

Abstract
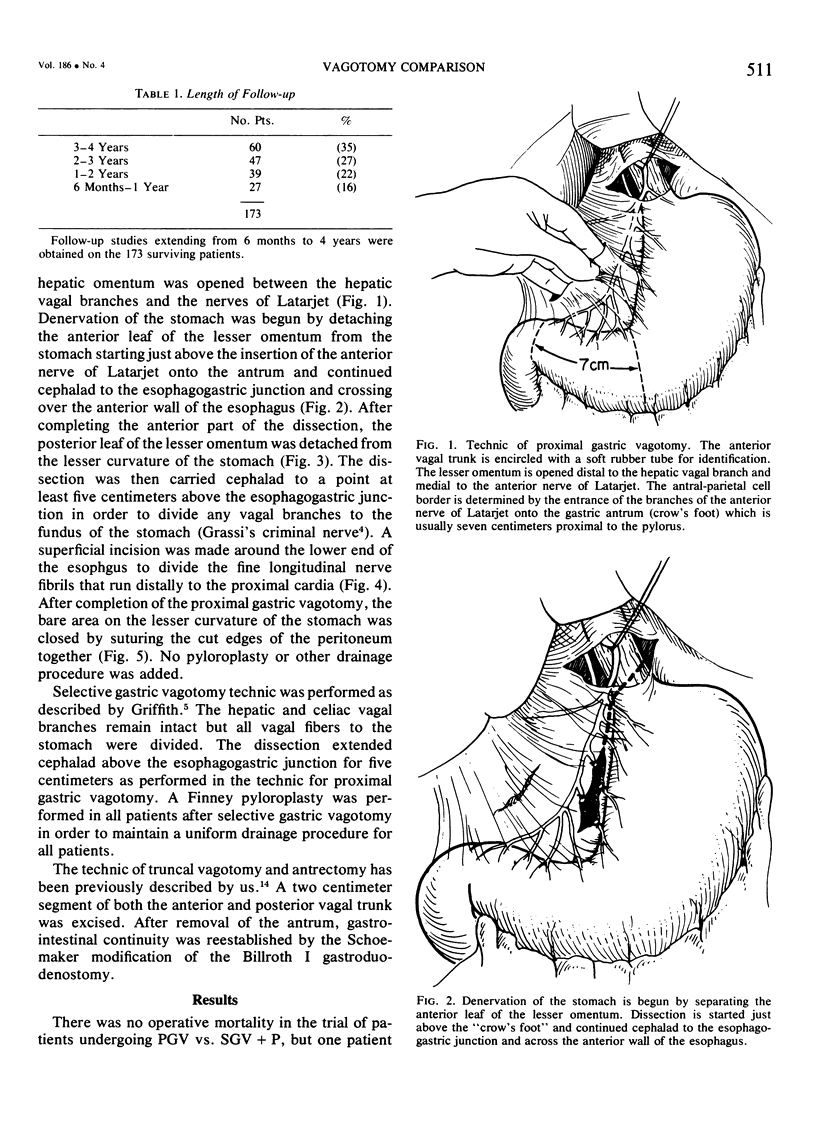
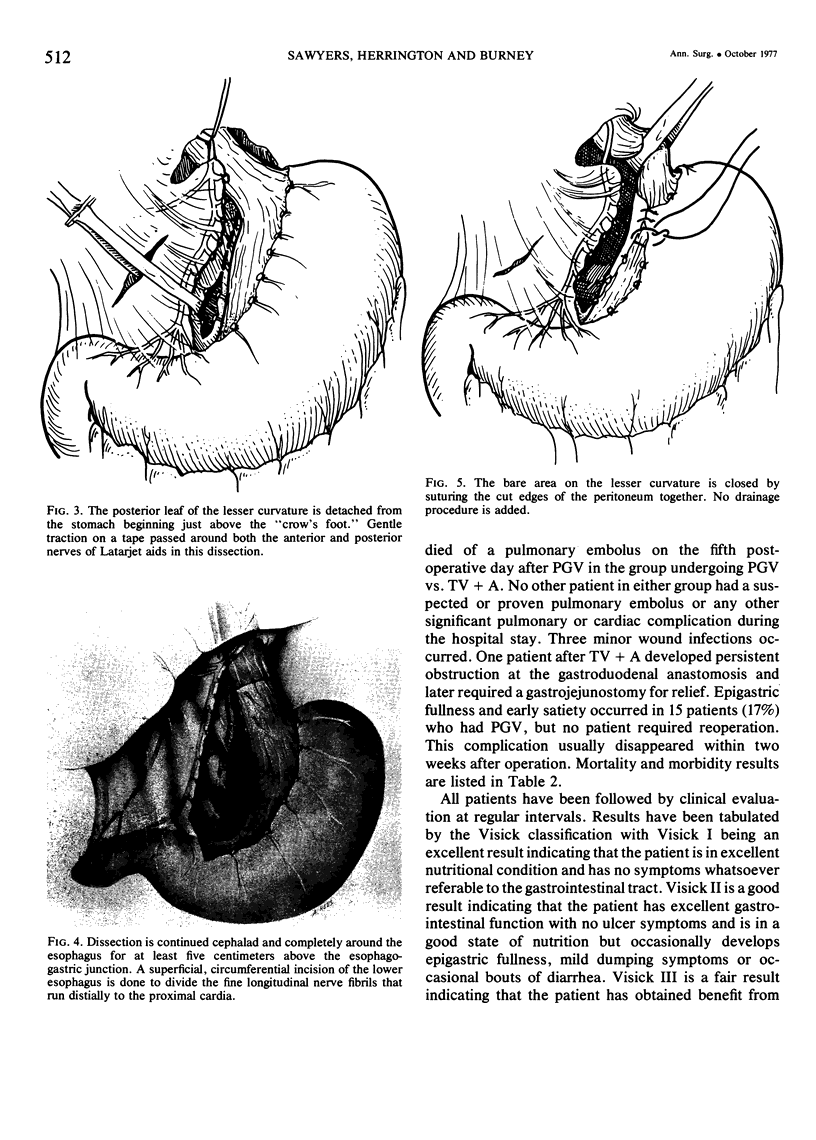
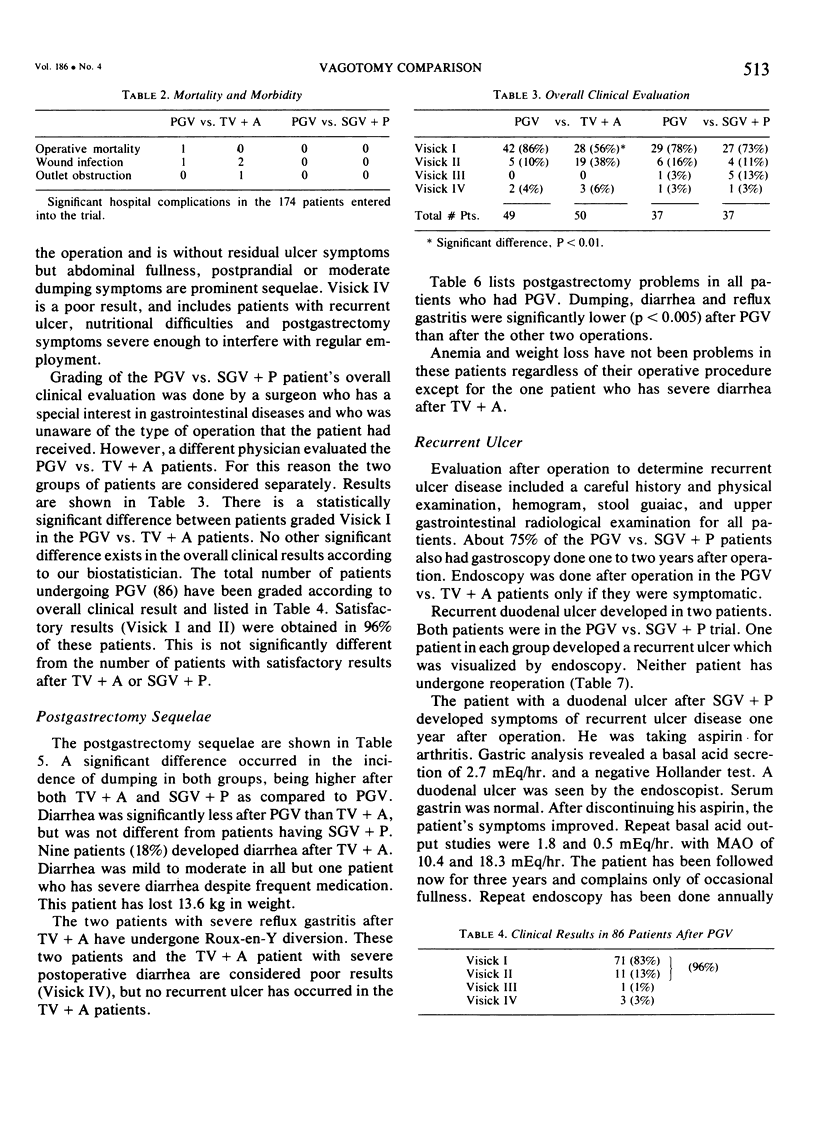
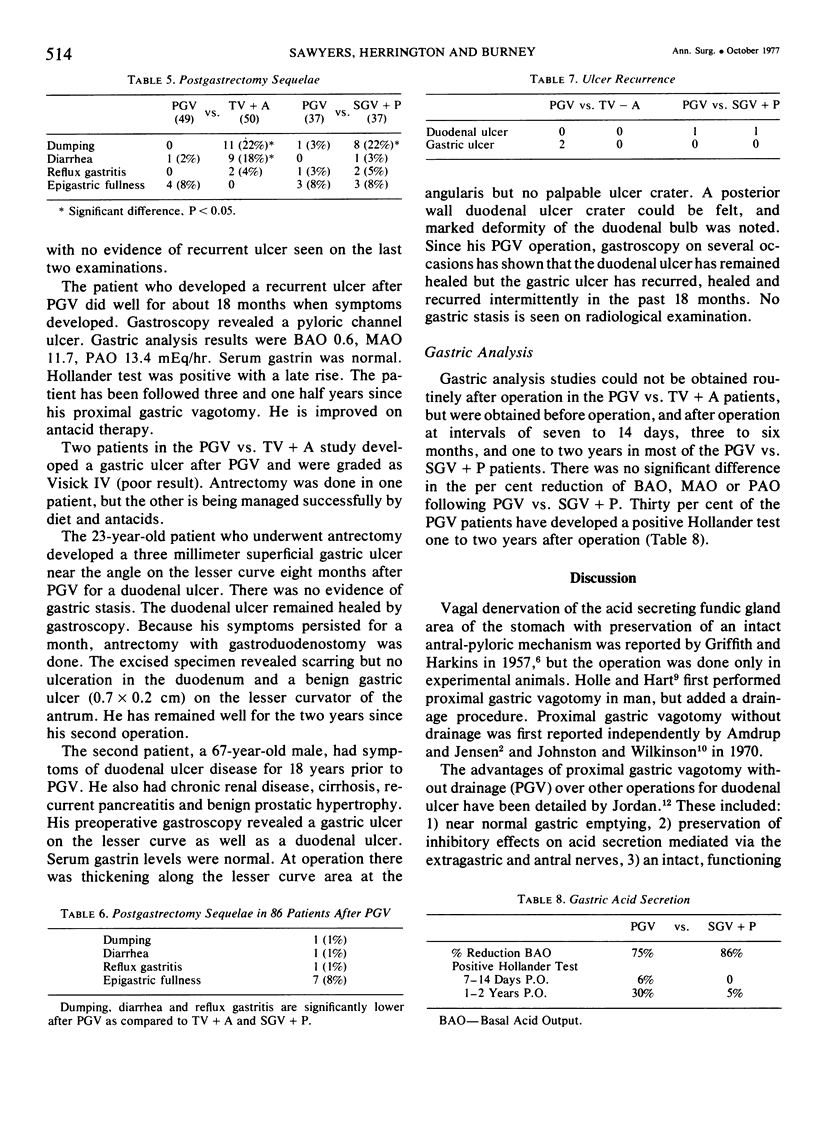
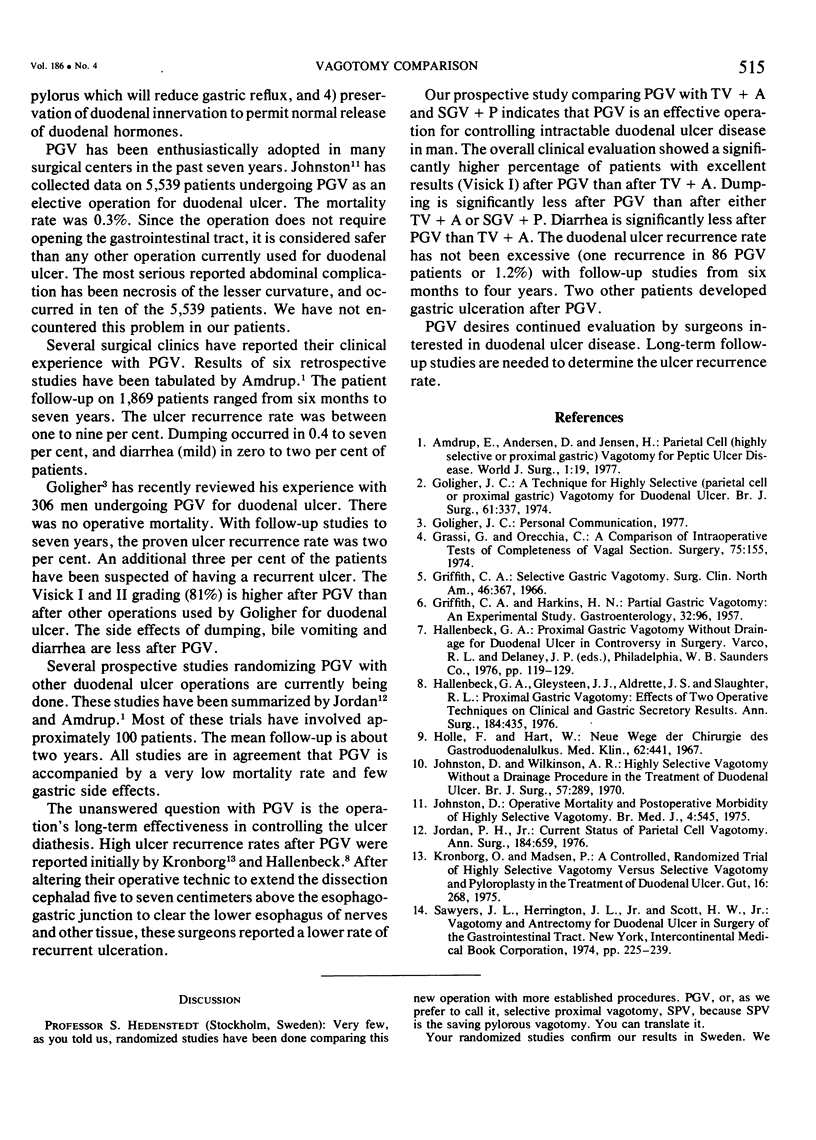
A prospective, randomized study of proximal gastric vagotomy without drainage (PGV) was done in 174 adult men with chronic duodenal ulcer intractable to medical therapy. PGV was randomized against truncal vagotomy with antrectomy (TV + A) and against selective gastric vagotomy with Finney pyloroplasty (SGV + P). Postgastrectomy sequelae (dumping, diarrhea and reflux gastritis) were less after PGV. One patient after PGV developed a recurrent ulcer as did one patient after SGV + P. Two patients developed gastric ulcers after PGV. Good to excellent results (Visick I and II) were obtained in 96% of patients with PGV, 94% with TV + A and 86% with SGV + P. Follow-up studies were from six months to four years.
Full text
PDF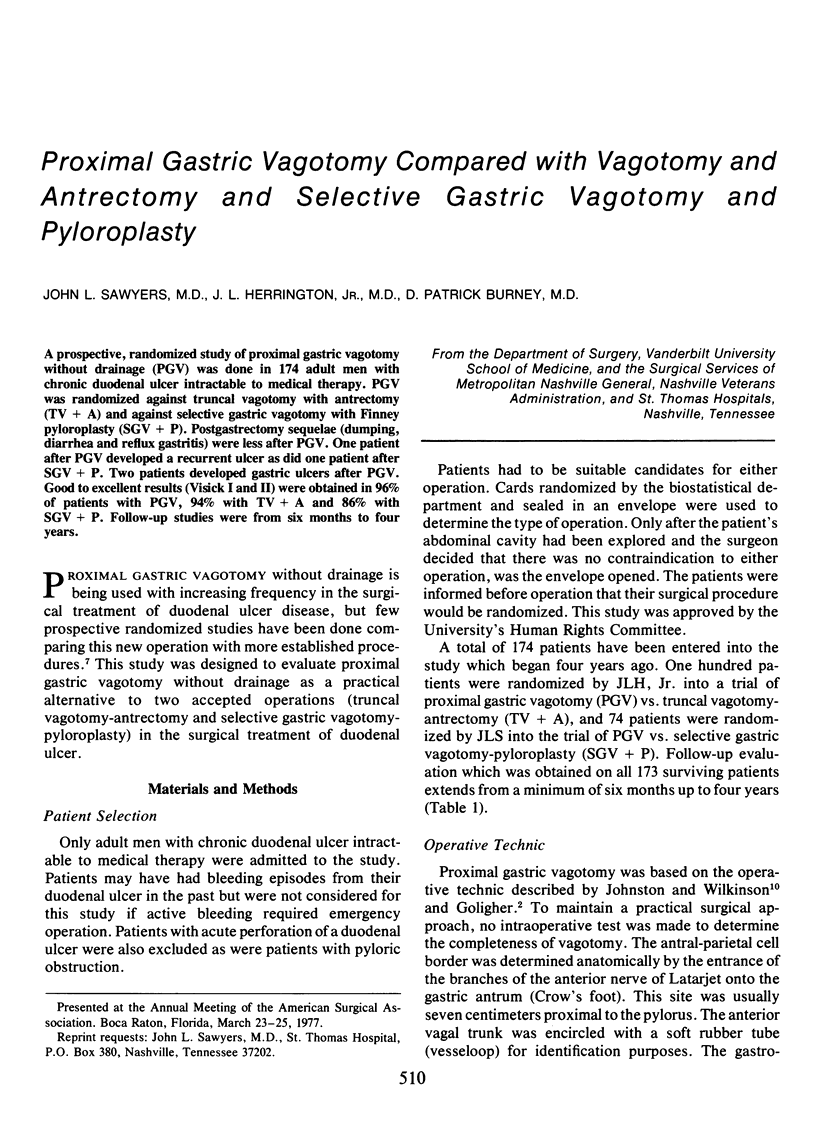
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Amdrup E., Andersen D., Jensen H. E. Parietal cell (highly selective or proximal gastric) vagotomy for peptic ulcer disease. World J Surg. 1977 Jan;1(1):19–25. doi: 10.1007/BF01654722. [DOI] [PubMed] [Google Scholar]
- GRIFFITH C. A., HARKINS H. N. Partial gastric vagotomy: an experimental study. Gastroenterology. 1957 Jan;32(1):96–102. [PubMed] [Google Scholar]
- Goligher J. C. A technique for highly selective (parietal cell or proximal gastric) vagotomy for duodenal ulcer. Br J Surg. 1974 May;61(5):337–345. doi: 10.1002/bjs.1800610502. [DOI] [PubMed] [Google Scholar]
- Grassi G., Orecchia C. A comparison of intraoperative tests of completeness of vagal section. Surgery. 1974 Feb;75(2):155–160. [PubMed] [Google Scholar]
- Griffith C. A. Selective gastric vagotomy. Surg Clin North Am. 1966 Apr;46(2):367–377. doi: 10.1016/s0039-6109(16)37839-2. [DOI] [PubMed] [Google Scholar]
- Hallenbeck G. A., Gleysteen J. J., Aldrete J. S., Slaughter R. L. Proximal gastric vagotomy: effects of two operative techniques on clinical and gastric secretory results. Ann Surg. 1976 Oct;184(4):435–442. doi: 10.1097/00000658-197610000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holle F., Hart W. Neue Wege der Chirurgie des Gastroduodenalulkus. Med Klin. 1967 Mar 24;62(12):441–450. [PubMed] [Google Scholar]
- Johnston D. Operative mortality and postoperative morbidity of highly selective vagotomy. Br Med J. 1975 Dec 6;4(5996):545–547. doi: 10.1136/bmj.4.5996.545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston D., Wilkinson A. R. Highly selective vagotomy without a drainage procedure in the treatment of duodenal ulcer. Br J Surg. 1970 Apr;57(4):289–296. doi: 10.1002/bjs.1800570414. [DOI] [PubMed] [Google Scholar]
- Jordan P. H., Jr Current status of parietal cell vagotomy. Ann Surg. 1976 Dec;184(6):659–671. doi: 10.1097/00000658-197612000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kronborg O., Madsen P. A controlled, randomized trial of highly selective vagotomy versus selective vagotomy and pyloroplasty in the treatment of duodenal ulcer. Gut. 1975 Apr;16(4):268–271. doi: 10.1136/gut.16.4.268. [DOI] [PMC free article] [PubMed] [Google Scholar]