

Abstract
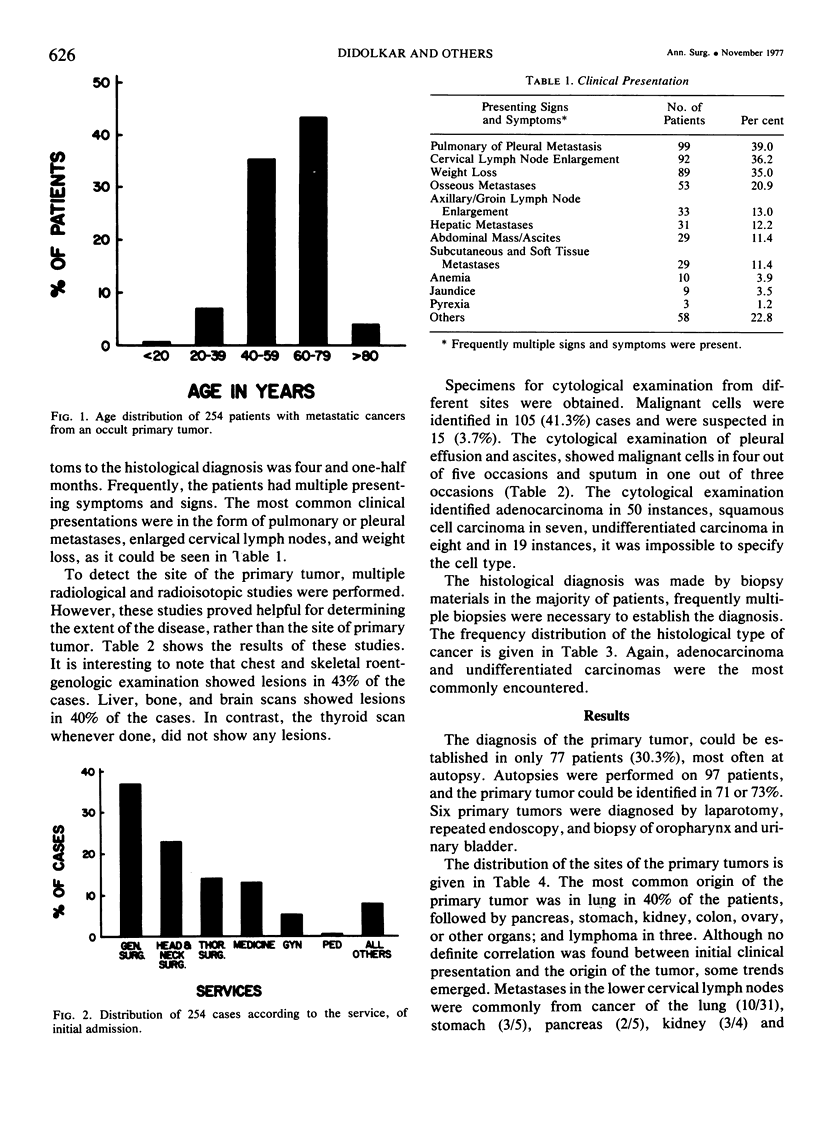
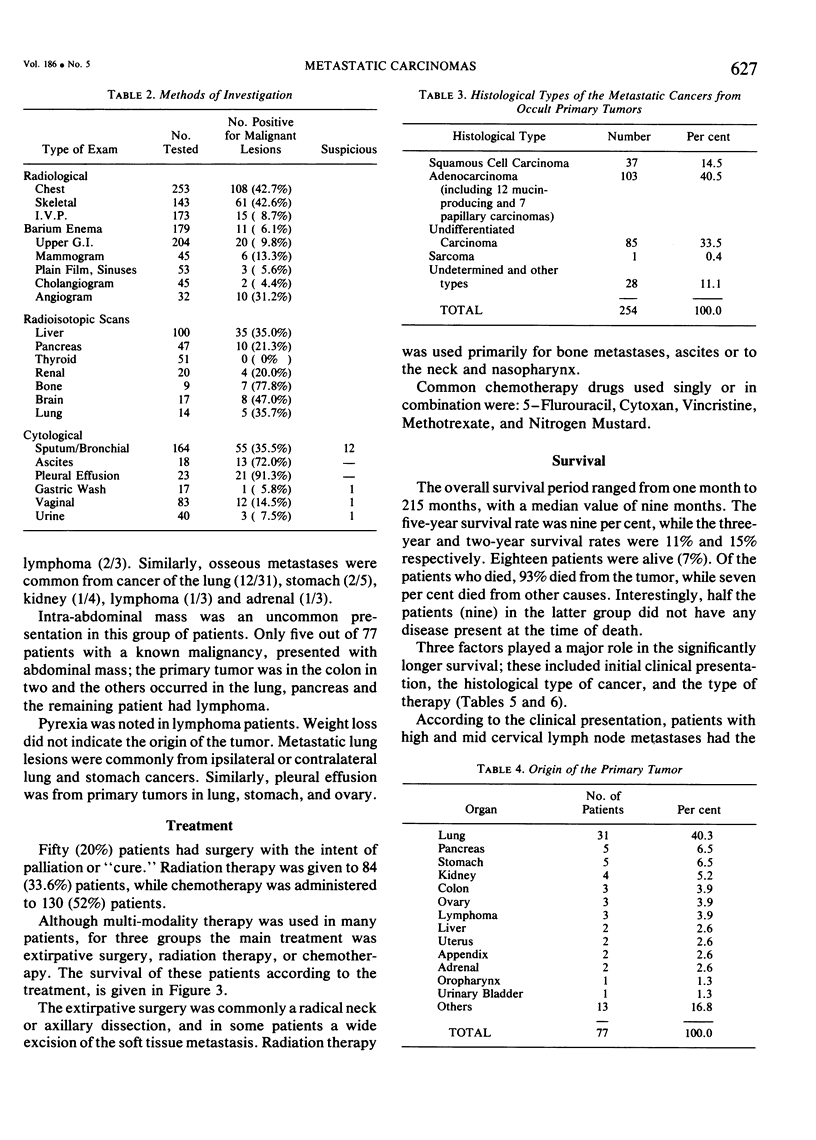
From 1950 to 1973, 254 patients with metastatic cancers from occult primary tumors, comprising 0.5% of all the referred cancer patients were seen. The average age was 59 years. Clinical presentation was commonly in the form of metastatic lesions in lung, cervical lymph node, bone or liver. Radiological and radioisotopic investigations proved helpful in determining the extent of disease rather than the origin of primary tumor. Adenocarcinoma was the commonest type, followed by undifferentiated and squamous cell carcinomas. The origin of the primary tumor was established in 77 (30%) patients, mostly at autopsy. It was in the lung in 40% of the cases, followed by stomach, pancreas, kidney, ovary and colon. Some correlation was found between clinical presentation and the origin of the primary tumor. Histologically different second cancers were detected in 28 (11%) patients. Overall median and five-year survival rates were nine months and nine per cent respectively. Longer survival was seen in patients with squamous cell carcinoma metastases, middle and upper neck lymph node lesions, and those who had “curative” surgery. In localized metastatic lesions, surgical extirpation should be done. Depending on the histological type of the metastatic lesions, chemotherapy and/or radiation therapy have definite roles in the management of these patients. Periodic follow-up examinations also prove valuable.
Full text
PDF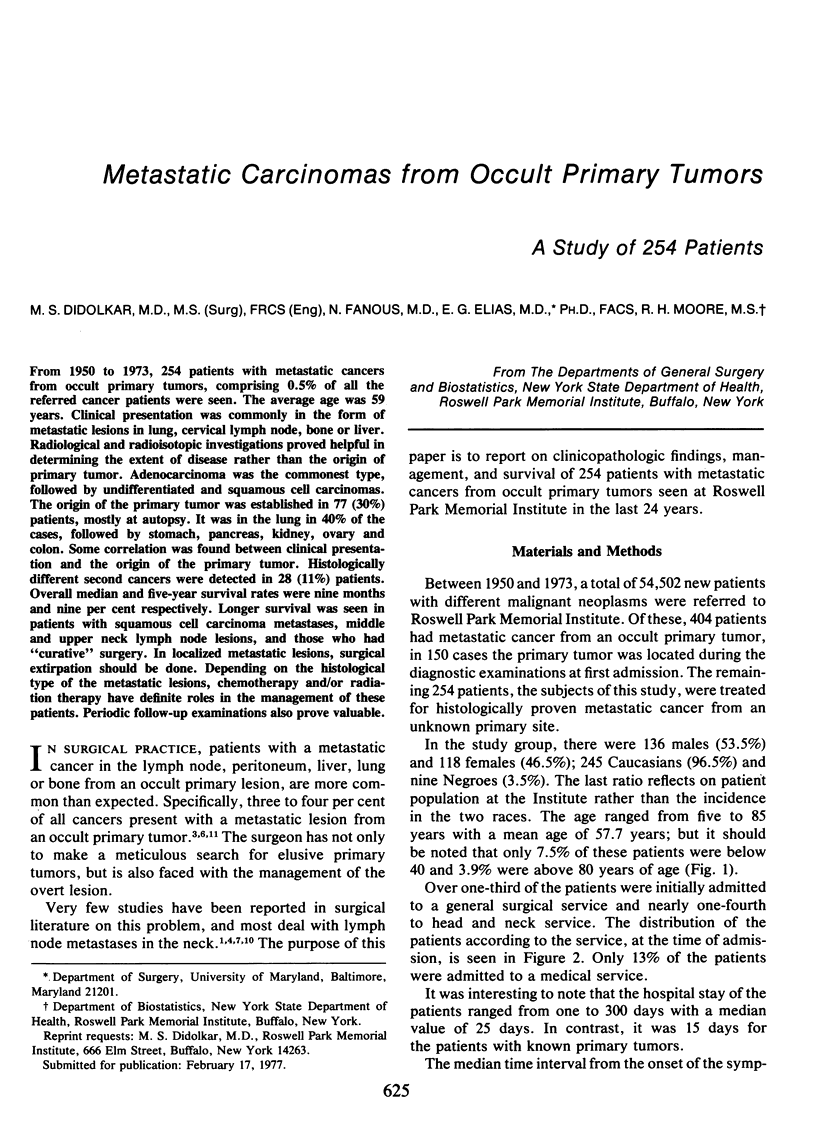
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Batsakis J. G., McBurney T. A. Metastatic neoplasms to the head and neck. Surg Gynecol Obstet. 1971 Oct;133(4):673–677. [PubMed] [Google Scholar]
- Holmes F. F., Fouts T. L. Metastatic cancer of unknown primary site. Cancer. 1970 Oct;26(4):816–820. doi: 10.1002/1097-0142(197010)26:4<816::aid-cncr2820260413>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- JOHNSON R. O., CASTRO R., ANSFIELD F. J. RESPONSE OF PRIMARY UNKNOWN CANCERS TO TREATMENT WITH 5-FLUOROURACIL (NSC-19893). Cancer Chemother Rep. 1964 May;38:63–64. [PubMed] [Google Scholar]
- Jesse R. H., Perez C. A., Fletcher G. H. Cervical lymph node metastasis: unknown primary cancer. Cancer. 1973 Apr;31(4):854–859. doi: 10.1002/1097-0142(197304)31:4<854::aid-cncr2820310414>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- Lleander V. C., Goldstein G., Horsley J. S., 2nd Chemotherapy in the management of metastatic cancer of unknown primary site. Oncology. 1972;26(2):265–270. doi: 10.1159/000224675. [DOI] [PubMed] [Google Scholar]
- MARCHETTA F. C., MURPHY W. T., KOVARIC J. J. CARCINOMA OF THE NECK. Am J Surg. 1963 Dec;106:974–979. doi: 10.1016/0002-9610(63)90166-1. [DOI] [PubMed] [Google Scholar]
- Moertel C. G., Reitemeier R. J., Schutt A. J., Hahn R. G. Treatment of the patient with adenocarcinoma of unknown origin. Cancer. 1972 Dec;30(6):1469–1472. doi: 10.1002/1097-0142(197212)30:6<1469::aid-cncr2820300609>3.0.co;2-t. [DOI] [PubMed] [Google Scholar]
- Roth J. A., Silverstein M. J., Morton D. L. Metastatic potential of metastases. Surgery. 1976 Jun;79(6):669–673. [PubMed] [Google Scholar]
- Smith P. E., Krementz E. T., Chapman W. Metastatic cancer without a detectable primary site. Am J Surg. 1967 May;113(5):633–637. doi: 10.1016/0002-9610(67)90309-1. [DOI] [PubMed] [Google Scholar]
- Templeton A. C. Tumours of unknown origin. Recent Results Cancer Res. 1973;41:302–305. doi: 10.1007/978-3-642-80725-1_18. [DOI] [PubMed] [Google Scholar]