

Abstract
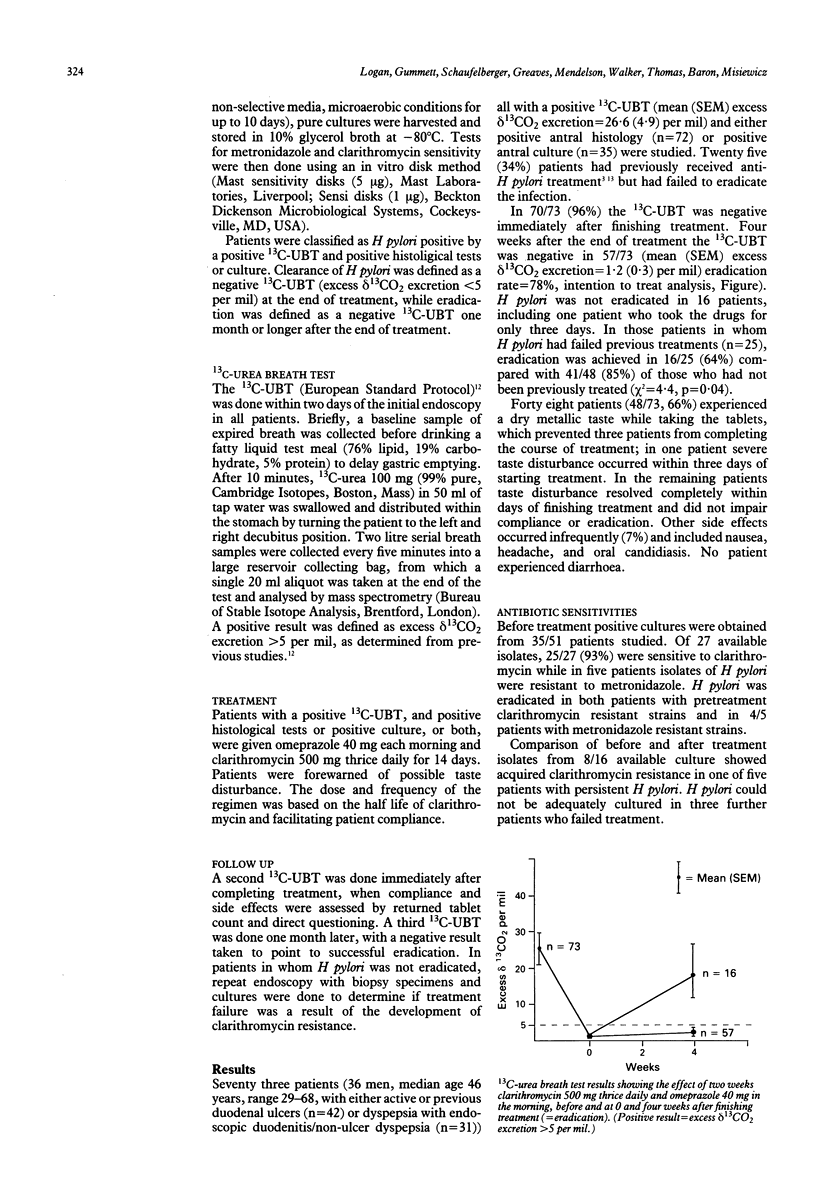
Clarithromycin, a new and well tolerated, acid stable macrolide antibiotic, has a similar antimicrobial spectrum to erythromycin but a better in vitro MIC90 (0.03 microgram/l-1) against Helicobacter pylori (H pylori). This study aimed at determining the eradication rate using clarithromycin 500 mg thrice daily and omeprazole 40 mg daily for two weeks. Patients were given an endoscopy and H pylori status assessed by antral culture (microaerobic conditions, for up to 10 days), antral and corpus histology tests (haematoxylin and eosin/Gimenez stains), and 13C-urea breath test (13C-UBT, European standard protocol, positive result = excess delta 13CO2 excretion > 5 per mil). Compliance was assessed by returned tablet counts. H pylori clearance at the end of treatment and eradication four weeks after finishing treatment were assessed by the 13C-UBT. Seventy three patients (54 men, median age 45 years) with duodenal ulcers (n = 42) or duodenitis/non-ulcer dyspepsia (n = 31) all with a positive 13C-UBT (mean (SEM) excess delta-13CO2 excretion = 26.6 (4.9) per mil) and either positive antral histology (n = 72) or positive antral culture (n = 35) were studied. Before treatment 2/27 (7%) isolates of H pylori were resistant to clarithromycin and five isolates were resistant to metronidazole. In 70/73 (96%) the 13C-UBT was negative immediately after finishing treatment. Four weeks later the 13C-UBT was negative in 57/73 (mean (SEM) excess delta 13CO2 excretion = 1.2 (0.3) per mil, eradication rate = 78%). Forty eight (66%) patients experienced a metallic taste while taking the tablets. Although four (5%) patients, however, could not complete the course of treatment, in only one of these four was H pylori not eradicated. These results show that duel therapy with clarithromycin and omeprazole is well tolerated. With an eradication rate of 78% it is an effective treatment for metronidazole resistant H pylori and may be an alternative to standard triple therapy.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cleaning and disinfection of equipment for gastrointestinal flexible endoscopy: interim recommendations of a Working Party of the British Society of Gastroenterology. Gut. 1988 Aug;29(8):1134–1151. doi: 10.1136/gut.29.8.1134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daw M. A., Deegan P., Leen E., O'Moráin C. Short report: the effect of omeprazole on Helicobacter pylori and associated gastritis. Aliment Pharmacol Ther. 1991 Aug;5(4):435–439. doi: 10.1111/j.1365-2036.1991.tb00047.x. [DOI] [PubMed] [Google Scholar]
- Glupczynski Y., Burette A., De Koster E., Nyst J. F., Deltenre M., Cadranel S., Bourdeaux L., De Vos D. Metronidazole resistance in Helicobacter pylori. Lancet. 1990 Apr 21;335(8695):976–977. doi: 10.1016/0140-6736(90)91043-a. [DOI] [PubMed] [Google Scholar]
- Graham D. Y., Lew G. M., Malaty H. M., Evans D. G., Evans D. J., Jr, Klein P. D., Alpert L. C., Genta R. M. Factors influencing the eradication of Helicobacter pylori with triple therapy. Gastroenterology. 1992 Feb;102(2):493–496. doi: 10.1016/0016-5085(92)90095-g. [DOI] [PubMed] [Google Scholar]
- Graham D. Y., Opekun A. R., Klein P. D. Clarithromycin for the eradication of Helicobacter pylori. J Clin Gastroenterol. 1993 Jun;16(4):292–294. doi: 10.1097/00004836-199306000-00004. [DOI] [PubMed] [Google Scholar]
- Hui W. M., Lam S. K., Ho J., Lai C. L., Lok A. S., Ng M. M., Lau W. Y., Branicki F. J. Effect of omeprazole on duodenal ulcer-associated antral gastritis and Helicobacter pylori. Dig Dis Sci. 1991 May;36(5):577–582. doi: 10.1007/BF01297022. [DOI] [PubMed] [Google Scholar]
- Logan R. P., Gummett P. A., Hegarty B. T., Walker M. M., Baron J. H., Misiewicz J. J. Clarithromycin and omeprazole for Helicobacter pylori. Lancet. 1992 Jul 25;340(8813):239–239. doi: 10.1016/0140-6736(92)90502-t. [DOI] [PubMed] [Google Scholar]
- Logan R. P., Gummett P. A., Misiewicz J. J., Karim Q. N., Walker M. M., Baron J. H. One week eradication regimen for Helicobacter pylori. Lancet. 1991 Nov 16;338(8777):1249–1252. doi: 10.1016/0140-6736(91)92111-e. [DOI] [PubMed] [Google Scholar]
- Logan R. P., Gummett P. A., Misiewicz J. J., Karim Q. N., Walker M. M., Baron J. H. Two-week eradication regimen for metronidazole-resistant Helicobacter pylori. Aliment Pharmacol Ther. 1993 Apr;7(2):149–153. doi: 10.1111/j.1365-2036.1993.tb00083.x. [DOI] [PubMed] [Google Scholar]
- Marshall B. J., Goodwin C. S., Warren J. R., Murray R., Blincow E. D., Blackbourn S. J., Phillips M., Waters T. E., Sanderson C. R. Prospective double-blind trial of duodenal ulcer relapse after eradication of Campylobacter pylori. Lancet. 1988 Dec 24;2(8626-8627):1437–1442. doi: 10.1016/s0140-6736(88)90929-4. [DOI] [PubMed] [Google Scholar]
- Rasheed K., Coughlan G., O'Donnell B. Congenital diaphragmatic hernia in the newborn. Outcome in 59 consecutive cases over a ten year period (1980-1989). Ir J Med Sci. 1992 Jan;161(1):16–17. doi: 10.1007/BF02984671. [DOI] [PubMed] [Google Scholar]
- Rauws E. A., Tytgat G. N. Cure of duodenal ulcer associated with eradication of Helicobacter pylori. Lancet. 1990 May 26;335(8700):1233–1235. doi: 10.1016/0140-6736(90)91301-p. [DOI] [PubMed] [Google Scholar]
- Stolte M., Bethke B. Elimination of Helicobacter pylori under treatment with omeprazole. Z Gastroenterol. 1990 Jun;28(6):271–274. [PubMed] [Google Scholar]
- Westblom T. U., Duriex D. E. Enhancement of antibiotic concentrations in gastric mucosa by H2-receptor antagonist. Implications for treatment of Helicobacter pylori infections. Dig Dis Sci. 1991 Jan;36(1):25–28. doi: 10.1007/BF01300082. [DOI] [PubMed] [Google Scholar]