

Abstract
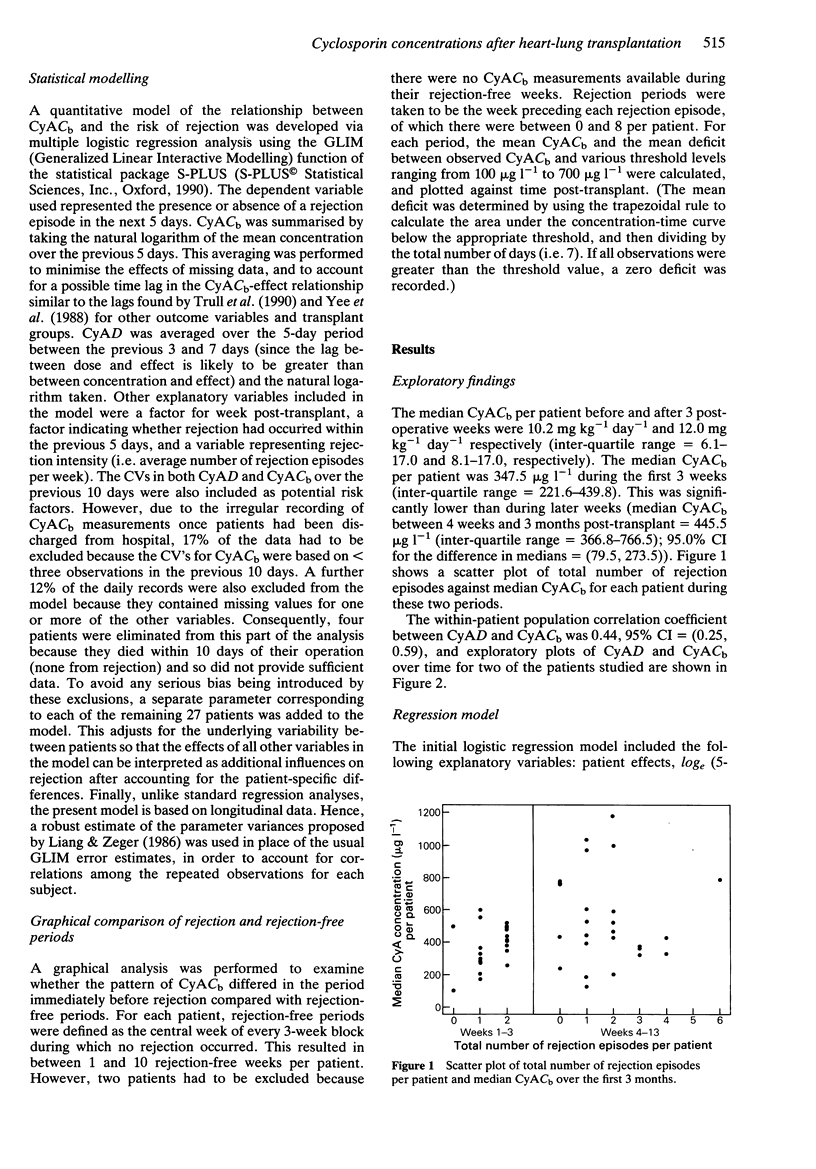
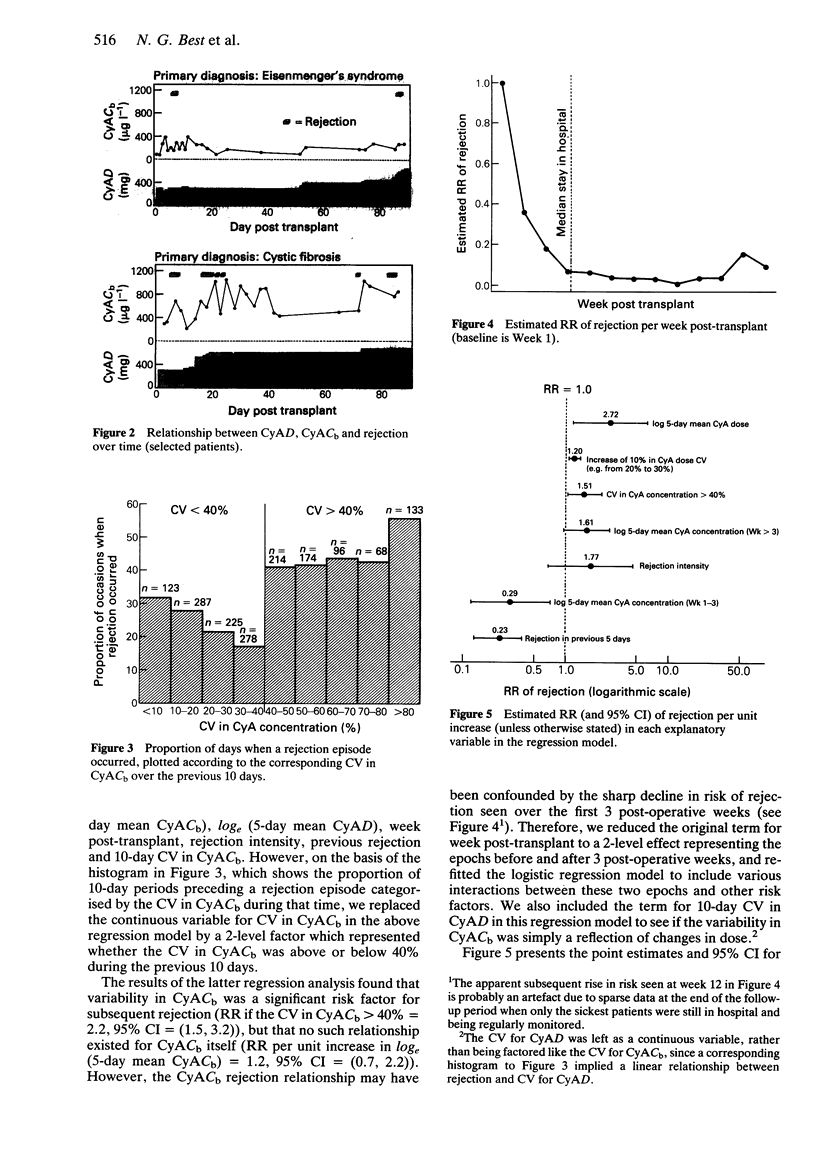
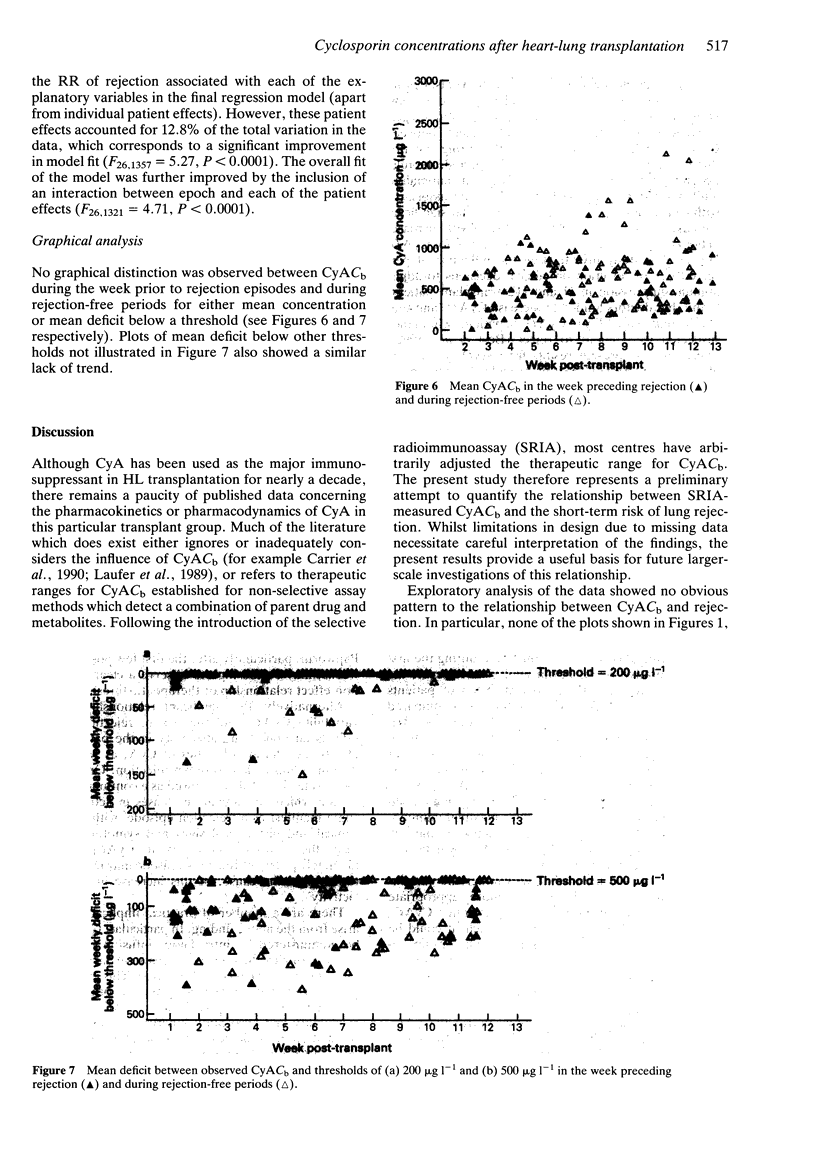
1. The relationship between blood cyclosporin concentration (CyACb) and a patient's risk of organ rejection following heart-lung (HL) transplantation was investigated. 2. Longitudinal data were collected for 90 days post-operation for 31 HL transplant recipients. Following exploratory analysis, a multiple logistic regression model with a binary outcome variable representing presence or absence of lung rejection (as defined on biopsy findings and/or intention to treat) in the next 5 days was fitted to the data. 3. A significant interaction between time post-transplant and CyACb was found. During weeks 1-3, the relative risk (RR) of rejection per unit increase in log(e) (5-day mean CyACb) was reduced: RR = 0.29, 95% confidence interval (CI) = (0.12, 0.72). After 3 post-operative weeks, this trend was reversed: RR = 1.61, 95% CI = (0.96, 2.70). Increases in cyclosporin dose (CyAD) and in coefficient of variation (CV) for both CyAD and CyACb over the previous 10 days significantly increased the risk of rejection: RR per unit increase in log(e) (5-day mean CyAD) = 2.72, 95% CI = (1.18, 6.25); RR per increase of 10% (i.e. from, say, 20% to 30%) in the CV for CyAD = 1.20, 95% CI = (1.07, 1.36); RR if the CV for CyACb > 40% = 1.51, 95% CI = (1.01, 2.27). Administration of high dose steroids in the previous 5 days was found to protect against further rejection: RR if steroid treatment was given = 0.23, 95% CI = (0.13, 0.38).(ABSTRACT TRUNCATED AT 250 WORDS)
Full text
PDF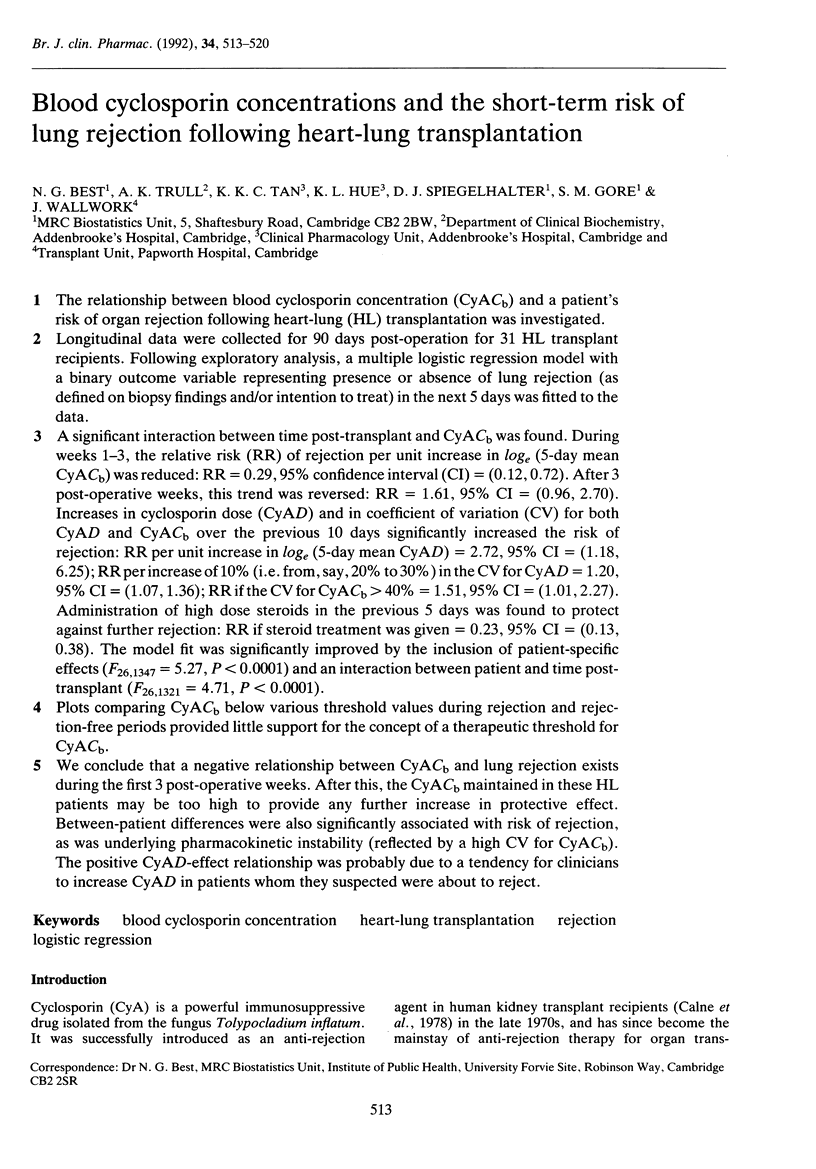


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Carrier M., Russell D. H., Cork R. C., Wild J., Emery R. W., Copeland J. G. Analysis of risk factors for acute allograft rejection after heart transplantation. J Heart Transplant. 1990 Jul-Aug;9(4):372–375. [PubMed] [Google Scholar]
- Johansson A., Möller E. Evidence that the immunosuppressive effects of FK506 and cyclosporine are identical. Transplantation. 1990 Dec;50(6):1001–1007. doi: 10.1097/00007890-199012000-00021. [DOI] [PubMed] [Google Scholar]
- Kahan B. D., Grevel J. Optimization of cyclosporine therapy in renal transplantation by a pharmacokinetic strategy. Transplantation. 1988 Nov;46(5):631–644. doi: 10.1097/00007890-198811000-00002. [DOI] [PubMed] [Google Scholar]
- Laufer G., Miholic J., Laczkovics A., Wollenek G., Holzinger C., Hajek-Rosenmeier A., Wuzl G., Schreiner W., Buxbaum P., Wolner E. Independent risk factors predicting acute graft rejection in cardiac transplant recipients treated by triple drug immunosuppression. J Thorac Cardiovasc Surg. 1989 Dec;98(6):1113–1121. [PubMed] [Google Scholar]
- Reitz B. A., Burton N. A., Jamieson S. W., Bieber C. P., Pennock J. L., Stinson E. B., Shumway N. E. Heart and lung transplantation: autotransplantation and allotransplantation in primates with extended survival. J Thorac Cardiovasc Surg. 1980 Sep;80(3):360–372. [PubMed] [Google Scholar]
- Shaw L. M., Audet P. R., Grossman R. A., Fields L., Lensmeyer G. L., Dafoe D. C. Adjustment of cyclosporine dosage in renal transplant patients based on concentration measured specifically in whole blood: clinical outcome results and diagnostic utility. Transplant Proc. 1990 Jun;22(3):1267–1273. [PubMed] [Google Scholar]
- Tan K. K., Hue K. L., Strickland S. E., Trull A. K., Smyth R. L., Scott J. P., Kelman A. W., Whiting B., Higenbottam T. W., Wallwork J. Altered pharmacokinetics of cyclosporin in heart-lung transplant recipients with cystic fibrosis. Ther Drug Monit. 1990 Nov;12(6):520–524. doi: 10.1097/00007691-199011000-00002. [DOI] [PubMed] [Google Scholar]
- Tolkoff-Rubin N. E., Rubin R. H. The impact of cyclosporine therapy on the occurrence of infection in the renal transplant recipient. Transplant Proc. 1986 Apr;18(2 Suppl 1):168–176. [PubMed] [Google Scholar]
- Trull A., Hue K., Tan K., Gore S., Whitewood S., Smyth R., Scott J., Price C., Wallwork J. Cross-correlation of cyclosporine concentrations and biochemical measures of kidney and liver function in heart and heart-lung transplant recipients. Clin Chem. 1990 Aug;36(8 Pt 1):1474–1478. [PubMed] [Google Scholar]
- Wreghitt T. G., Hakim M., Gray J. J., Kucia S., Cory-Pearce R., Wallwork J., English T. A. A detailed study of cytomegalovirus infections in the first 160 heart and heart/lung transplant recipients at Papworth Hospital, Cambridge, England. Transplant Proc. 1987 Feb;19(1 Pt 3):2495–2496. [PubMed] [Google Scholar]
- Yee G. C., Self S. G., McGuire T. R., Carlin J., Sanders J. E., Deeg H. J. Serum cyclosporine concentration and risk of acute graft-versus-host disease after allogeneic marrow transplantation. N Engl J Med. 1988 Jul 14;319(2):65–70. doi: 10.1056/NEJM198807143190201. [DOI] [PubMed] [Google Scholar]