

Abstract
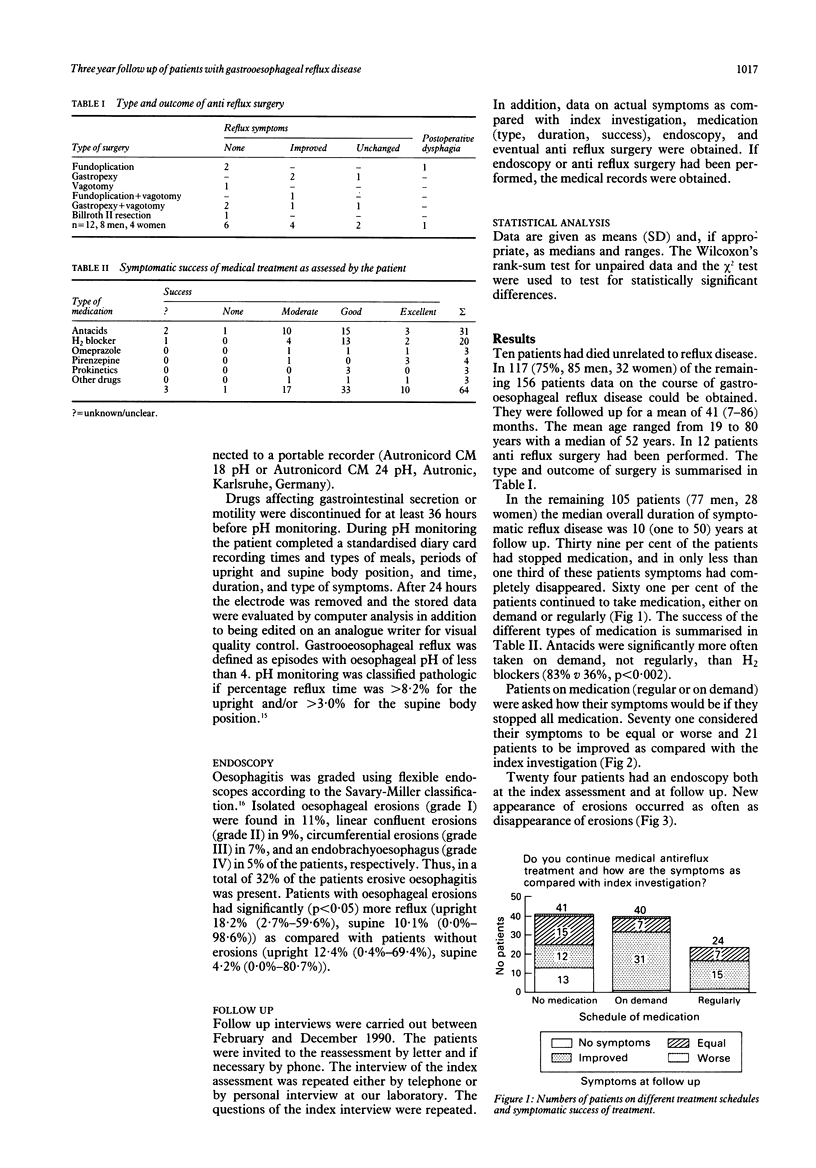
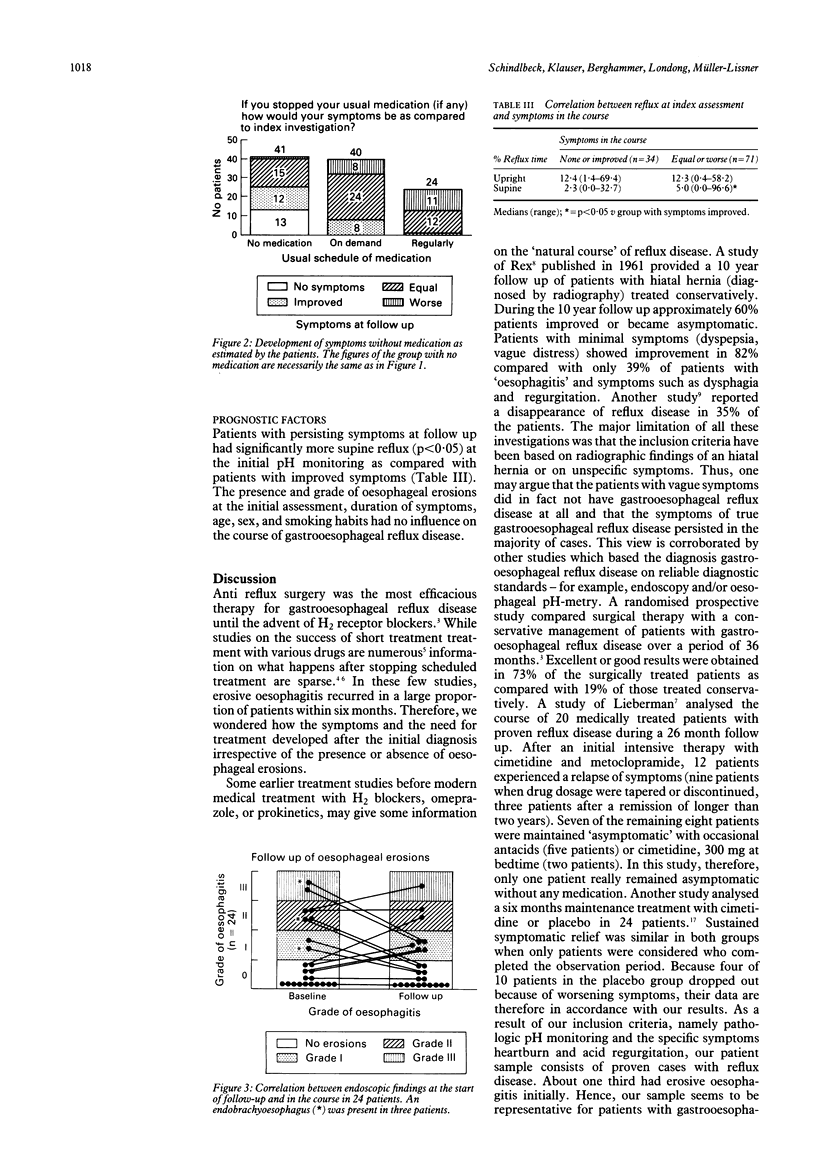
Data on the natural course of gastrooesophageal reflux disease are sparse. One hundred and sixty six patients with typical reflux symptoms (heartburn and/or acid regurgitation) and pathologic pH monitoring (reflux time > 8.2% upright and/or > 3.0% supine) were studied. The patients were followed up by questionnaire and interview for a mean of 41 (seven to 86) months after diagnosis of reflux disease. Ten patients had died of diseases not reflux related. In 117 (75%) of the remaining 156 patients data on the course of gastrooesophageal reflux disease could be obtained. In 12 patients anti reflux surgery had been performed. Forty one (39%) of the remaining 105 patients have stopped taking medical therapy, in 13 of these patients symptoms had completely disappeared. Sixty four patients continued on medication (40 on demand, 24 regularly). When asked how their symptoms would be if they completely stopped medication, 71 patients considered their symptoms to be equal or worse and 21 patients to be improved as compared with the initial investigation. Patients with persisting symptoms at follow up had significantly more supine reflux (p < 0.05) at the initial pH monitoring as compared with patients with improved symptoms. The presence and grade of oesophageal erosions at initial endoscopy, duration of symptoms, age, sex, and smoking habits had no influence on the course of gastrooesophageal reflux disease. In conclusion, reflux symptoms disappear only in a minority of patients with proven gastrooesophageal reflux disease. More than half of all patients continue medication, either on demand or regularly. Severe supine reflux is an unfavourable prognostic factor.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Behar J., Sheahan D. G., Biancani P., Spiro H. M., Storer E. H. Medical and surgical management of reflux esophagitis. A 38-month report of a prospective clinical trial. N Engl J Med. 1975 Aug 7;293(6):263–268. doi: 10.1056/NEJM197508072930602. [DOI] [PubMed] [Google Scholar]
- DeMeester T. R., Wang C. I., Wernly J. A., Pellegrini C. A., Little A. G., Klementschitsch P., Bermudez G., Johnson L. F., Skinner D. B. Technique, indications, and clinical use of 24 hour esophageal pH monitoring. J Thorac Cardiovasc Surg. 1980 May;79(5):656–670. [PubMed] [Google Scholar]
- Heading R. C. Epidemiology of oesophageal reflux disease. Scand J Gastroenterol Suppl. 1989;168:33–37. [PubMed] [Google Scholar]
- Hetzel D. J., Dent J., Reed W. D., Narielvala F. M., Mackinnon M., McCarthy J. H., Mitchell B., Beveridge B. R., Laurence B. H., Gibson G. G. Healing and relapse of severe peptic esophagitis after treatment with omeprazole. Gastroenterology. 1988 Oct;95(4):903–912. doi: 10.1016/0016-5085(88)90162-x. [DOI] [PubMed] [Google Scholar]
- Kaul B., Petersen H., Erichsen H., Myrvold H. E., Grette K., Halvorsen T., Fjøsne U. Gastroesophageal reflux disease. Acute and maintenance treatments with cimetidine. Scand J Gastroenterol. 1986 Mar;21(2):139–145. doi: 10.3109/00365528609034638. [DOI] [PubMed] [Google Scholar]
- Klauser A. G., Schindlbeck N. E., Müller-Lissner S. A. Esophageal 24-h pH monitoring: is prior manometry necessary for correct positioning of the electrode? Am J Gastroenterol. 1990 Nov;85(11):1463–1467. [PubMed] [Google Scholar]
- Koelz H. R., Birchler R., Bretholz A., Bron B., Capitaine Y., Delmore G., Fehr H. F., Fumagalli I., Gehrig J., Gonvers J. J. Healing and relapse of reflux esophagitis during treatment with ranitidine. Gastroenterology. 1986 Nov;91(5):1198–1205. doi: 10.1016/s0016-5085(86)80017-8. [DOI] [PubMed] [Google Scholar]
- Koelz H. R. Treatment of reflux esophagitis with H2-blockers, antacids and prokinetic drugs. An analysis of randomized clinical trials. Scand J Gastroenterol Suppl. 1989;156:25–36. [PubMed] [Google Scholar]
- Lieberman D. A. Medical therapy for chronic reflux esophagitis. Long-term follow-up. Arch Intern Med. 1987 Oct;147(10):1717–1720. [PubMed] [Google Scholar]
- Nebel O. T., Fornes M. F., Castell D. O. Symptomatic gastroesophageal reflux: incidence and precipitating factors. Am J Dig Dis. 1976 Nov;21(11):953–956. doi: 10.1007/BF01071906. [DOI] [PubMed] [Google Scholar]
- Palmer E. D. The hiatus hernia-esophagitis-esophageal stricture complex. Twenty-year prospective study. Am J Med. 1968 Apr;44(4):566–579. doi: 10.1016/0002-9343(68)90057-0. [DOI] [PubMed] [Google Scholar]
- REX J. C., ANDERSEN H. A., BARTHOLOMEW L. G., CAIN J. C. Esophageal hiatal hernia: a 10-year study of medically treated cases. JAMA. 1961 Oct 21;178:271–274. doi: 10.1001/jama.1961.03040420011003. [DOI] [PubMed] [Google Scholar]
- Schindlbeck N. E., Heinrich C., König A., Dendorfer A., Pace F., Müller-Lissner S. A. Optimal thresholds, sensitivity, and specificity of long-term pH-metry for the detection of gastroesophageal reflux disease. Gastroenterology. 1987 Jul;93(1):85–90. doi: 10.1016/0016-5085(87)90318-0. [DOI] [PubMed] [Google Scholar]
- Schindlbeck N. E., Ippisch H., Klauser A. G., Müller-Lissner S. A. Which pH threshold is best in esophageal pH monitoring? Am J Gastroenterol. 1991 Sep;86(9):1138–1141. [PubMed] [Google Scholar]
- de Caestecker J. S., Blackwell J. N., Pryde A., Heading R. C. Daytime gastro-oesophageal reflux is important in oesophagitis. Gut. 1987 May;28(5):519–526. doi: 10.1136/gut.28.5.519. [DOI] [PMC free article] [PubMed] [Google Scholar]