

Abstract
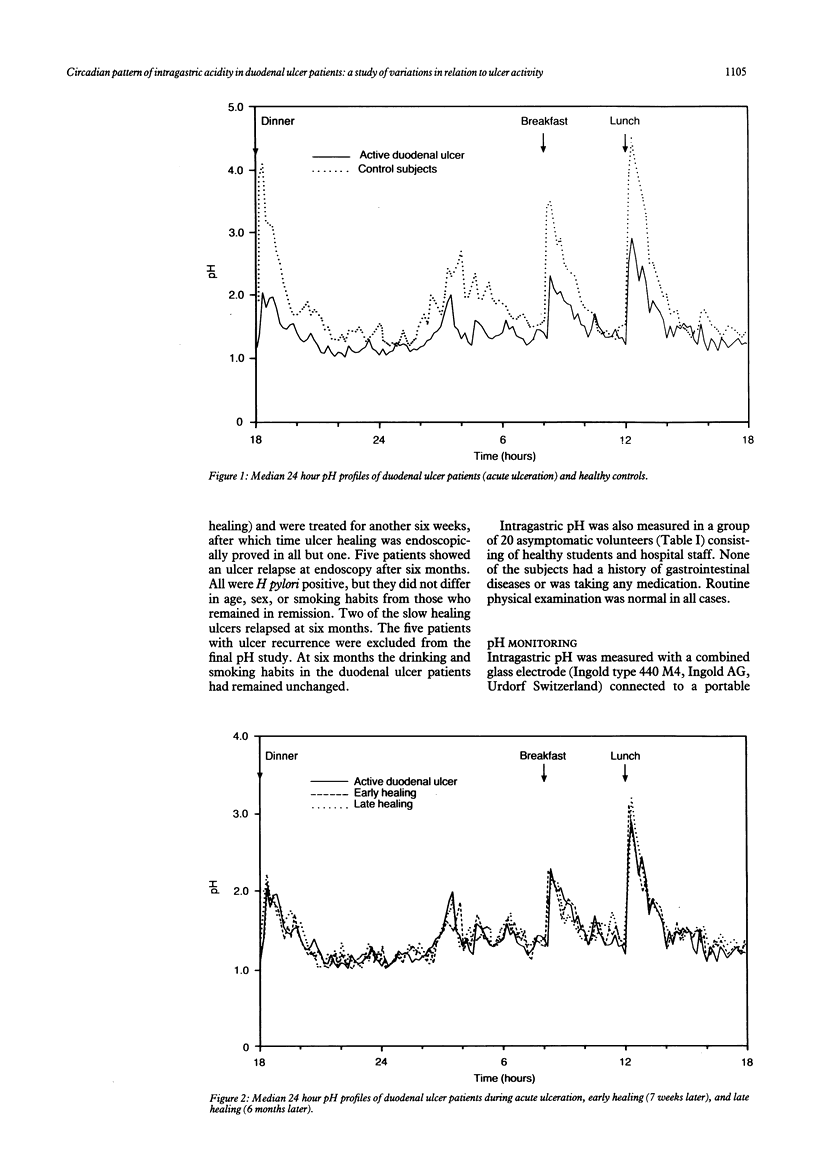
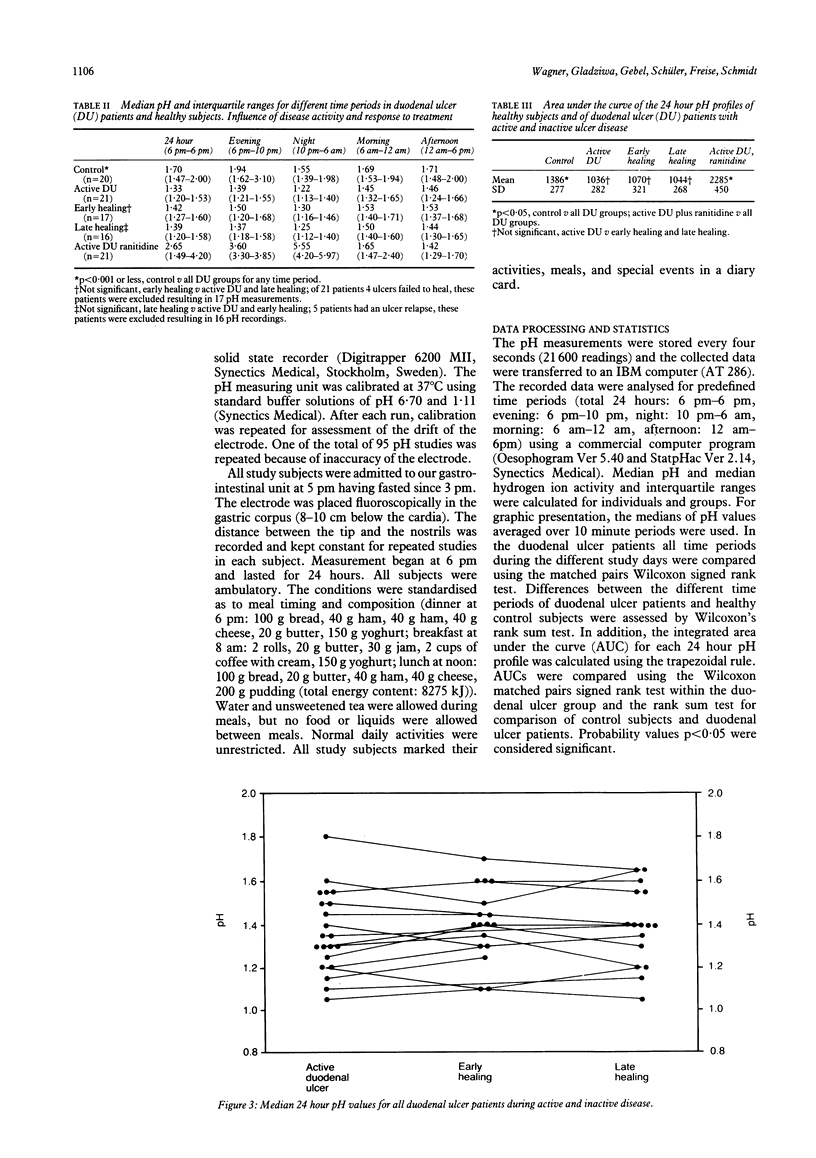
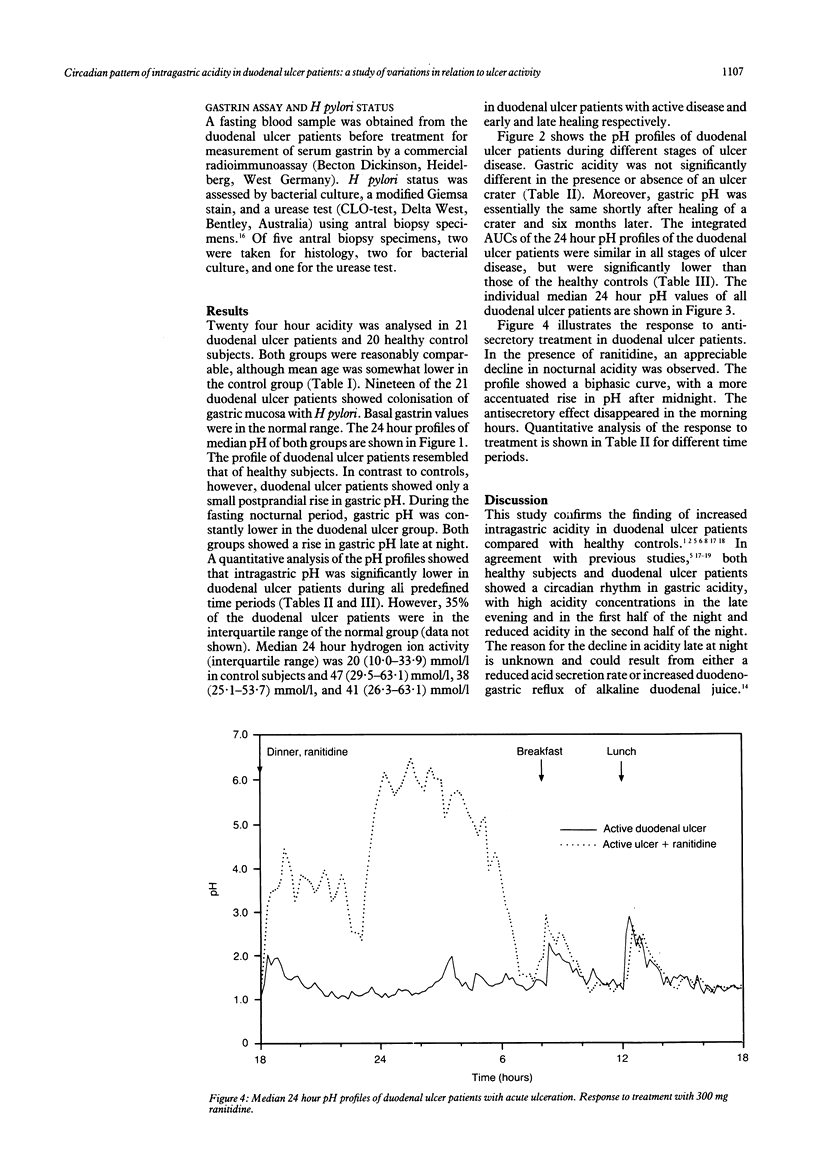
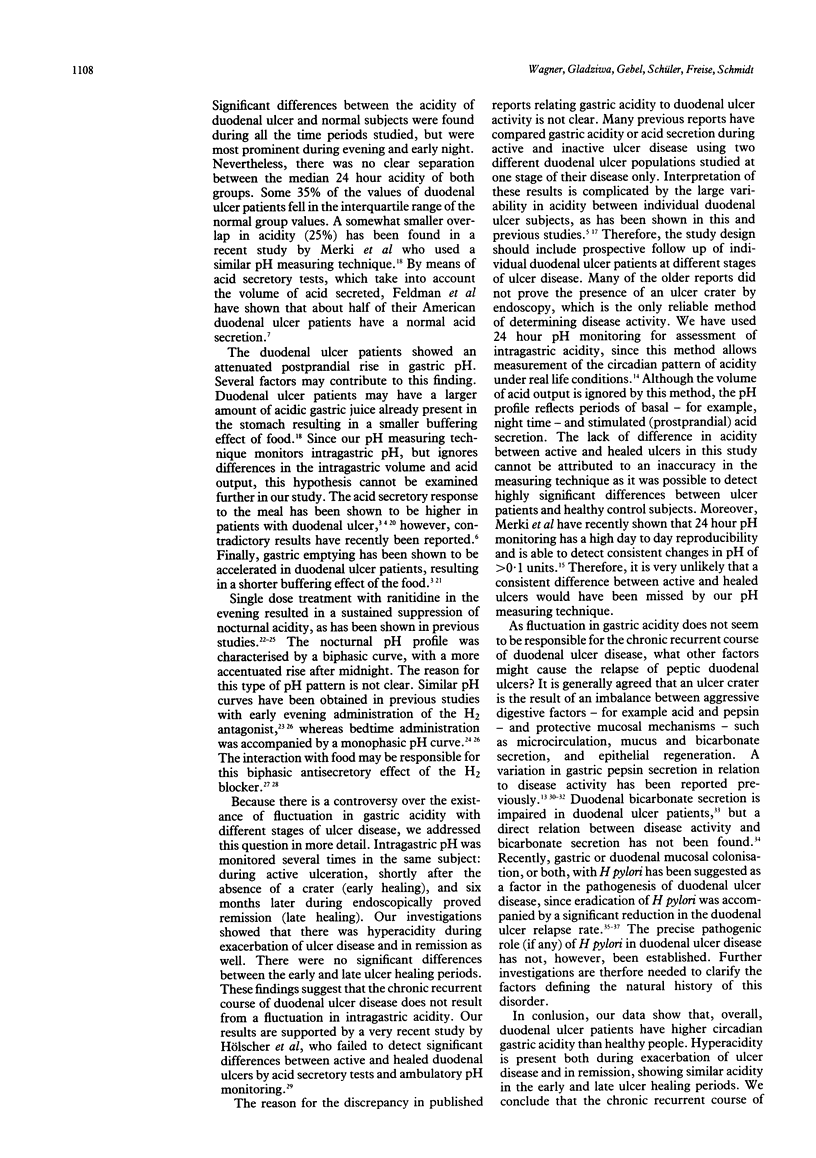
The relation between intragastric acidity and duodenal ulcer activity was studied prospectively in 21 patients with endoscopically proved duodenal ulcers. The 24 hour intragastric acidity was measured on four separate occasions by continuous recording using combined glass electrodes: (a) in the presence of an ulcer crater without treatment; (b) during active ulceration being treated with ranitidine; (c) during early healing after a six week course of ranitidine; (d) during late healing six months after acute ulceration. Intragastric acidity was also monitored in 20 healthy subjects. At all stages of ulcer activity and during all predefined time periods, duodenal ulcer patients had significantly higher gastric acidity than healthy control subjects. Duodenal ulcer patients showed a similar circadian pattern of intragastric acidity during exacerbation of ulcer disease and in remission during the early and late ulcer healing periods. These results argue against a direct relation between the activity of duodenal ulcer disease and gastric acidity. It is concluded that the chronic recurrent course of duodenal ulcer disease does not result from a fluctuation in intragastric acidity.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Achord J. L. Gastric pepsin and acid secretion in patients with acute and healed duodenal ulcer. Gastroenterology. 1981 Jul;81(1):15–18. [PubMed] [Google Scholar]
- Bauerfeind P., Cilluffo T., Emde C., Fimmel C., Kohler W., Gasser T., Blum A. L. Reduction of gastric acidity with ranitidine or famotidine: early evening dosage is more effective than late evening dosage. Digestion. 1987;37(4):217–222. doi: 10.1159/000199504. [DOI] [PubMed] [Google Scholar]
- Blair A. J., 3rd, Feldman M., Barnett C., Walsh J. H., Richardson C. T. Detailed comparison of basal and food-stimulated gastric acid secretion rates and serum gastrin concentrations in duodenal ulcer patients and normal subjects. J Clin Invest. 1987 Feb;79(2):582–587. doi: 10.1172/JCI112850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blaser M. J. Gastric Campylobacter-like organisms, gastritis, and peptic ulcer disease. Gastroenterology. 1987 Aug;93(2):371–383. doi: 10.1016/0016-5085(87)91028-6. [DOI] [PubMed] [Google Scholar]
- Bodemar G., Norlander B., Walan A., Larsson R. Short- and long-term treatment with cimetidine in peptic ulcer disease and the pharmacokinetics of cimetidine. Scand J Gastroenterol Suppl. 1979;55:96–106. [PubMed] [Google Scholar]
- DRAGSTEDT L. R. Cause of peptic ulcer. J Am Med Assoc. 1959 Jan 17;169(3):203–209. doi: 10.1001/jama.1959.03000200001001. [DOI] [PubMed] [Google Scholar]
- Feldman M., Richardson C. T., Lam S. K., Samloff I. M. Comparison of gastric acid secretion rates and serum pepsinogen I and II concentrations in Occidental and Oriental duodenal ulcer patients. Gastroenterology. 1988 Sep;95(3):630–635. doi: 10.1016/s0016-5085(88)80008-8. [DOI] [PubMed] [Google Scholar]
- Feldman M., Richardson C. T. Total 24-hour gastric acid secretion in patients with duodenal ulcer. Comparison with normal subjects and effects of cimetidine and parietal cell vagotomy. Gastroenterology. 1986 Mar;90(3):540–544. doi: 10.1016/0016-5085(86)91106-6. [DOI] [PubMed] [Google Scholar]
- Fimmel C. J., Etienne A., Cilluffo T., von Ritter C., Gasser T., Rey J. P., Caradonna-Moscatelli P., Sabbatini F., Pace F., Bühler H. W. Long-term ambulatory gastric pH monitoring: validation of a new method and effect of H2-antagonists. Gastroenterology. 1985 Jun;88(6):1842–1851. doi: 10.1016/0016-5085(85)90009-5. [DOI] [PubMed] [Google Scholar]
- Food and H2 blockade. Lancet. 1988 Oct 8;2(8615):852–853. [PubMed] [Google Scholar]
- Fordtran J. S., Walsh J. H. Gastric acid secretion rate and buffer content of the stomach after eating. Results in normal subjects and in patients with duodenal ulcer. J Clin Invest. 1973 Mar;52(3):645–657. doi: 10.1172/JCI107226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gledhill T., Howard O. M., Buck M., Paul A., Hunt R. H. Single nocturnal dose of an H2 receptor antagonist for the treatment of duodenal ulcer. Gut. 1983 Oct;24(10):904–908. doi: 10.1136/gut.24.10.904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Isenberg J. I., Selling J. A., Hogan D. L., Koss M. A. Impaired proximal duodenal mucosal bicarbonate secretion in patients with duodenal ulcer. N Engl J Med. 1987 Feb 12;316(7):374–379. doi: 10.1056/NEJM198702123160704. [DOI] [PubMed] [Google Scholar]
- Jalan K. N., Mahalanabis D., Maitra T. K., Agarwal S. K. Gastric acid secretion rate and buffer content of the stomach after a rice- and a wheat-based meal in normal subjects and patients with duodenal ulcer. Gut. 1979 May;20(5):389–393. doi: 10.1136/gut.20.5.389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston D. A., Wormsley K. G. The effect of food on ranitidine-induced inhibition of nocturnal gastric secretion. Aliment Pharmacol Ther. 1988 Dec;2(6):507–511. doi: 10.1111/j.1365-2036.1988.tb00724.x. [DOI] [PubMed] [Google Scholar]
- LITMAN A. Basal gastric secretion in patients with duodenal ulcer: a long term study of variations in relation to ulcer activity. Gastroenterology. 1962 Aug;43:166–173. [PubMed] [Google Scholar]
- Lam S. K., Isenberg J. I., Grossman M. I., Lane W. H., Walsh J. H. Gastric acid secretion is abnormally sensitive to endogenous gastrin released after peptone test meals in duodenal ulcer patients. J Clin Invest. 1980 Feb;65(2):555–562. doi: 10.1172/JCI109699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malagelada J. R., Longstreth G. F., Deering T. B., Summerskill W. H., Go V. L. Gastric secretion and emptying after ordinary meals in duodenal ulcer. Gastroenterology. 1977 Nov;73(5):989–994. [PubMed] [Google Scholar]
- Marshall B. J., Goodwin C. S., Warren J. R., Murray R., Blincow E. D., Blackbourn S. J., Phillips M., Waters T. E., Sanderson C. R. Prospective double-blind trial of duodenal ulcer relapse after eradication of Campylobacter pylori. Lancet. 1988 Dec 24;2(8626-8627):1437–1442. doi: 10.1016/s0140-6736(88)90929-4. [DOI] [PubMed] [Google Scholar]
- Merki H. S., Fimmel C. J., Walt R. P., Harre K., Röhmel J., Witzel L. Pattern of 24 hour intragastric acidity in active duodenal ulcer disease and in healthy controls. Gut. 1988 Nov;29(11):1583–1587. doi: 10.1136/gut.29.11.1583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merki H. S., Witzel L., Walt R. P., Cohnen E., Harre K., Heim J., Mappes A., Röhmel J. Day-to-day variation of 24-hour intragastric acidity. Gastroenterology. 1988 Apr;94(4):887–891. doi: 10.1016/0016-5085(88)90543-4. [DOI] [PubMed] [Google Scholar]
- Merki H., Witzel L., Harre K., Scheurle E., Neumann J., Röhmel J. Single dose treatment with H2 receptor antagonists: is bedtime administration too late? Gut. 1987 Apr;28(4):451–454. doi: 10.1136/gut.28.4.451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore J. G., Halberg F. Circadian rhythm of gastric acid secretion in men with active duodenal ulcer. Dig Dis Sci. 1986 Nov;31(11):1185–1191. doi: 10.1007/BF01296516. [DOI] [PubMed] [Google Scholar]
- Pugh S., Williams S. E., Lewin M. R., Ishaque M., Barton T. P., Bose K., Bardhan K. D., Clark C. G. Duodenal and antral mucosal prostaglandin E2 synthesis in a study of normal subjects and all stages of duodenal ulcer disease treated by H2 receptor antagonists. Gut. 1989 Feb;30(2):161–165. doi: 10.1136/gut.30.2.161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Savarino V., Mela G. S., Scalabrini P., Di Timoteo E., Magnolia M. R., Celle G. Continuous 24-hour intragastric pH monitoring in the evaluation of the effect of a nightly dose of famotidine, ranitidine and placebo on gastric acidity of patients with duodenal ulcer. Digestion. 1987;37(2):103–109. doi: 10.1159/000199475. [DOI] [PubMed] [Google Scholar]
- Savarino V., Mela G. S., Scalabrini P., Sumberaz A., Fera G., Celle G. 24-hour study of intragastric acidity in duodenal ulcer patients and normal subjects using continuous intraluminal pH-metry. Dig Dis Sci. 1988 Sep;33(9):1077–1080. doi: 10.1007/BF01535781. [DOI] [PubMed] [Google Scholar]
- Taylor W. H. Pepsins of patients with peptic ulcer. Nature. 1970 Jul 4;227(5253):76–77. doi: 10.1038/227076a0. [DOI] [PubMed] [Google Scholar]
- Thomson A. B., Pinchbeck B. R., Kirdeikis J., Zuk L., Marriage B., Prat A. A single night-time dose of famotidine is equivalent to ranitidine in decreasing 24-hour gastric acidity in asymptomatic duodenal ulcer subjects. Aliment Pharmacol Ther. 1989 Apr;3(2):199–210. doi: 10.1111/j.1365-2036.1989.tb00206.x. [DOI] [PubMed] [Google Scholar]
- Wagner S., Freise J., Bär W., Fritsch S., Schmidt F. W. Epidemiologie und Therapie der Campylobacter-pylori-Infektion. Dtsch Med Wochenschr. 1989 Mar 17;114(11):407–413. doi: 10.1055/s-2008-1066609. [DOI] [PubMed] [Google Scholar]
- Whittingham S., Naselli G., McNeilage L. J., Coppel R. L., Sturgess A. D. Serological diagnosis of primary Sjögren's syndrome by means of human recombinant La (SS-B) as nuclear antigen. Lancet. 1987 Jul 4;2(8549):1–3. [PubMed] [Google Scholar]
- Wolfe M. M., Soll A. H. The physiology of gastric acid secretion. N Engl J Med. 1988 Dec 29;319(26):1707–1715. doi: 10.1056/NEJM198812293192605. [DOI] [PubMed] [Google Scholar]