1989 Apr;76(4):335–338. doi: 10.1002/bjs.1800760406. [DOI] [PubMed] [Google Scholar]
- Somerville K. W., Logan R. F., Edmond M., Langman M. J. Smoking and Crohn's disease. Br Med J (Clin Res Ed) 1984 Oct 13;289(6450):954–956. doi: 10.1136/bmj.289.6450.954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- VAN PATTER W. N., BARGEN J. A., DOCKERTY M. B., FELDMAN W. H., MAYO C. W., WAUGH J. M. Regional enteritis. Gastroenterology. 1954 Mar;26(3):347–450. [PubMed] [Google Scholar]