

Abstract
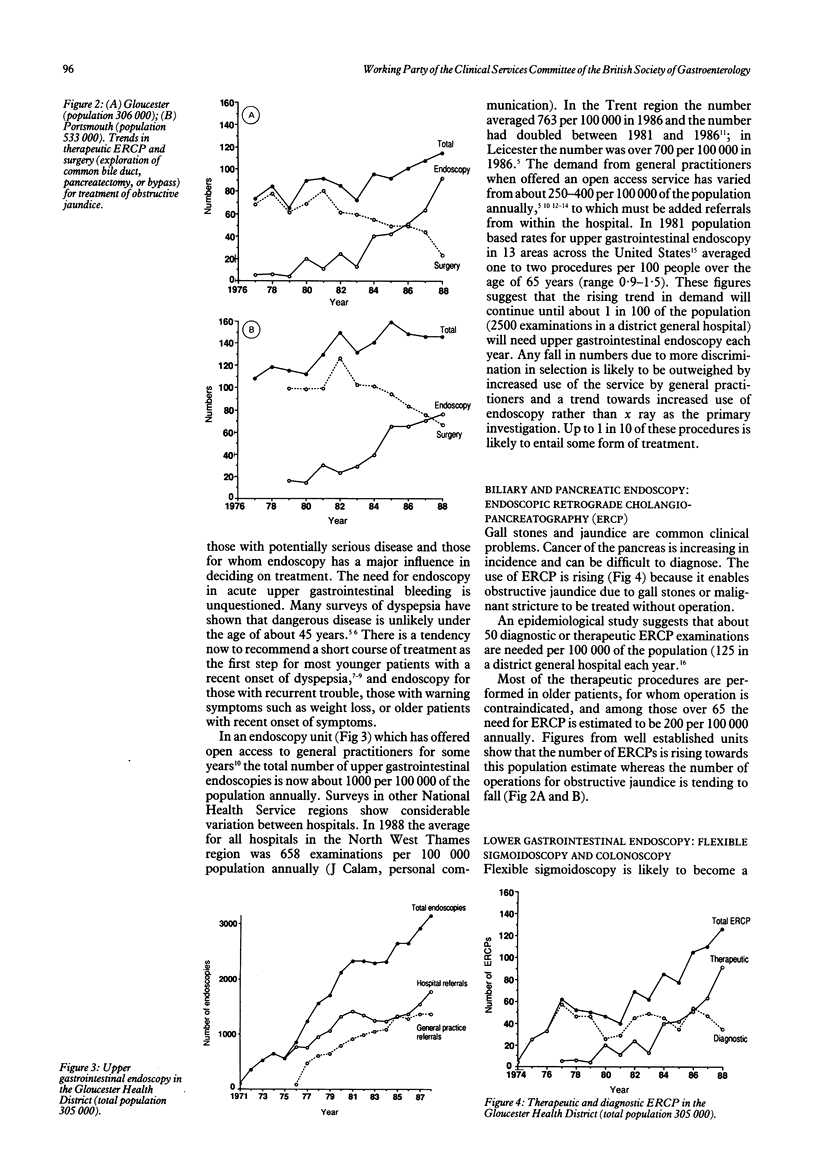
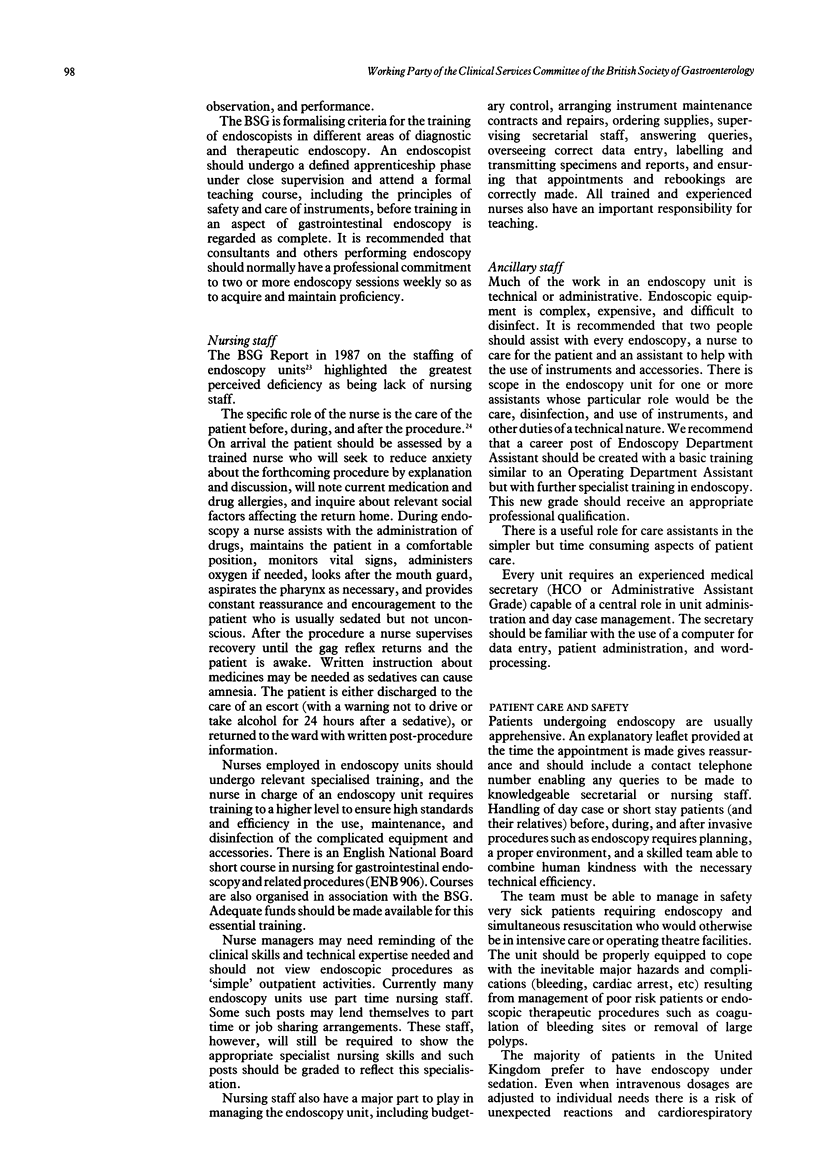
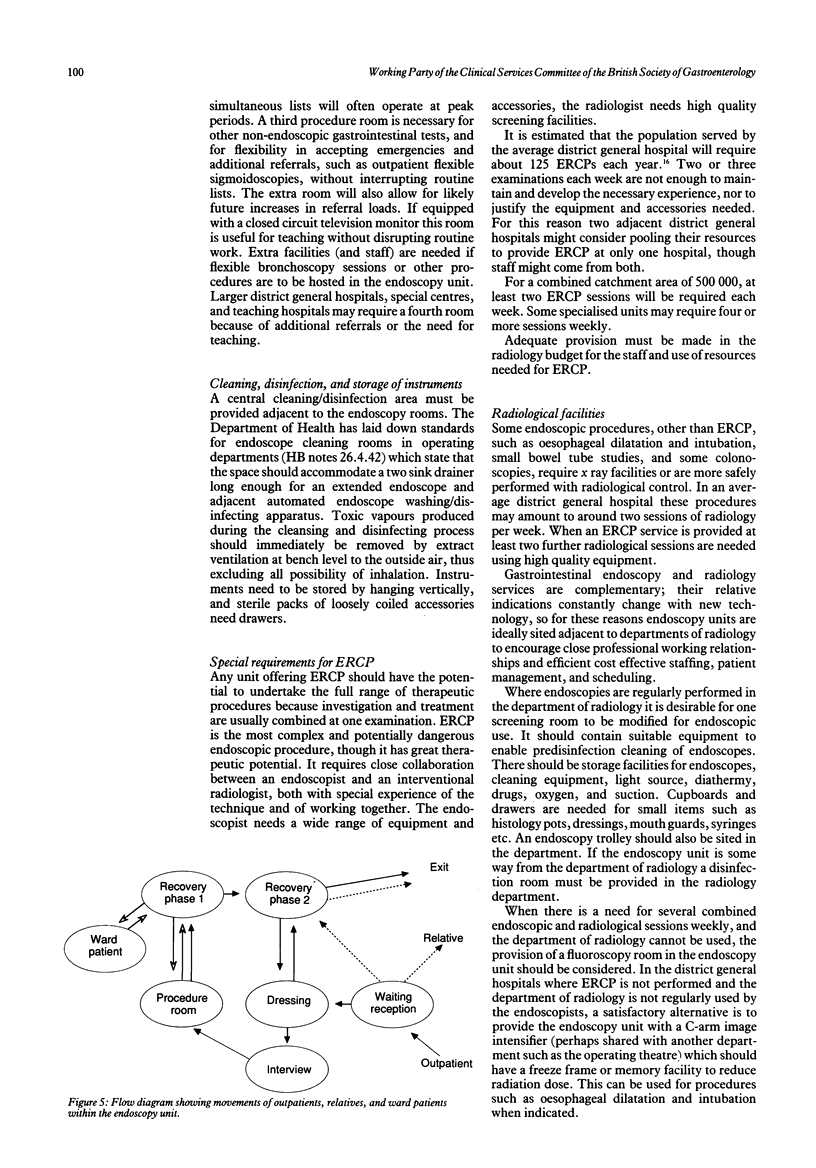
(1) The number of endoscopic examinations performed is rising. Epidemiological data and the workload of well developed units show that annual requirements per head of population are approaching: Upper gastrointestinal 1 in 100 Flexible sigmoidoscopy 1 in 500 Colonoscopy 1 in 500 ERCP 1 in 2000 (2) Open access endoscopy to general practitioners is desirable and increasingly sought. For a district general hospital serving a population of 250,000, this workload entails about 3500 procedures annually, performed during 10 half day routine sessions plus emergency work. (3) High standards of training and experience are needed by all staff, who must work in purpose built accommodation designed to promote efficient and safe practice. (4) The endoscopy unit should be adjacent to day care facilities and near the x ray department. There should be easy access to wards. (5) An endoscopy unit needs at least two endoscopy rooms; a fully ventilated cleaning/disinfection area; rooms for patient reception, preparation, and recovery; and accommodation for administration, storage, and staff amenities. (6) The service should be consultant based. At least 10 clinical sessions are required, made up of six or more consultant sessions and two to four clinical assistant, hospital practitioner, or staff specialist sessions. Each consultant should be expected to commit at least two sessions weekly to endoscopy. Extra consultant sessions may be needed to provide an efficient service. (7) A specially trained nursing sister (grade G or H) and five other endoscopy nurses are needed to care for the patients; their work may be supplemented by care assistants. (8) A new post of endoscopy department assistant (analogous to an operating department assistant) is proposed to maintain and prepare instruments, and to give technical assistance during procedures. (9) A full time secretary should be employed. Records, appointments, and audit should be computer based. (10) ERCP needs the collaboration of an interventional radiologist working with high quality x ray equipment in a specially prepared radiology screening room. This facility may need to serve more than one hospital. (11) A gastrointestinal measurement laboratory can conveniently be combined with the endoscopy unit. In some hospitals one or more gastrointestinal measurement technicians may staff this laboratory. (12) An endoscopy unit is a service department analogous to a radiology department. It needs an annual budget.
Full text
PDF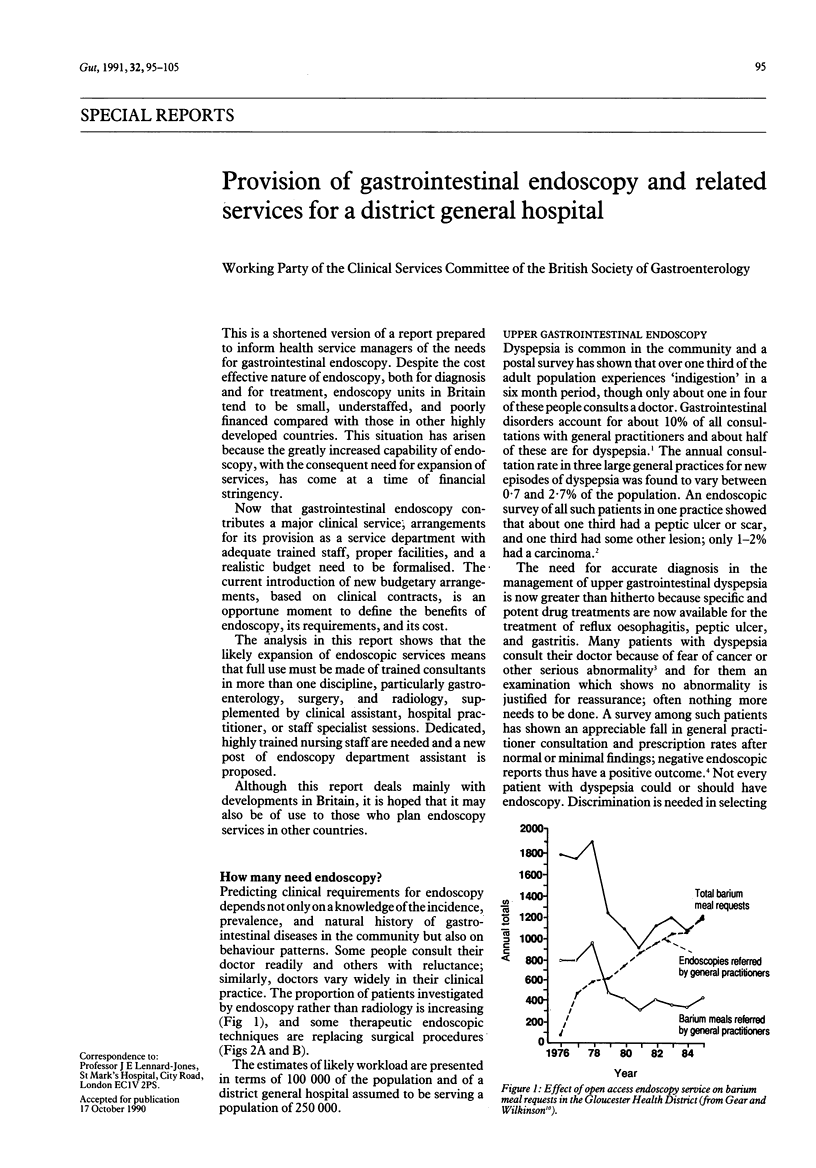


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bottrill P. Gastroenterology: gastrointestinal endoscopy--clinical practice. Nurs Stand. 1990 Jan 24;4(18):26–29. doi: 10.7748/ns.4.18.26.s38. [DOI] [PubMed] [Google Scholar]
- Brown C., Rees W. D. Dyspepsia in general practice. BMJ. 1990 Mar 31;300(6728):829–830. doi: 10.1136/bmj.300.6728.829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cockel R., Colin-Jones D. G., Schiller K. F. Gastrointestinal endoscopy services--a review of the 70s with predictions for the 80s. Health Trends. 1982 May;14(2):46–49. [PubMed] [Google Scholar]
- Colin-Jones D. G. Endoscopy or radiology for upper gastrointestinal symptoms? Lancet. 1986 May 3;1(8488):1022–1023. doi: 10.1016/s0140-6736(86)91283-3. [DOI] [PubMed] [Google Scholar]
- Gear M. W., Barnes R. J. Endoscopic studies of dyspepsia in a general practice. Br Med J. 1980 May 3;280(6223):1136–1137. doi: 10.1136/bmj.280.6223.1136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gear M. W., Dent N. A., Colin-Jones D. G., Lennard-Jones J. H., Colley J. R. Future needs for ERCP: incidence of conditions leading to bile duct obstruction and requirements for diagnostic and therapeutic biliary procedures. Gut. 1990 Oct;31(10):1150–1155. doi: 10.1136/gut.31.10.1150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gear M. W., Wilkinson S. P. Open-access upper alimentary endoscopy. Br J Hosp Med. 1989 May;41(5):438, 440, 442-4. [PubMed] [Google Scholar]
- Geerdsen J., Pedersen V. M., Kjaergård H., Nordkild P., Andersen J. Radiation dose in investigations of the large bowel. Comparison of radiation doses in examinations of the colon with double-contrast barium enema with the Welin modification and colonoscopy. Scand J Gastroenterol. 1986 Jun;21(5):556–558. doi: 10.3109/00365528609003099. [DOI] [PubMed] [Google Scholar]
- Hardcastle J. D., Thomas W. M., Chamberlain J., Pye G., Sheffield J., James P. D., Balfour T. W., Amar S. S., Armitage N. C., Moss S. M. Randomised, controlled trial of faecal occult blood screening for colorectal cancer. Results for first 107,349 subjects. Lancet. 1989 May 27;1(8648):1160–1164. doi: 10.1016/s0140-6736(89)92750-5. [DOI] [PubMed] [Google Scholar]
- Herlinger H., Glanville J. N., Kreel L. An evaluation of the double contrast barium meal (DCBM) against endoscopy. Clin Radiol. 1977 May;28(3):307–314. doi: 10.1016/s0009-9260(77)80187-6. [DOI] [PubMed] [Google Scholar]
- Jones R. Dyspeptic symptoms in the community. Gut. 1989 Jul;30(7):893–898. doi: 10.1136/gut.30.7.893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones R. Upper gastrointestinal endoscopy--a view from general practice. J R Coll Gen Pract. 1986 Jan;36(282):6–8. [PMC free article] [PubMed] [Google Scholar]
- Jones R. What happens to patients with non-ulcer dyspepsia after endoscopy? Practitioner. 1988 Jan;232(1441):75-6, 78. [PubMed] [Google Scholar]
- Kahn K. L., Kosecoff J., Chassin M. R., Solomon D. H., Brook R. H. The use and misuse of upper gastrointestinal endoscopy. Ann Intern Med. 1988 Oct 15;109(8):664–670. doi: 10.7326/0003-4819-109-8-664. [DOI] [PubMed] [Google Scholar]
- Kerrigan D. D., Brown S. R., Hutchinson G. H. Open access gastroscopy: too much to swallow? BMJ. 1990 Feb 10;300(6721):374–376. doi: 10.1136/bmj.300.6721.374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindsay D. C., Freeman J. G., Cobden I., Record C. O. Should colonoscopy be the first investigation for colonic disease? Br Med J (Clin Res Ed) 1988 Jan 16;296(6616):167–169. doi: 10.1136/bmj.296.6616.167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lydeard S., Jones R. Factors affecting the decision to consult with dyspepsia: comparison of consulters and non-consulters. J R Coll Gen Pract. 1989 Dec;39(329):495–498. [PMC free article] [PubMed] [Google Scholar]
- Management of dyspepsia: report of a working party. Lancet. 1988 Mar 12;1(8585):576–579. [PubMed] [Google Scholar]
- Mann J., Holdstock G., Harman M., Machin D., Loehry C. A. Scoring system to improve cost effectiveness of open access endoscopy. Br Med J (Clin Res Ed) 1983 Oct 1;287(6397):937–940. doi: 10.1136/bmj.287.6397.937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salter R. H. X-ray negative dyspepsia. Br Med J. 1977 Jul 23;2(6081):235–236. doi: 10.1136/bmj.2.6081.235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scott B., Atkinson M. Gastroenterology services: a regional review of changes over a five year period (1981-86). Gut. 1989 May;30(5):695–700. doi: 10.1136/gut.30.5.695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scott B. Endoscopic demands in the 90's. Gut. 1990 Feb;31(2):125–126. doi: 10.1136/gut.31.2.125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vellacott K. D., Virjee J. Audit on the use of the barium enema. Gut. 1986 Feb;27(2):182–185. doi: 10.1136/gut.27.2.182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams B., Luckas M., Ellingham J. H., Dain A., Wicks A. C. Do young patients with dyspepsia need investigation? Lancet. 1988 Dec 10;2(8624):1349–1351. doi: 10.1016/s0140-6736(88)90879-3. [DOI] [PubMed] [Google Scholar]