

Abstract
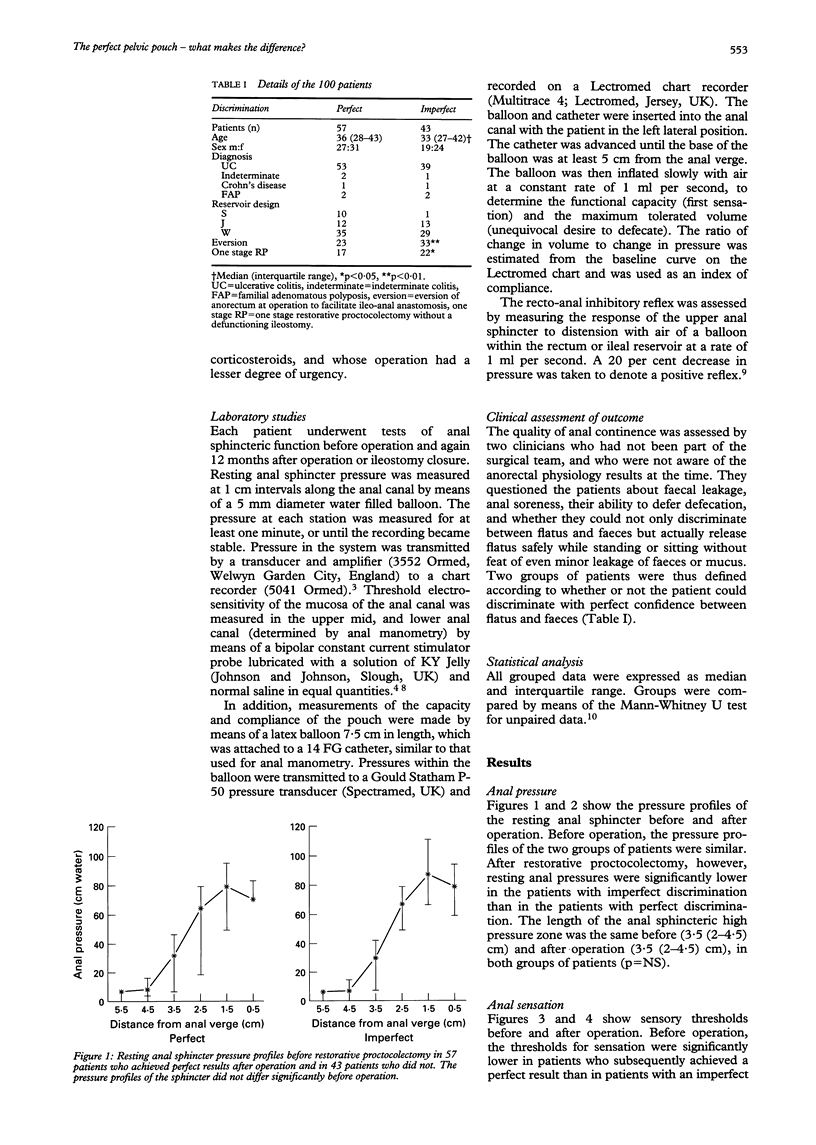
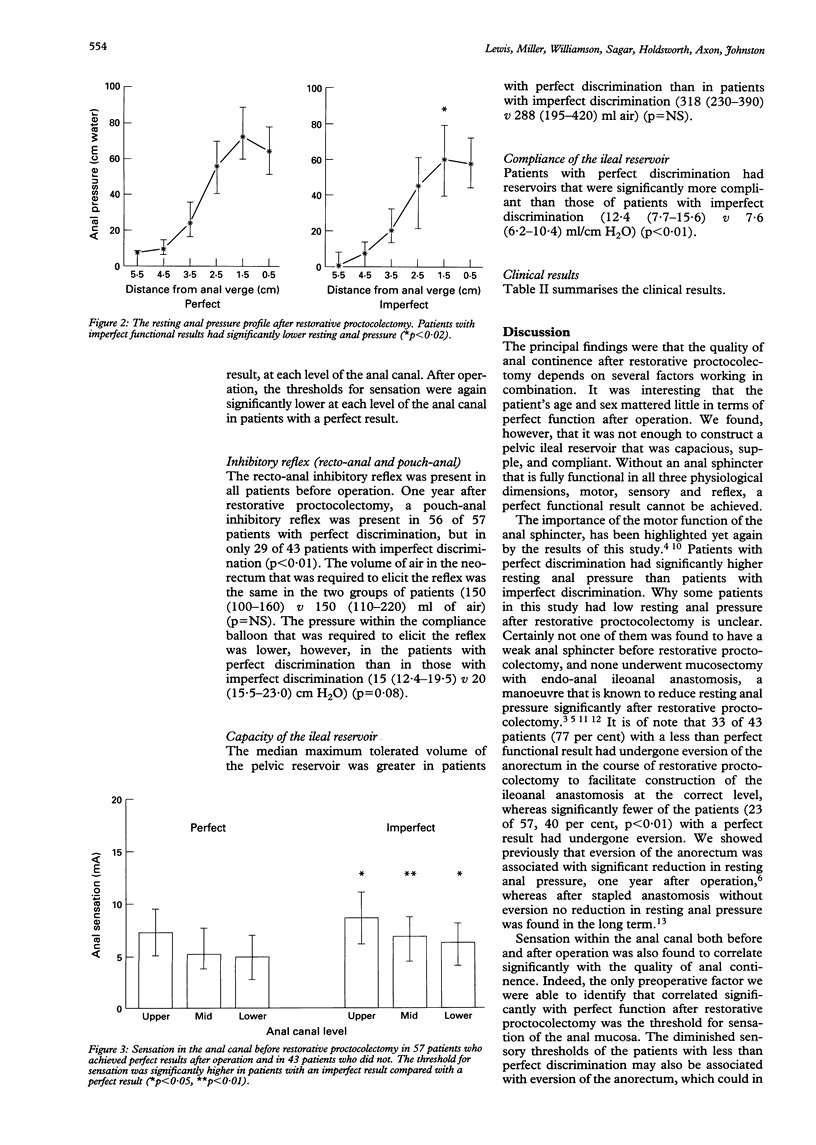
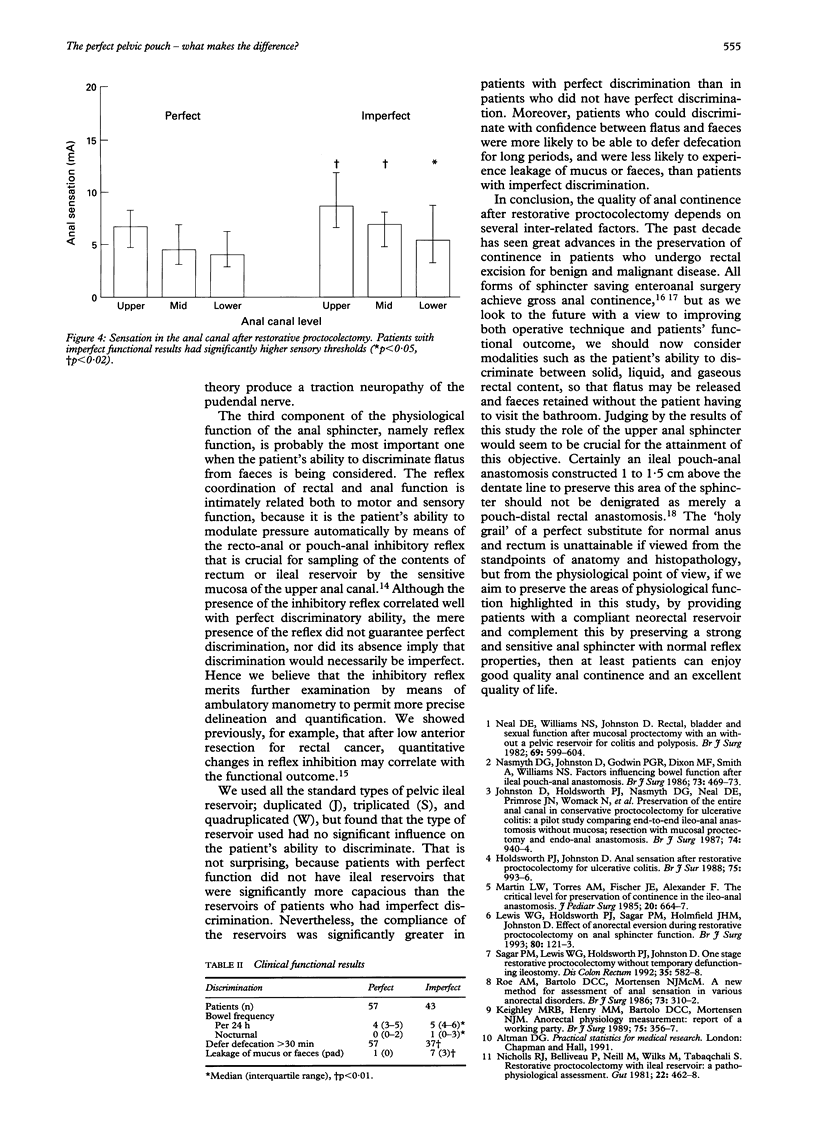
The aim of this study was to determine what factors are important for the achievement of perfect anal continence after restorative proctocolectomy. One hundred patients underwent paired studies of anorectal physiology before and one year after restorative proctocolectomy with pelvic ileal reservoir (11 S, 25 J, 64 W) with stapled ileoanal anastomosis, without mucosectomy. Fifty seven patients attained perfect anal continence and were able to discriminate flatus from faeces with such confidence that they were able to release flatus safely without fear of faecal soiling. The remaining 43 patients experienced minor problems in this regard. Four factors were found to correlate significantly with a perfect functional result (median, perfect v imperfect): maximum resting anal pressure (72 v 57 cm H2O, p < 0.02), the sensory threshold in the upper and mid-anal canal (7.3 v 8.6 and 5.3 v 7.0 mA, p < 0.05 and p < 0.02), compliance of the ileal reservoir (12.4 v 7.6 ml/cm H2O, p < 0.01), and the presence of a pouch-anal inhibitory reflex (56 of 57 patients v 29 of 43 patients, p < 0.01). The quality of anal continence depends on several factors: a complaint ileal reservoir, a strong sensitive anal sphincter, and normal reflex coordination of the activities of the reservoir and the sphincter. Excellent pouch-anal coordination is obtainable irrespective of the design of the reservoir, provided that these criteria are satisfied.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BENNETT R. C., DUTHIE H. L. THE FUNCTIONAL IMPORTANCE OF THE INTERNAL ANAL SPHINCTER. Br J Surg. 1964 May;51:355–357. doi: 10.1002/bjs.1800510514. [DOI] [PubMed] [Google Scholar]
- Choen S., Tsunoda A., Nicholls R. J. Prospective randomized trial comparing anal function after hand sewn ileoanal anastomosis with mucosectomy versus stapled ileoanal anastomosis without mucosectomy in restorative proctocolectomy. Br J Surg. 1991 Apr;78(4):430–434. doi: 10.1002/bjs.1800780415. [DOI] [PubMed] [Google Scholar]
- Holdsworth P. J., Johnston D. Anal sensation after restorative proctocolectomy for ulcerative colitis. Br J Surg. 1988 Oct;75(10):993–996. doi: 10.1002/bjs.1800751016. [DOI] [PubMed] [Google Scholar]
- Johnston D., Holdsworth P. J., Nasmyth D. G., Neal D. E., Primrose J. N., Womack N., Axon A. T. Preservation of the entire anal canal in conservative proctocolectomy for ulcerative colitis: a pilot study comparing end-to-end ileo-anal anastomosis without mucosal resection with mucosal proctectomy and endo-anal anastomosis. Br J Surg. 1987 Oct;74(10):940–944. doi: 10.1002/bjs.1800741020. [DOI] [PubMed] [Google Scholar]
- Keighley M. R., Henry M. M., Bartolo D. C., Mortensen N. J. Anorectal physiology measurement: report of a working party. Br J Surg. 1989 Apr;76(4):356–357. doi: 10.1002/bjs.1800760414. [DOI] [PubMed] [Google Scholar]
- Kelly K. A. Anal sphincter-saving operations for chronic ulcerative colitis. Am J Surg. 1992 Jan;163(1):5–11. doi: 10.1016/0002-9610(92)90244-l. [DOI] [PubMed] [Google Scholar]
- Lewis W. G., Holdsworth P. J., Sagar P. M., Holmfield J. H., Johnston D. Effect of anorectal eversion during restorative proctocolectomy on anal sphincter function. Br J Surg. 1993 Jan;80(1):121–123. doi: 10.1002/bjs.1800800139. [DOI] [PubMed] [Google Scholar]
- Lewis W. G., Holdsworth P. J., Stephenson B. M., Finan P. J., Johnston D. Role of the rectum in the physiological and clinical results of coloanal and colorectal anastomosis after anterior resection for rectal carcinoma. Br J Surg. 1992 Oct;79(10):1082–1086. doi: 10.1002/bjs.1800791032. [DOI] [PubMed] [Google Scholar]
- Martin L. W., Torres A. M., Fischer J. E., Alexander F. The critical level for preservation of continence in the ileoanal anastomosis. J Pediatr Surg. 1985 Dec;20(6):664–667. doi: 10.1016/s0022-3468(85)80020-8. [DOI] [PubMed] [Google Scholar]
- Nasmyth D. G., Johnston D., Godwin P. G., Dixon M. F., Smith A., Williams N. S. Factors influencing bowel function after ileal pouch-anal anastomosis. Br J Surg. 1986 Jun;73(6):469–473. doi: 10.1002/bjs.1800730617. [DOI] [PubMed] [Google Scholar]
- Neal D. E., Williams N. S., Johnston D. Rectal, bladder and sexual function after mucosal proctectomy with and without a pelvic reservoir for colitis and polyposis. Br J Surg. 1982 Oct;69(10):599–604. doi: 10.1002/bjs.1800691015. [DOI] [PubMed] [Google Scholar]
- Nicholls R. J., Belliveau P., Neill M., Wilks M., Tabaqchali S. Restorative proctocolectomy with ileal reservoir: a pathophysiological assessment. Gut. 1981 Jun;22(6):462–468. doi: 10.1136/gut.22.6.462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pezim M. E., Pemberton J. H., Dozois R. R. Enteric continence and the ileal pouch-anal procedure. Semin Surg Oncol. 1987;3(2):92–98. doi: 10.1002/ssu.2980030209. [DOI] [PubMed] [Google Scholar]
- Roe A. M., Bartolo D. C., Mortensen N. J. New method for assessment of anal sensation in various anorectal disorders. Br J Surg. 1986 Apr;73(4):310–312. doi: 10.1002/bjs.1800730421. [DOI] [PubMed] [Google Scholar]
- Sagar P. M., Holdsworth P. J., Johnston D. Correlation between laboratory findings and clinical outcome after restorative proctocolectomy: serial studies in 20 patients with end-to-end pouch-anal anastomosis. Br J Surg. 1991 Jan;78(1):67–70. doi: 10.1002/bjs.1800780121. [DOI] [PubMed] [Google Scholar]
- Sagar P. M., Lewis W., Holdsworth P. J., Johnston D. One-stage restorative proctocolectomy without temporary defunctioning ileostomy. Dis Colon Rectum. 1992 Jun;35(6):582–588. doi: 10.1007/BF02050540. [DOI] [PubMed] [Google Scholar]