

Abstract
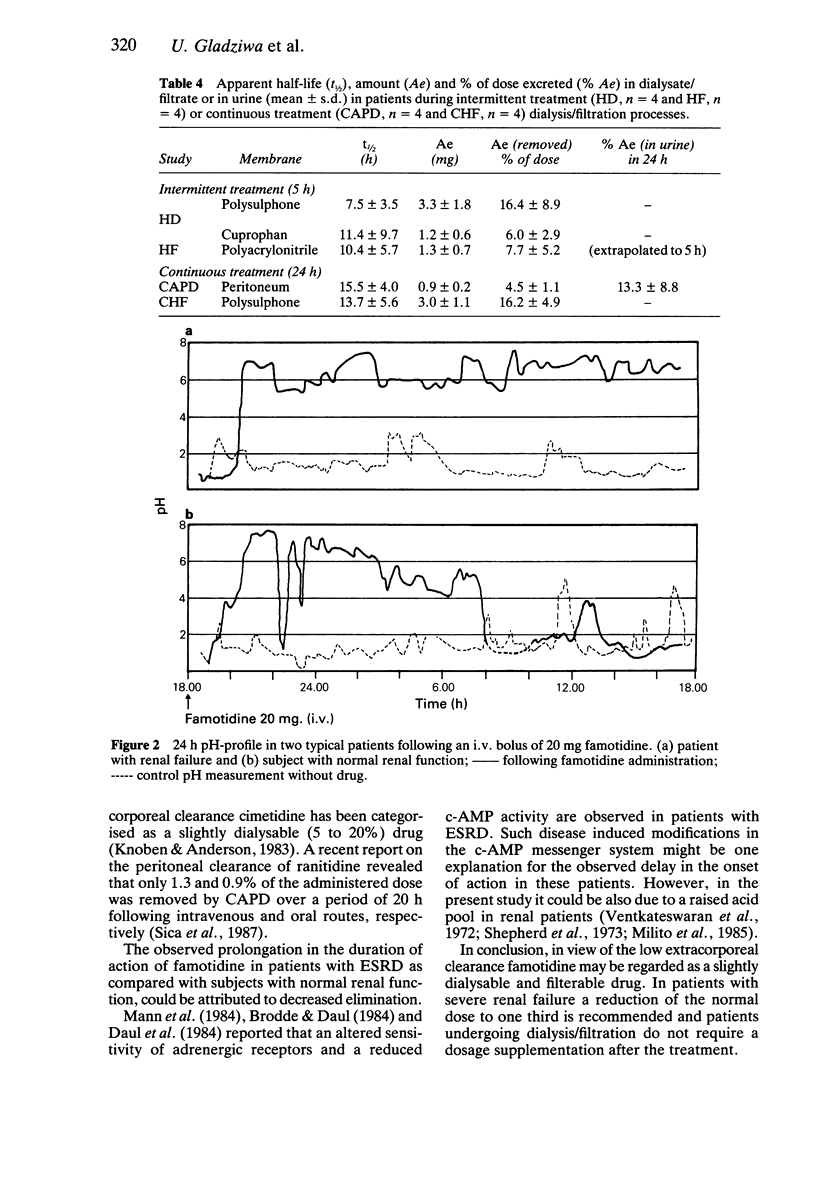
1. Famotidine, a new histamine H2-receptor antagonist was administered intravenously (20 mg) to 22 patients with end stage renal disease during a dialysis free interval (n = 6) and during different blood purification processes including haemodialysis (HD; n = 4), intermittent haemofiltration (HF; n = 4), continuous haemofiltration (CHF; n = 4) and continuous ambulatory peritoneal dialysis (CAPD; n = 4). The plasma, the dialysate/filtrate and the urine concentrations of famotidine were analysed by h.p.l.c. 2. In addition, intra-gastric pH was measured by a long-term-pH probe in seven patients with renal failure and in six patients with normal renal function (control group) following 20 mg famotidine. 3. A 7 to 10 fold prolongation of famotidine's elimination half-life (27.2 +/- 8.5 h; mean +/- s.d.) was observed in patients with renal failure as compared with the half-life (2.6-3.6 h) in subjects with normal renal function. 4. Total body clearance (CL) and volume of distribution (V) were found to be 33.5 +/- 10.1 ml min-1 and 1.3 +/- 0.7 l kg-1, respectively in patients with end-stage renal failure. 5. Blood purification processes have shown considerable variation in clearing famotidine from the body: 16.4 +/- 8.9 and 6.0 +/- 2.9% of the administered dose in HD with polysulphone and cuprophan membranes respectively, 7.7 +/- 5.2% in HF with a polyacrylonitrile membrane (each for 5 h), 4.5 +/- 1.1% in CAPD and 16.2 +/- 4.9% in CHF with a polysulphone membrane within 24 h.(ABSTRACT TRUNCATED AT 250 WORDS)
Full text
PDF
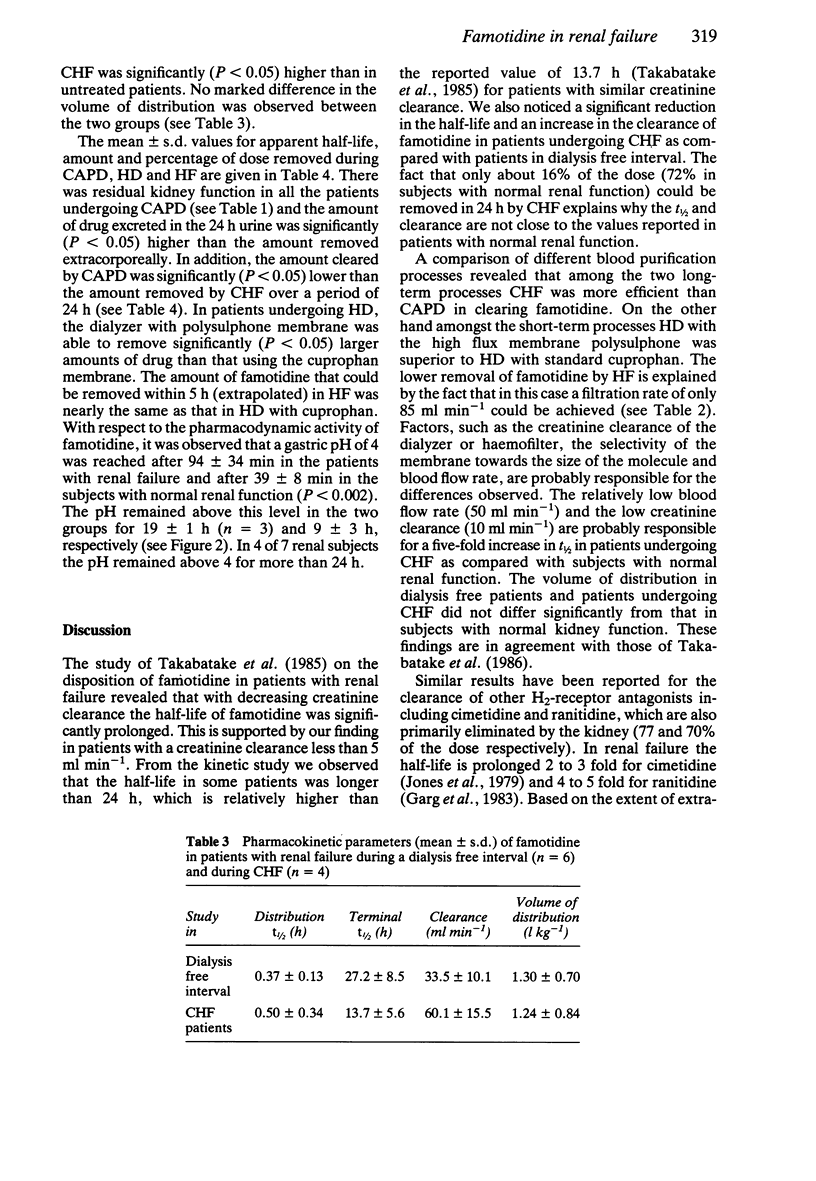
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Brodde O. E., Daul A. Alpha- and beta-adrenoceptor changes in patients on maintenance hemodialysis. Contrib Nephrol. 1984;41:99–107. doi: 10.1159/000429270. [DOI] [PubMed] [Google Scholar]
- Daul A. E., Khalifa A. M., Graven N., Brodde O. E. Impaired regulation of beta-adrenoceptors in patients on maintenance haemodialysis. Proc Eur Dial Transplant Assoc Eur Ren Assoc. 1985;21:178–184. [PubMed] [Google Scholar]
- Garg D. C., Weidler D. J., Eshelman F. N. Ranitidine bioavailability and kinetics in normal male subjects. Clin Pharmacol Ther. 1983 Apr;33(4):445–452. doi: 10.1038/clpt.1983.60. [DOI] [PubMed] [Google Scholar]
- Goldstein H., Murphy D., Sokol A., Rubini M. E. Gastric acid secretion in patients undergoing chronic dialysis. Arch Intern Med. 1967 Dec;120(6):645–653. [PubMed] [Google Scholar]
- Jones R. H., Lewin M. R., Parsons V. Therapeutic effect of cimetidine in patients undergoing haemodialysis. Br Med J. 1979 Mar 10;1(6164):650–652. doi: 10.1136/bmj.1.6164.650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kroemer H., Klotz U. Pharmacokinetics of famotidine in man. Int J Clin Pharmacol Ther Toxicol. 1987 Aug;25(8):458–463. [PubMed] [Google Scholar]
- Mann J. F., Hausen M., Jacobs K. H., Kutter A., Nagel W., Rascher W., Schick M., Sudhoff R., Ritz E. Adrenergic responsiveness in experimental uremia. Contrib Nephrol. 1984;41:108–112. doi: 10.1159/000429271. [DOI] [PubMed] [Google Scholar]
- Milito G., Taccone-Gallucci M., Brancaleone C., Nardi F., Filingeri V., Cesca D., Casciani C. U. Assessment of the upper gastrointestinal tract in hemodialysis patients awaiting renal transplantation. Am J Gastroenterol. 1983 Jun;78(6):328–331. [PubMed] [Google Scholar]
- Peck C. C., Barrett B. B. Nonlinear least-squares regression programs for microcomputers. J Pharmacokinet Biopharm. 1979 Oct;7(5):537–541. doi: 10.1007/BF01062394. [DOI] [PubMed] [Google Scholar]
- Ritz E., Krempien B., Wanke M., Ziegler M., Wesch G., Torner U. KLinische und experimentelle Untersuchungen zur urämischen Gastritis. Verh Dtsch Ges Inn Med. 1971;77:220–224. [PubMed] [Google Scholar]
- Shepherd A. M., Stewart W. K., Wormsley K. G. Peptic ulceration in chronic renal failure. Lancet. 1973 Jun 16;1(7816):1357–1359. doi: 10.1016/s0140-6736(73)91677-2. [DOI] [PubMed] [Google Scholar]
- Sica D. A., Comstock T., Harford A., Eshelman F. Ranitidine pharmacokinetics in continuous ambulatory peritoneal dialysis. Eur J Clin Pharmacol. 1987;32(6):587–591. doi: 10.1007/BF02455993. [DOI] [PubMed] [Google Scholar]
- Takabatake T., Ohta H., Maekawa M., Yamamoto Y., Ishida Y., Hara H., Nakamura S., Ushiogi Y., Kawabata M., Hashimoto N. Pharmacokinetics of famotidine, a new H2-receptor antagonist, in relation to renal function. Eur J Clin Pharmacol. 1985;28(3):327–331. doi: 10.1007/BF00543332. [DOI] [PubMed] [Google Scholar]
- Ventkateswaran P. S., Jeffers A., Hocken A. G. Gastric acid secretion in chronic renal failure. Br Med J. 1972 Oct 7;4(5831):22–23. doi: 10.1136/bmj.4.5831.22. [DOI] [PMC free article] [PubMed] [Google Scholar]